Article Text

Abstract
Background/aims To assess epidemiological tumour features, risk factors, clinical management and outcome of eyelid squamous cell carcinoma (SCC) and changes thereof. Furthermore, we searched for validating predictors of the American Joint Committee on Cancer (AJCC) 8 classification system.
Methods We evaluated data of 117 patients with histologically proven eyelid SCC at a large tertiary German university centre between January 2009 and March 2020. This retrospective, monocentric analysis included descriptive statistics and non-parametric tests (p<0.05).
Results Histologically controlled excision and follow-up was performed in 88 (75.2%) patients. In the remaining patients with higher T-category, individual adjuvant therapy combinations were initiated. We found higher numbers of nodal metastasis and recurrence for male patients and higher T-category (p=0.035, p=0.008 and p=0.001, p<0.001). Recurrence rates proved higher for patients with multiple lesions (p=0.008). Disease-specific survival (DSS) was 95.7% at 2 and 94.9% at 5 years of follow-up. Six patients (5.1%) died from eyelid SCC with nodal metastasis and higher T-category being negative prognostic factors (p<0.001 and p=0.009). Mortality was associated with tumour location in the medial upper eyelid, nodal metastasis being more frequent (p=0.001 and p=0.009) and tumour of the lower eyelid alone as positive predictor (p=0.012). T category differed in 34 (29.1%) patients when comparing AJCC 7 and 8 (p<0.001). Changes in T category as per the AJCC 8 classification resulted in better prediction of DSS (p=0.024).
Conclusion Special attention should be paid to male patients, tumour location in the upper medial eyelid and lymph node diagnostics. Prediction of DSS proved superior as per the AJCC 8 staging system.
- epidemiology
- eye lids
- neoplasia
Data availability statement
Deidentified participant data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Although the incidence of eyelid squamous cell carcinoma (SCC) is low (eg, 0.09–2.42 cases per 100.000 population),1 it is reportedly the second most common malignancy of the eyelid,2 accounting for 5%–10% of all eyelid malignancies.3 Eyelid SCC patients treated early in time have an excellent prognosis, but advanced tumour stages may result in the need of orbital exenteration or even cause mortality due to systemic metastasis.
Inaccuracy of preoperative clinical diagnosis, even by experienced examiners, has been reported for eyelid SCC.4 5 As clinical presentation may vary greatly, histological workup is required for accurate diagnosis in suspicious lesions. Generally, microscopic controlled excision is recommended for treatment of periocular basal cell carcinoma and SCC and low recurrence rates have thus been obtained.6
There are reported negative predictive factors for recurrence of eyelid SCC such as chronic immunosuppression in the literature.3 7 8 A precise staging system alongside histological workup would be invaluable for better prediction of tumour relapse and disease-specific survival (DSS).
The American Joint Committee on Cancer (AJCC) Staging Manual, eighth edition (AJCC 8), was introduced in 2016 and includes significant changes in definitions of T and N categories.9 10 For AJCC 7, Nasser et al reported that clinical stage T2b or worse was associated with an elevated risk of nodal metastasis.11 First reports to validate the AJCC 8 staging system have been published including patients with different eyelid cancers12 as well as a study including 109 US American patients with eyelid SCC in particular.13 These publications reported a high rate of difference between both classification systems (75%12 and 30.3%,13 respectively). AJCC 8 staging criteria seem to result in better prediction of DSS.13
In the present study, we retrospectively analysed eyelid SCC tumour and patient characteristics, tumour risk factors, patient management and outcome as well as possible changes of these factors over time for 117 consecutive patients that were referred to our large German tertiary University centre over a period of over 11 years. Additionally, following the example of the first US American validation studies for AJCC 8 staging,12 13 we analysed staging differences between AJCC 7 and AJCC 8 and possible correlation with DSS as more studies from different regions need to be conducted in order to further validate these important previous findings.
Material and methods
Patients were identified by searching for the diagnosis ‘eyelid SCC’ in the departmental histopathology database for inclusion in this retrospective, monocentric, observational study. Patients were histologically diagnosed with eyelid SCC between January 2009 and March 2020. Clinical data were completed from the original patient files.
Data collected included tumour extent (including largest tumour diameter in mm as well as additional conjunctival, perineural and orbital invasion) and staging, last follow-up as well as disease mortality. Eyelid SCCs were classified by pathological TNM (primary tumour, lymph node, distant metastasis)-staging of carcinoma of the eyelid as per the seventh or as per the eighth edition AJCC Staging Manual9 10 depending on the time of diagnosis and retrospectively according to both systems for the comparative purpose of the study. Potential confounders included patient gender (female or male), patient age at diagnosis, time from first symptoms to diagnosis, lesion laterality (right or left eye, both eyes), best-corrected visual acuity (BCVA) (log(MAR)), predisposing factors for development of SCC such as systemic immunosuppression, chronic blepharitis/neurodermitis or multiple lesions, adjuvant tumour therapy and disease recurrence.
A detailed photodocumentation had been performed of the patients’ face in primary position as well as a tumour close-up in a well-lit room for all patients prior to biopsy or complete excision with histological confirmation of tumour clearance.
Histopathology findings were extracted from the original reports. The vast majority of lesions were treated by primary surgical excision, while some were biopsied by the referring practitioner before definitive excision at our institution. Tumour excision was performed by histologically controlled excision examining the excision margins microscopically for remaining tumour cells until all tumourous cells had been removed. Histopathological assessment was performed by a certified ocular Histopathologist after formalin-fixation, paraffin embedding, sectioning and staining with haematoxylin and eosin, periodic acid-Schiff staining and immunohistology when necessary.
Statistical data collection was performed using Microsoft Excel (Microsoft Corporation, Redmond, Washington, USA) for Mac 2011. Data analysis was performed with SPSS V.25.0 (IBM Corporation, Armonk, New York, USA). Descriptive statistics, χ2 test or Fisher’s exact test, Kruskal-Wallis-analysis, Mann-Whitney U test and Kaplan-Meier analysis were employed to assess the patients’ clinical and functional data. To avoid bias when restaging with the seventh or eighth edition AJCC Staging Manual by evaluating clinical, histopathological data and photography, respective histopathology and clinical data were first recorded separately and combined for analysis only after completion of the data collection process. Statistical significance of differences was accepted for p<0.05 in two-tailed tests. As all statistical procedures are of exploratory nature, no adjustment for multiple testing has been made.
Results
Demographic data
Analysis was completed in 117 patients with histologically proven eyelid SCC (n=114, 97.4%) or eyelid in situ carcinoma (n=3, 2.6%). Patients’ tumour TNM staging is elaborated in table 1.
Tumour staging by the seventh and eighth edition of the AJCC cancer staging manual
Out of nine patients with nodal metastasis, six (66.6%) presented with nodal metastasis at presentation and three (33.3%) developed lymph node invasion throughout follow-up. Patient numbers and detailed T-staging (AJCC Staging eighth edition) from 2009 to March 2020 are shown in figure 1.

Frequency of eyelid SCCs and tumour T-category per year (2009–03/2020). SCC, squamous cell carcinoma.
Fifty-five (47.0%) patients were female, and 62 (53.0%) male. Respective mean, median and range of age at tumour diagnosis were 73.7, 74.8 and 28–95 years. The tumour was located on the right side in 57 (48.7%) and on the left side in 60 (51.3%) patients. Mean BCVA of the symptomatic eye (log(MAR)) was 0.3 (range 0–2.1). Time from onset of clinical symptoms to diagnosis was mean 6, median 4 and range 0–48 months. Two patients developed recurrent disease (1.7%) after primary excision in our clinic and were treated with further resection, whereas 20 (17.1%) patients were referred to the clinic with suspicious lesions after previous therapy without histologically controlled excision by their treating practitioner (for evaluation of predictive factors, these patients were recorded with tumour recurrence). Known risk factors for the development of eyelid SCC were systemic immunosuppression (n=8, 6.8%, status postheart transplantation and lung transplantation in one patient, 0.9%, respectively), chronic blepharitis/allergic diathesis including neurodermitis in 9 (7.7%) patients and pre-existent solar elastosis (n=4, 3.4%)). Four patients (3.4%) had a history of associated actinic keratosis. History of at least one further (pre) cancerous skin lesion on the body was present in 32 (27.4%) patients (table 2).
Histology of previous (pre)cancerous lesions in 32 patients
Cutaneous eyelid SCC was accompanied by conjunctival SCC in 6 (5.1%) patients with multilocular lesions. Perineural invasion was present in 13 (11.1%) cases.
Patient management
Tumour management included histologically controlled excision only and follow-up in 88 (75.2%) patients. For the remaining 29 patients, a plethora of adjuvant therapy combinations was applied following our tumour board decision and is listed in table 3.
Tumour treatment strategies
One patient underwent radiotherapy only and one patient received palliative treatment only; both of these T4b tumours were considered inoperable by our interdisciplinary tumour board.
Prognostic factors
Negative prognostic factors in terms of survival included histopathological spread to the local lymph nodes and higher tumour T-category (p<0.001 and p=0.009; Fisher’s exact test).
In terms of gender analysis, we recorded significantly higher numbers of lymph node invasion and recurrence for male patients (p=0.035, p=0.008). Higher tumour T-category was also associated with higher numbers of lymph node invasion and recurrence (p=0.001, p<0.001; Fisher’s exact test for all cases). Recurrence rates proved significantly higher for patients that presented with multiple lesions (p=0.008; Fisher’s exact test).
Frequency of tumour location was 60 (51.3%) in the lower and 26 (22.2%) in the upper lid only, 22 (18.8%) in the medial and 12 (10.3%) in the lateral canthal region. Three patients had tumour infiltration of the medial and lateral canthal region due to vast tumour extension. Patients with tumour location in the medial upper eyelid including the medial canthal region (n=41 (35.0%)), had an elevated disease-specific mortality (p=0.001; Fisher’s exact test). Additionally, lymph node invasion was significantly more frequent in tumours situated in the medial upper eyelid (p=0.009; Fisher’s exact test) whereas tumour location in the lower eyelid alone was a significant positive predictor (n=60 (51.3%), p=0.012; Fisher’s exact test).
Patient survival
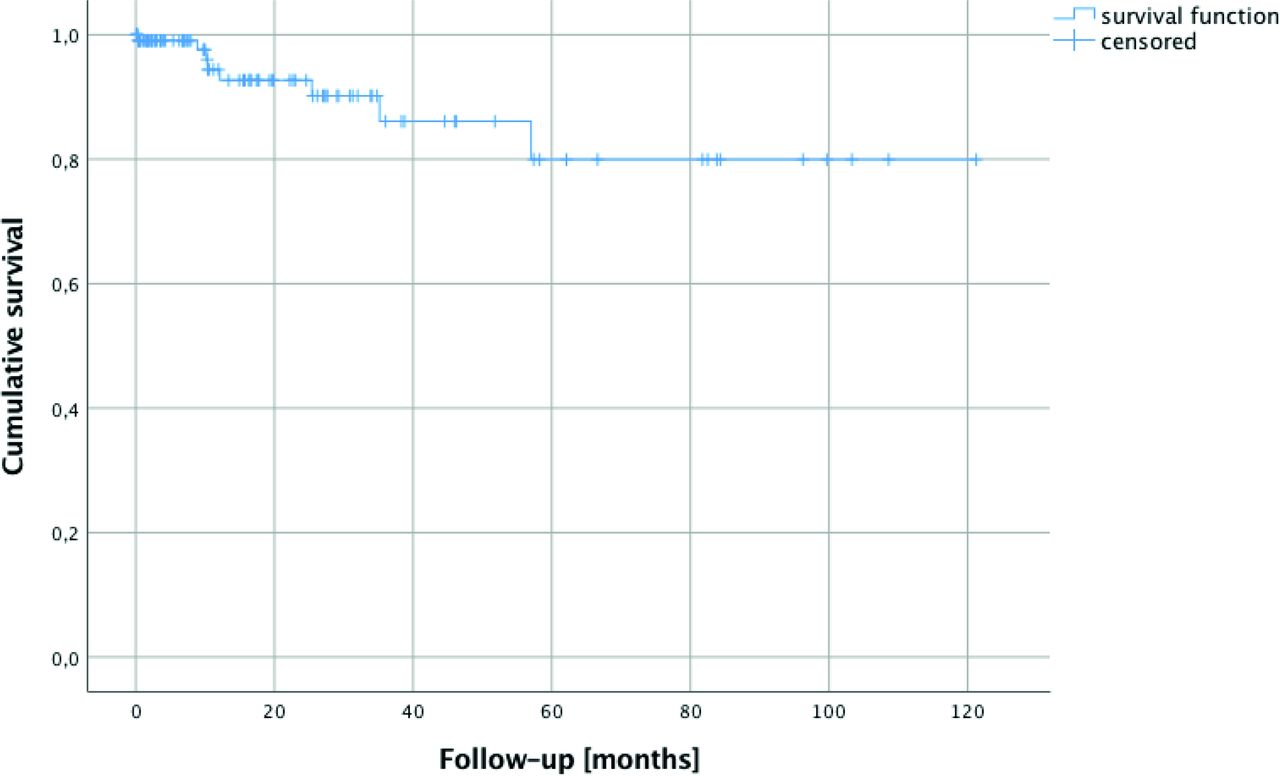
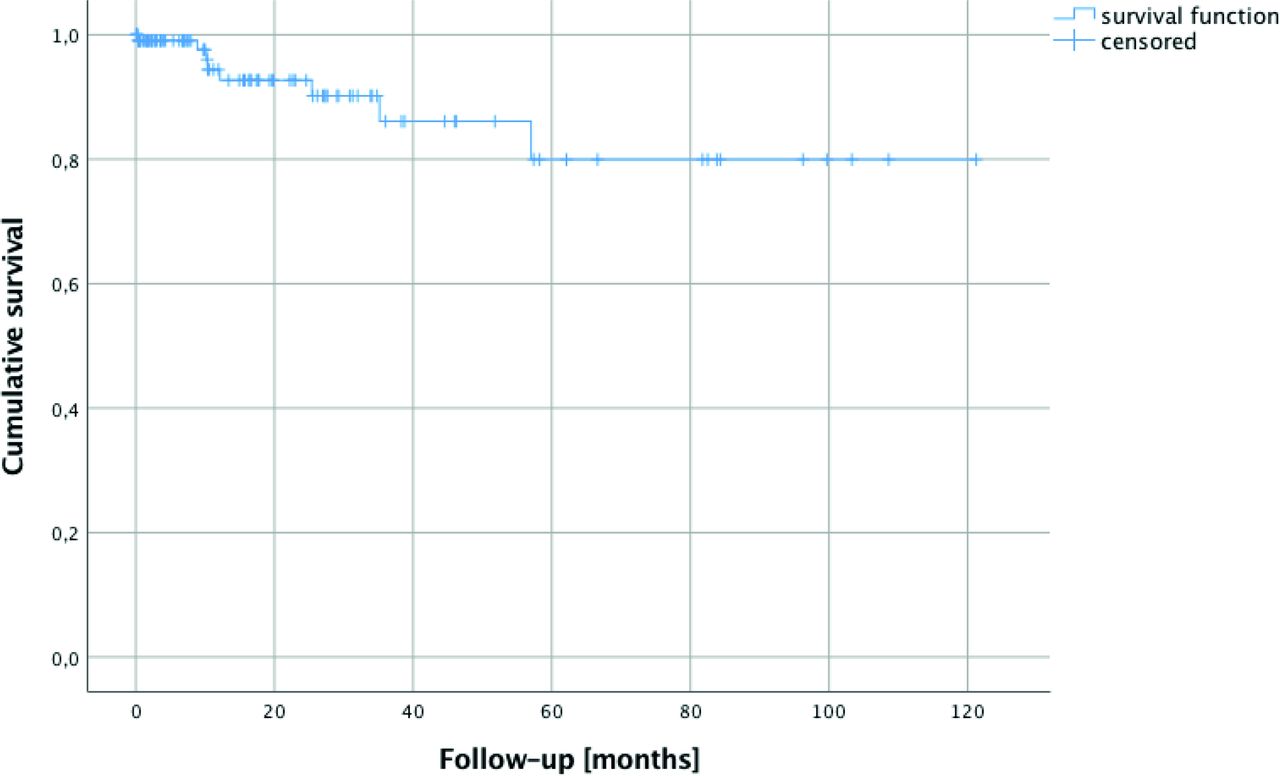
Eight patients died during a follow-up period of 0–121 months of the complete cohort (median 10, mean 22, 95% CI 17 to 26 months). Six of these deaths were caused by eyelid SCC (5.1% tumour associated mortality rate, Kaplan-Meier curve see figure 2) at 0, 9, 10, 10, 12 and 35 months of follow-up and two by further cancerous lesions (metastatic pleural mesothelioma and metastatic parotid carcinoma, at 25 and 57 months of follow-up) recorded in the register of deaths. DSS was 95.7% at 2 years (five deaths from eyelid SCC) and 94.9% at 5 years (with a total of 6 deaths due to eyelid SCC). No further disease-associated deaths were noted throughout further follow-up (censored at last presentation). The following deaths were noted as directly related to eyelid SCC: One patient presented with vast eyelid SCC, orbital as well as sinus and osseous tumour infiltration (category T4b) and received palliative treatment only due to his strongly reduced general health status. He succumbed to acute cerebritis and abscess forwarded by the osseous defect to the skull base less than 1 month after histopathology was taken. Another patient died from tumour invasion of the cavernous sinus. Four patients died from proven eyelid SCC metastasis.
{kind=link}
{kind=link}
Kaplan-Meier survival function showing the follow-up of 117 patients with 6 patients (5.1%) having died from eyelid SCC and 2 (1.7%) patients having succumbed to other malignancies. SCC, squamous cell carcinoma.
Comparison of AJCC 7 and AJCC 8 staging classifications
T category differed in a total of 34 (29.1%) patients when grouping by the AJCC 7 vs AJCC 8 staging system (p<0.001, Fisher’s exact test). A total of 28 (23.9%) patients were downstaged from T2 (AJCC 7) to T1 (AJCC 8) and 6 (5.1%) patients were upstaged from T3 to T4. Five out of 6 patients who died from eyelid SCC had T4 disease per AJCC 8 at initial presentation, whereas two out of these six patients had been categorised as T3a and T3b per AJCC 7. One patient was staged T2b (AJCC 7) and T2c (AJCC 8), respectively.
Changes in T category as per the AJCC 8 resulted in better prediction of DSS (p=0.024, Fisher’s exact test). Going more into detail, DSS could be proven significantly worse in patients with tumours of AJCC 8 tumour stage T2c or higher (0=0.018; Fisher’s exact test).
Subgroup comparison of tumour variables
For assessment of possible changes in tumour or patient characteristics over time, we divided patients into patient subgroups diagnosed between 2009–2011 (n=32), 2012–2014 (n=27), 2015–2017 (n=28) and 2018–2020 (n=30) that did not differ significantly in number and performed Kruskal-Wallis analysis and Mann-Whitney U test for all tumour parameters mentioned above as the potential confounders, but found no significant differences (table 4).
Excerpt of parameters tested by Kruskal-Wallis analysis
Discussion
The most important results of this study include that, similar to the previous publication from the USA by Xu et al, AJCC 8th edition T category and N category are important prognostic factors for DSS.13 In addition, we found male gender to be associated with nodal metastasis and recurrence as well as location in the medial upper eyelid to be an important negative predictor for nodal metastasis and tumour mortality.
Importantly, the eighth edition AJCC staging system for carcinoma of the eyelid has been proven superior to the seventh edition.12 We could confirm that both T-category and nodal metastasis are negative prognostic factors for DSS of eyelid SCC patients13 in the present study.
T category differed in a significant number of patients (29.1%) when grouping by AJCC 7 and 8, respectively, which is similar to a large US American analysis.13 In the present study, downstaging resulted mainly from T2 (AJCC 7) to T1 (AJCC 8) due to the changes of tumour dimension (T1 ≤5 mm according to AJCC 7 and ≤10 mm in AJCC 8). Upstaging resulted in shifting from T3 (AJCC 7) to T4 (AJCC 8) in six cases (due to size limitation of ≤30 mm for T3 in AJCC 8). Consequently, as two of the patients staged as T3a and T3b, respectively, converted to T4 (AJCC 8), and 5 out of 6 patients who died were classified with T4 tumours (AJCC 8), prediction of DSS was significantly better for the updated staging system which again is in accordance with the literature.13 In a recent study, T4 category and tumour recurrence were the most important prognostic factors in eyelid malignancies14 which we could confirm in our analysis. All patients who died in the follow-up of our study were staged T2c or worse as per AJCC 8 which is in accordance with previous analyses.13
Furthermore, male gender was a risk factor for lymph node invasion and recurrence in this study. The predominance of recurrence in male patients noted may be associated with increased occupational sunlight exposure as suggested previously in an Australian publication including 51 cases of eyelid SCC.3 In the literature, a history of cutaneous SCC has been shown to have a three times relative risk of developing another SCC compared with patients without SCC history15 and recurrence has been described as an important prognostic factor in eyelid malignancies.14
Our results conclude that tumour location in the medial upper eyelid was associated with mortality, whereas tumour of the lower eyelid alone was a positive predictor. As reported in previous studies, eyelid SCC developed predominantly on the lower lid,3 followed by the upper lid and then the medial and lateral canthi. When dividing the lid into quadrants, our statistical analysis proved location in the medial upper eyelid as a negative predictive factor for DSS as well as lymph node invasion. We would assume, that tumours in this location might go unnoticed for a longer period of time. On the other hand, as the lower lid is the known most common location for cutaneous eyelid tumours,3 we suppose that these tumours might be detected earlier by clinicians and this again might result in a better prognosis.
Two (1.7%) patients developed eyelid SCC after organ transplantation (one heart- and one lung-transplantation) and under systemic immunosuppression (8, 6.8%), a further known risk factor for skin cancer3 that has also been associated with tumour recurrence recently.13
We could not prove a statistical preponderance of SCC on the right or left side in the current study. The predominance of the side of the lesion depending from increased sunlight exposure while driving has been described previously for SCC as well as basal cell carcinomas,3 16 but this may be more notable in southern regions with higher cumulative sunlight exposure.
Orbital invasion is a rare complication of advanced SCC and, if recognised early, can be treated effectively with exenteration.3 All patients with orbital and/or suspected perineural invasion were presented at our institution’s interdisciplinary tumour board with preoperative cross-sectional imaging and definitive treatment was decided in consensus. Orbital exenteration was necessary for local disease control in 12 (10.3%) patients in the present study and was performed combined with adjuvant therapy in 7 (58.3%) of these patients (radiotherapy in 6 (50.0%), chemotherapy in 1 (8.3%); additional resection of lymph nodes or parotidectomy in 7 (58.3%) cases). No tumour recurrence was noted post complete surgical resection within this patient subcollective. There is strong evidence for adjuvant radiotherapy in cases of perineural invasion, as a relapse in SCC of the head and neck has been reported in around 50%.17 In the present study, 13 (92.9%) of 14 patients with perineural invasion underwent adjuvant radiotherapy (6 in combination with orbital exenteration as stated above), one patient received palliative treatment only.
Further important adjuvant tumour therapy regimen also included topical interferon-alpha-2b eyedrops in 6 (5.1%) patients suffering from eyelid as well as concomitant SCC of the conjunctiva. Mean, median and range of follow-up of these patients was 37, 27 and 10–83 months, respectively. Four of these patients already had a history of previous conjunctival intraepithelial neoplasia or SCC. The authors have discussed their clinical experience with good efficacy of topical interferon-alpha-2b treatment of different epithelial conjunctival pathologies previously.18–20 Of course, this treatment is only meaningful as additional adjuvant treatment in multilocular lesions including the conjunctiva for eyelid SCC.
Importantly, no significant change in epidemiological patient or tumour characteristics was noted for this patient collective when performing subgroup analysis (2009–2011, 2012–2014, 2015–2017 and 2018–2020).
This study has certain limitations: First, although the total number of cases included in this study is meaningful, due to the retrospective nature of the study, the follow-up at our tertiary centre is limited despite the 11-year recruitment period, as patients oftentimes returned to their referring practitioner for follow-up visits. Although possible tumour recurrence or cases of tumour mortality may have been missed, the recurrence rate we found was in good conformity with the literature (1.9%6; 2.0%3). The rates of nodal or distant metastases reported vary greatly (1%–21% and 0%–21.4%, respectively).2 3 21 22
Second, although external histology had proven eyelid SCC in 20 patients and they were referred with recurrent eyelid SCC from their treating Ophthalmologist, we cannot differentiate with certainty between recurrence and incomplete surgical resection in these cases. Precancerous conditions or risk factors may have been missed, again to the retrospective nature of the study.
Third, despite the large number of 117 patients and long recruitment period included, the presence of certain factors was too small in numbers to conduct a multivariate analysis that could prove possible associations between the factors assessed.
In conclusion, patients with known risk factors for the development of SCC should be monitored closely. Differences between the AJCC 7 and AJCC 8 staging classification systems were significant. Early excisional biopsy of suspicious lesions is mandatory and would be expected to have an impact on patient survival as tumour category T2c or above and nodal metastasis was associated with worse DSS. Due to the negative prognosis, special care should be taken in the clinical evaluation of the medial upper eyelid. All patients with eyelid SCC should be advised of the risk of relapse or development of new tumours and be encouraged to attend long-term follow-up.
Data availability statement
Deidentified participant data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Institutional review board approval was obtained.
References
Footnotes
Contributors All authors have contributed substantially to the present study. AK: Conception and design of the study, data acquisition, analysis, drafting of the work, final approval. CS: Data analysis, critical revision, final approval. EMM: Data acquisition, critical revision, final approval. AG-K: Critical revision, final approval. SGP: Critical revision, final approval. CRH: Data acquisition, critical revision, final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance