Article Text

Abstract
Background/Aims Long COVID is characterised by a range of potentially debilitating symptoms which develop in at least 10% of people who have recovered from acute SARS-CoV-2 infection. This study has quantified corneal sub-basal nerve plexus morphology and dendritic cell (DC) density in patients with and without long COVID.
Methods Forty subjects who had recovered from COVID-19 and 30 control participants were included in this cross-sectional comparative study undertaken at a university hospital. All patients underwent assessment with the National Institute for Health and Care Excellence (NICE) long COVID, Douleur Neuropathique 4 (DN4) and Fibromyalgia questionnaires, and corneal confocal microscopy (CCM) to quantify corneal nerve fibre density (CNFD), corneal nerve branch density (CNBD), corneal nerve fibre length (CNFL), and total, mature and immature DC density.
Results The mean time after the diagnosis of COVID-19 was 3.7±1.5 months. Patients with neurological symptoms 4 weeks after acute COVID-19 had a lower CNFD (p=0.032), CNBD (p=0.020), and CNFL (p=0.012), and increased DC density (p=0.046) compared with controls, while patients without neurological symptoms had comparable corneal nerve parameters, but increased DC density (p=0.003). There were significant correlations between the total score on the NICE long COVID questionnaire at 4 and 12 weeks with CNFD (ρ=−0.436; p=0.005, ρ=−0.387; p=0.038, respectively) and CNFL (ρ=−0.404; p=0.010, ρ=−0.412; p=0.026, respectively).
Conclusion Corneal confocal microscopy identifies corneal small nerve fibre loss and increased DCs in patients with long COVID, especially those with neurological symptoms. CCM could be used to objectively identify patients with long COVID.
- cornea
- Covid-19
- imaging
Data availability statement
The data that support the findings of this study are available from the corresponding author (ORCID: 0000-0002-0509-5649) upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has been caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Although the major acute clinical manifestations of the disease involve the respiratory tract, neurological symptoms including loss of taste and smell, headache, dizziness, numbness, and neuropathic pain have been reported.1 2 The exact mechanism of neurological involvement in SARS-CoV-2 infection remains unclear, although pathways involving direct retrograde trans-neuronal or haematogenous pathways, and indirect innate and adaptive immune responses have been proposed.3
It is now becoming clear that at least 10% of people who have recovered from acute COVID-19 infection will develop long COVID.4 5 The National Institute for Health and Care Excellence (NICE), Scottish Intercollegiate Guidelines Network (SIGN), and Royal College of General Practitioners (RCGP) have developed a rapid guideline for diagnosing and managing long COVID.6 The guideline defines long COVID as ‘signs and symptoms that develop during or following an infection consistent with COVID-19 and which continue for more than 4 weeks and are not explained by an alternative diagnosis’. NICE further recommends the term ‘post-COVID syndrome’ for ongoing symptoms, beyond 12 weeks after infection with SARS-CoV-2. Long COVID is characterised by a heterogenous complex of symptoms affecting several organ systems; however, neurological and musculoskeletal symptoms are prominent.4 It has been suggested that small nerve fibre damage may underlie long COVID.7 8 Indeed, in our recent study we reported widespread sensory symptoms with loss of taste and smell and abnormal thermal thresholds in patients with diabetes who had recovered from severe COVID-19.9
Corneal confocal microscopy (CCM) is a real-time, non-invasive, high-resolution imaging technique which allows objective quantification of corneal sub-basal nerve fibres and dendritic cells (DCs). We have previously utilised CCM to show corneal nerve fibre loss in patients with idiopathic small fibre neuropathy,10 painful diabetic neuropathy11 and fibromyalgia,12 and an increase in DCs in patients with diabetic neuropathy13 and inflammatory and immune mediated nerve damage including multiple sclerosis and chronic inflammatory demyelinating polyneuropathy.14 15
In the present study, we utilised CCM to quantify sub-basal corneal nerve morphology and DC density in patients with and without long COVID. We also assessed the association between corneal nerve and DC abnormalities with the severity of long COVID, particularly in relation to neuropathic and musculoskeletal symptoms.
Methods
Forty patients within 1–6 months of COVID-19 and 30 healthy control subjects were enrolled in this cross-sectional study at a single tertiary referral university hospital. The study design fulfilled the tenets of the Declaration of Helsinki and was approved by the Research Ethics Committee of the Necmettin Erbakan University. A detailed explanation of the study protocol was provided and written informed consent was obtained from all participants.
Acute COVID-19 infection was defined by symptomatic presentation at hospital and confirmation of SARS-CoV-2 by reverse transcriptase-polymerase chain reaction (RT-PCR) assay of oropharyngeal and nasopharyngeal swabs. Exclusion criteria were any existing ophthalmic disease requiring topical medications, contact lens use, a previous history of ocular surgery or trauma, diabetes mellitus and any other systemic disease that might cause peripheral neuropathy. Patient records were retrospectively reviewed for blood test results including white cell count (WCC), C-reactive protein (CRP), fibrinogen, ferritin and D-dimer levels during the acute infection.
A questionnaire in accord with the long COVID guideline developed jointly by NICE, SIGN and the RCGP16 was administered to identify persisting symptoms at 4 and 12 weeks after the diagnosis of acute COVID-19 (online supplemental file E1). This questionnaire consists of 28 items in nine domains including generalised, respiratory, cardiovascular, neurological, musculoskeletal, psychological/psychiatric, gastrointestinal, dermatological, and ear, nose and throat symptoms, with a total score ranging from 0 to 28. The neurological domain of this questionnaire consists of seven items, scoring between 0 and 7. The Douleur Neuropathique 4 (DN4) interview questionnaire was used to identify neuropathic pain and consists of 10 items with a total score ranging from 0 to 10. The Fibromyalgia Questionnaire (FM-Q) was used to localise and grade the severity of muscle pain and overlapping symptoms including headache, depression/anxiety, heartburn, irritable bowel, bladder problems, fatigue, waking up unrefreshed and cognitive issues, with a total score ranging from 0 to 26.17
Supplemental material
All subjects underwent laser scanning CCM using the Rostock Corneal Module/Heidelberg Retina Tomograph lll (Heidelberg Engineering, Germany). The section mode was used to scan the central cornea, and two-dimensional digital images with an image size of 400×400 µm, a lateral digital resolution of 1 µm/pixel, and a depth resolution of 2 µm/pixel were obtained. Three high-quality sub-basal nerve plexus images were selected from each subject based on a previously defined standardised image selection protocol.18 The investigator (GB) undertaking the CCM was aware if the participant was a control subject or a patient with COVID-19. However, the investigator was not aware of the identity of the participant when quantifying corneal nerve or DC morphology, as the images were anonymised and coded. Corneal nerve plexus parameters were manually quantified and included: corneal nerve fibre density (CNFD)—the total number of major nerves (no./mm2); corneal nerve branch density (CNBD)—the number of branches arising from major nerves (no./mm2); and corneal nerve fibre length (CNFL)—the total length of all nerve fibres and branches (mm/mm2) using validated, purpose-designed software (CCMetrics, University of Manchester, Manchester, UK).19 DC density was quantified in the same image frames used to quantify the sub-basal nerve plexus. The number of highly reflective cells with (mature) and without (immature) dendriform structures were counted manually using the branch density quantification feature of the CCMetrics software, and the density was derived as the number of cells in the area of frame assessed (no./mm2).
Statistical analysis was performed using SPSS version 21.0 (Chicago, IL, USA) software. Basic descriptive statistics were calculated on all the data and are reported as mean±SD or median (IQR), as appropriate. Normal distribution of continuous variables was confirmed with the Shapiro-Wilk test. The Pearson χ2 test was used to compare categorical variables. Independent samples t-test for parametric data and Mann-Whitney U test for non-parametric data were used to compare the measures between the post-COVID patients and control subjects. One-way analysis of variance (ANOVA) test followed by Tukey multiple comparison test or Kruskal-Wallis test followed by Dunn’s test with adjusted p values using the Benjamini-Hochberg procedure were used to compare the parameters among the created subgroups. The Pearson χ2 test and independent samples t-test were used to compare the differences in age and gender among the subgroups of patients with COVID-19. The associations between variables were measured using Spearman’s rank correlation coefficient. For all evaluations, a two-sided p value <0.05 was considered statistically significant.
Results
Clinical and demographic measures
The demographic and clinical characteristics of the study participants are summarised in table 1. There were no significant differences between COVID-19 patients and control subjects for age (mean (SE) difference −0.23 (3.29), 95% CI −6.79 to 6.34; p=0.946) and gender (female/male 18/22 vs 14/16, respectively; p=0.890). The mean time after the diagnosis of COVID-19 was 3.7±1.5 months and was >12 weeks in 73% (29/40) of cases. Patients had received treatment with favipiravir (n=32, 80%), hydroxychloroquine (n=18, 45%), and enoxaparin (n=27, 68%) during the acute phase of COVID-19. In the acute phase, 22 patients (55%) had no clinical signs of pneumonia, 11 (28%) had clinical signs of pneumonia not requiring oxygen therapy, four (10%) were hospitalised with pneumonia and received oxygen therapy, and three (8%) patients with pneumonia were admitted to the intensive care unit (ICU) for respiratory support. The median (IQR) and mean±SD duration of stay in hospital and ICU were 11.0 (8.0–29.0) days and 10.7±3.5 days, respectively. Pre-existing comorbidities included hypertension in five patients (13%), asthma in three patients (8%), coronary artery disease in one patient (3%), and euthyroid Hashimoto’s thyroiditis in one patient (3%). The median (IQR) values of admission blood parameters were as follows: WCC 6.3 (4.9–7.7) 103/µL; CRP 4.8 (2.0–37.4) mg/L; fibrinogen 320.0 (268.0–445.0) mg/dL; ferritin 107.2 (33.6–215.1) µg/L; D-dimer 112.0 (53.3–173.8) ng/mL.
Baseline characteristics of the study participants
Corneal nerve and dendritic cell parameters
Figure 1 illustrates the CCM images of the central corneal sub-basal nerve plexus in a healthy subject and COVID-19 patients with and without neurological symptoms. CNBD was lower (mean (SE) difference −11.16 (4.58), 95% CI −20.30 to −2.02; p=0.017), total (median (IQR) 39.5 (13.2–92.5) vs 12.7 (0–30.4) cells/mm2; p=0.001), mature (median (IQR) 7.3 (0–16.7) vs 0 (0–4.2) cells/mm2; p<0.001) and immature (median (IQR) 30.6 (8.9–69.9) vs 12.7 (0–24.7) cells/mm2; p=0.002) DC densities were higher, with no difference in CNFD (mean (SE) difference −2.50 (1.68), 95% CI −5.84 to 0.85; p=0.141) and CNFL (mean (SE) difference −1.81 (1.02), 95% CI −3.85 to 0.22; p=0.080) in COVID-19 patients compared with control subjects (table 2).
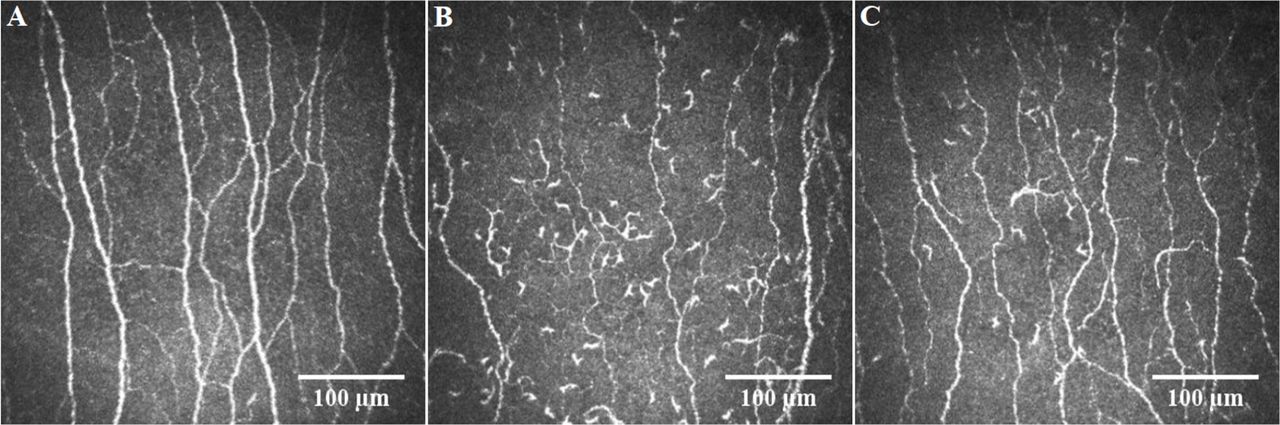
Representative corneal confocal microscopic images of the central corneal sub-basal nerve plexus in a healthy control participant (A), and in COVID-19 patients with (B) and without (C) long COVID.
Corneal confocal microscopic parameters in COVID-19 patients and healthy control subjects
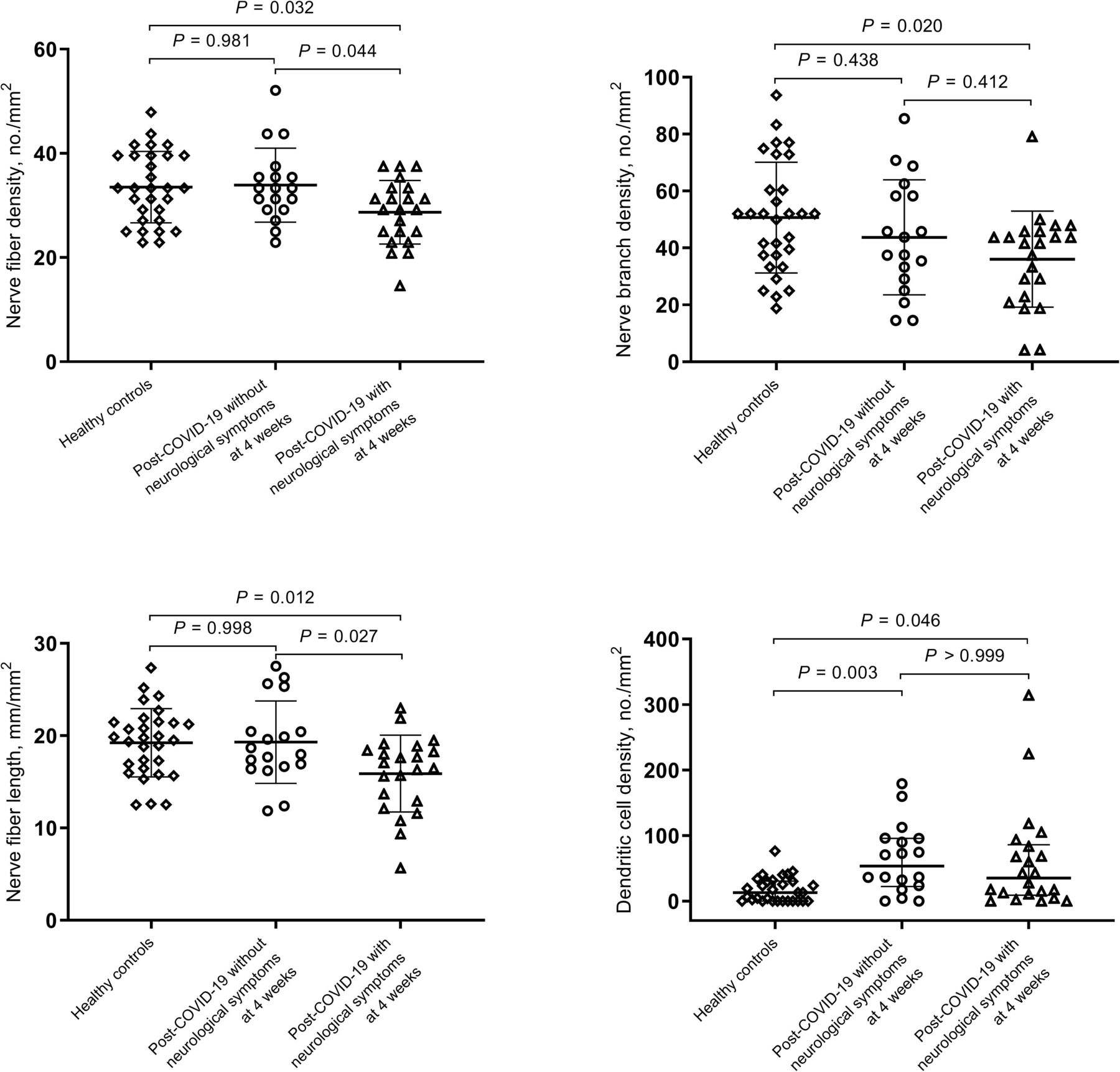
Neurological symptoms were present at 4 and 12 weeks in 22/40 (55%) and 13/29 (45%) patients, respectively. Subgroup analysis revealed that patients with neurological symptoms at 4 weeks had a lower CNFD (mean (SE) difference −4.85 (1.88), 95% CI −9.36 to −0.35; p=0.032), CNBD (mean (SE) difference −14.62 (5.30), 95% CI −27.32 to −1.91; p=0.020), and CNFL (mean (SE) difference −3.35 (1.14), 95% CI −6.08 to −0.62; p=0.012), and increased total (median (IQR) 35.1 (9.0–85.8) vs 12.7 (0–30.4) cells/mm2; p=0.046) and mature (median (IQR) 7.3 (0–18.7) vs 0 (0–4.2) cells/mm2; p=0.003) DC densities, compared with control subjects. Patients without neurological symptoms had comparable corneal nerve parameters but increased total (median (IQR) 53.5 (22.0–95.7) vs 12.7 (0–30.4) cells/mm2; p=0.003), mature (median (IQR) 7.3 (0–15.1) vs 0 (0–4.2) cells/mm2; p=0.010) and immature (median (IQR) 33.5 (15.2–80.3) vs 12.7 (0–24.7) cells/mm2; p=0.007) DC densities, compared with control subjects (table 2). CNFD (mean (SE) difference −5.22 (2.13), 95% CI −10.33 to −0.12; p=0.044) and CNFL (mean (SE) difference −3.41 (1.29), 95% CI −6.50 to −0.32; p=0.027) were lower in patients with compared with without neurological symptoms (figure 2).
{kind=link}
{kind=link}
Corneal nerve fibre parameters and dendritic cell density in healthy control participants and patients with and without neurological symptoms 4 weeks after the initial diagnosis of COVID-19. Error bars indicate mean (SD) for corneal nerve fibre density, nerve branch density and nerve fibre length, and median (IQR) for dendritic cell density.
Patients with neurological symptoms at 12 weeks had a lower CNFD (mean (SE) difference −6.94 (2.22), 95% CI −12.28 to −1.60; p=0.008), CNBD (mean (SE) difference −16.40 (6.31), 95% CI −31.59 to −1.21; p=0.031) and CNFL (mean (SE) difference −4.51 (1.33), 95% CI −7.70 to −1.31; p=0.004), and higher total (median (IQR) 59.6 (14.9–99.2) vs 12.7 (0–30.4) cells/mm2; p=0.016), mature (median (IQR) 8.3 (4.1–21.9) vs 0 (0–4.2) cells/mm2; p=0.001), and immature (median (IQR) 41.2 (11.9–78.3) vs 12.7 (0–24.7) cells/mm2; p=0.039) DC densities, compared with control subjects (table 3). CNFD (mean (SE) difference −7.78 (2.49), 95% CI −13.78 to −1.78; p=0.008) and CNFL (mean (SE) difference −4.80 (1.49), 95% CI −8.40 to −1.21; p=0.006) were lower in patients with compared with without neurological symptoms.
Corneal confocal microscopic parameters in COVID-19 patients with and without persisting neurological symptoms at 12 weeks and healthy control subjects
CNFD (mean (SE) difference −6.38 (2.63), 95% CI −12.72 to −0.04; p=0.048) and CNFL (mean (SE) difference −4.56 (1.55), 95% CI −8.29 to −0.83; p=0.013) were lower in patients with compared with without long COVID (online supplemental table S1). CNFD (mean (SE) difference −5.51 (2.12), 95% CI −10.59 to −0.44; p=0.030) and CNFL (mean (SE) difference −3.68 (1.28), 95% CI −6.74 to −0.62; p=0.015) were lower in patients with compared with without clinical signs of pneumonia (online supplemental table S2).
Supplemental material
There were no significant differences for age and gender among all compared subgroups of patients with COVID-19 (p>0.05 for all, data not shown).
Relationship to neuropathic pain (DN4)
There was no significant difference in the DN4 score between subjects with and without long COVID (median (IQR) 0 (0–4.3) vs 0 (0–0), respectively; p=0.060). The proportion of patients with a DN4 ≥4, which defines patients with neuropathic pain, was greater in patients with long COVID (5/18, 28%) compared with patients without long COVID (0/11, 0%), but did not achieve statistical significance (p=0.055).
Relationship to musculoskeletal symptoms (FM-Q)
The FM-Q score was significantly higher in subjects with long COVID compared with subjects without long COVID (median (IQR) 11.0 (7.5–12.0) vs 2.0 (1.0–8.0), respectively; p=0.001).
Correlations between CCM and NICE-Q, DN4, FM-Q disease scores
Among patients with COVID-19, there were significant inverse correlations between CNFD and the total score on the NICE long COVID questionnaire at 4 (ρ=−0.436; p=0.005) and 12 weeks (ρ=−0.387; p=0.038), NICE questionnaire neurological scores at 4 (ρ=−0.407; p=0.009) and 12 weeks (ρ=−0.547; p=0.002), and FM-Q score (ρ=−0.399; p=0.011). There were significant inverse correlations between CNFL and the total score on the NICE long COVID questionnaire at 4 (ρ=−0.404; p=0.010) and 12 weeks (ρ=−0.412; p=0.026), NICE questionnaire neurological scores at 4 (ρ=−0.386; p=0.014) and 12 weeks (ρ=−0.469; p=0.010), and FM-Q score (ρ=−0.419; p=0.007). There were significant inverse correlations between CNBD and the DN4 score (ρ=−0.347; p=0.028), CRP (ρ=−0.365; p=0.043), total DC density (ρ=−0.365; p=0.020), mature DC density (ρ=−0.419; p=0.007), and immature DC density (ρ=−0.353; p=0.025).
Discussion
To the best of our knowledge, this is the first study reporting corneal nerve loss and an increase in DC density in patients who have recovered from COVID-19, especially in subjects with persisting symptoms consistent with long COVID. Several studies have reported varied neurological manifestations related to acute COVID-19, suggestive of both central and peripheral nervous system involvement, including encephalitis, cranial neuropathy, Guillain-Barré syndrome, and peripheral neuropathy.3 20–22 A case series of 214 patients from Wuhan reported that 36.4% of patients had neurological symptoms and 2.3% had neuropathic pain.1 In another study including 350 patients with COVID-19, neurological manifestations were present in 18.9% and 3.1% had numbness or paresthesia.23
A recent meta-analysis suggested that 80% of patients who have recovered from COVID-19 continue to have at least one symptom, sign, or abnormal laboratory parameter, beyond 2 weeks after the initial diagnosis.24 Carfì et al 25 reported that 87% of hospitalised patients had at least one persisting symptom 60 days after the acute diagnosis of COVID-19. In another study, only 0.7% of patients were reported to be completely free of symptoms, 79 days after the initial diagnosis of COVID-19.26 Our study shows that at least one neurological symptom was present in 55% and 45% of patients, 4 and 12 weeks after the onset of COVID-19, while at least one symptom was present in 78% and 62% of patients at 4 and 12 weeks, consistent with long COVID.
There are now emerging studies which provide biological plausibility for the development of peripheral neuropathy and neuropathic pain as a result of COVID-19.8 27 It has also been suggested that small fibre neuropathy may underlie long COVID based on a case report of orthostatic cerebral hypoperfusion syndrome and painful small fibre neuropathy in a patient with COVID-19.28 Odriozola et al 9 have also reported the presence of a widespread sensory neuropathy and small and large fibre dysfunction in diabetic patients who had recovered from severe COVID-19. Although detailed neuromuscular studies are limited and tend to be biased, as they are based on reports from patients with more severe acute COVID-19 and critical illness, they nevertheless report abnormalities consistent with a peripheral neuropathy and myopathy.29 30
We and others have previously reported on the utility of CCM to identify small nerve fibre damage in various central and peripheral neurodegenerative disorders.10 11 14 15 We have now utilised CCM to demonstrate corneal nerve fibre damage, especially in those with neurological symptoms, 4 and 12 weeks after the initial diagnosis of COVID-19. Furthermore, we show significant associations between corneal nerve fibre loss and the severity of long COVID based on the NICE long COVID questionnaire, neuropathic pain based on DN4, and musculoskeletal symptoms based on the FM-Q. This is consistent with our previous studies showing corneal nerve fibre loss in patients with idiopathic small fibre neuropathy, painful diabetic neuropathy and fibromyalgia.10–12
Another major finding of this study is that corneal DC density was increased in COVID-19 patients, comprised of mature DCs in patients with persisting neurological symptoms at 4 weeks, with an increase in both mature and immature DCs at 12 weeks, providing insights into the evolution of immune activation in COVID-19. Brain autopsy material from a patient with SARS-CoV-2 infection showed microglial activation and pronounced neuronophagia involving the inferior olivary nuclei and cerebellar dentate nuclei.31 Neuropathological studies have also shown SARS-CoV-2 in the cerebrum, cerebellum, cranial nerves, olfactory bulb and olfactory epithelium, with associated microglial activation and lymphoid inflammation.32 Furthermore, COVID-19 infection has been associated with Guillain-Barré syndrome, a post-infectious immune mediated peripheral neuropathy,22 and an improvement in neuropathy has been observed following plasma exchange.33 In this study, we show an increase in mature and immature corneal DCs in patients with COVID-19 which was associated with reduced CNBD. These findings are consistent with an innate immune and inflammatory process characterised by the migration and accumulation of DCs in the central cornea in a number of immune mediated and inflammatory conditions.14 15 34 Further study of the relative change in mature and immature DC density and corneal nerves in COVID-19 patients over time may provide insights into the contribution of immune and inflammatory pathways to nerve degeneration.
According to data from China, among 44 415 confirmed COVID-19 patients, 81% had mild or moderate disease, 14% had severe disease, and 5% had critical illness.35 In the current study, 83% of patients had mild and moderate disease (without clinical signs of pneumonia and mild pneumonia not requiring oxygen support), 10% had severe disease (need for oxygen therapy), and 8% had critical disease (requiring ICU admission due to respiratory failure), indicating that our study population is comparable with other large populations in terms of disease severity presentation. We also show that patients with more severe acute COVID-19 had evidence of greater corneal nerve damage, suggesting that the severity of nerve damage may be related to the severity of disease at presentation.
We acknowledge several limitations, including the relatively small number of study participants and the absence of longer-term follow-up examination. Other limitations include the use of questionnaires to define the severity of neurological symptoms rather than more objective measures of neuropathy including quantitative sensory testing, nerve conduction studies and skin biopsy, and the lack of assessment of ocular surface symptoms and corneal sensitivity. Nevertheless, we show that patients with long COVID have evidence of small nerve fibre damage which relates to the severity of long COVID and neuropathic as well as musculoskeletal symptoms. Further studies of larger cohorts of patients using additional measures of neuropathy and CCM are required. Corneal confocal microscopy may have clinical utility as a rapid objective ophthalmic test to evaluate patients with long COVID.
Data availability statement
The data that support the findings of this study are available from the corresponding author (ORCID: 0000-0002-0509-5649) upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study concept and design: GB, CK, RAM. Data collection: GB, CK, AZ, AO. Data analysis and interpretation: GB, NZ, GP, RAM. Drafting the manuscript: GB, CK, AZ. Revision of the manuscript: AO, NZ, RAM. Administrative, technical, or material support: AZ, AO, NZ, GP, RAM. Study supervision: RAM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue