Article Text

Abstract
Purpose To report the ocular characteristics and the presence of viral RNA of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in conjunctival swab specimens in a patient with confirmed 2019 novel coronavirus disease (COVID-19).
Participant and methods A 30-year-old man with confirmed COVID-19 and bilateral acute conjunctivitis which occurred 13 days after illness onset. Based on detailed ophthalmic examination, reverse transcription PCR (RT-PCR) was performed to detect SARS-CoV-2 virus in conjunctival swabs. The ocular characteristics, presence of viral RNA and viral dynamics of SARS-CoV-2 in the conjunctival specimens were evaluated.
Results Slit lamp examination showed bilateral acute follicular conjunctivitis. RT-PCR assay demonstrated the presence of viral RNA in conjunctival specimen 13 days after onset (cycle threshold value: 31). The conjunctival swab specimens remained positive for SARS-CoV-2 on 14 and 17 days after onset. On day 19, RT-PCR result was negative for SARS-CoV-2.
Conclusion SARS-CoV-2 is capable of causing ocular complications such as viral conjunctivitis in the middle phase of illness. Precautionary measures are recommended when examining infected patients throughout the clinical course of the infection. However, conjunctival sampling might not be useful for early diagnosis because the virus may not appear initially in the conjunctiva.
- conjunctiva
- infection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In December 2019, an outbreak of a novel coronavirus disease (COVID-19) emerged in Wuhan, China, and has quickly spread throughout the world. 1 COVID-19 is a highly contagious disease capable of progression to acute respiratory distress syndrome and even death.1 The infectious agent of this disease entity is caused by a novel betacoronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Coronavirus had been previously reported to be associated with conjunctivitis in humans.2 Additionally, retinal disorders, such as retinal vasculitis,3 4 retinal degeneration5 6 and blood–retinal barrier breakdown,7 had been demonstrated in experimental animal models of coronavirus infection. However, ocular complications of SARS-CoV-2 infection have not been widely reported .8 In addition, viral loads in ocular tissue are still to be investigated.
Here, we report the ocular presentations of a patient with confirmed COVID-19 who developed bilateral redness of the eyes 13 days after the onset of systemic symptoms in Shenzhen, China. Our findings will facilitate understanding of ocular features in patients with COVID-19 and the clinical course of ophthalmic complications.
Case report
Institutional review board approval was obtained for this study and we strictly followed the Declaration of Helsinki in all procedures. Written informed consent was obtained from the case patient.
On 4 February 2020, a 30-year-old man presented to a local hospital with symptoms of sore throat and diarrhoea that started on 31 January 2020 (day 1 of illness). He disclosed a history of close contact with a patient with COVID-19 from 28 to 30 January 2020. His medical history was unremarkable. His physical examination was normal. Given the patient’s contact history, nasopharyngeal swab samples were collected to test for SARS-CoV-2 and chest CT was performed, showing localised emphysema in the left lung. The patient was then discharged to home isolation.
On 5 February 2020 (day 6 of illness), the local hospital confirmed that the patient’s nasopharyngeal swabs tested positive for SARS-CoV-2 in a reverse transcription PCR (RT-PCR) assay. Therefore, he was admitted to an airborne infection isolation ward at the Third People’s Hospital of Shenzhen, the only designated hospital for confirmed COVID-19 cases in Shenzhen.
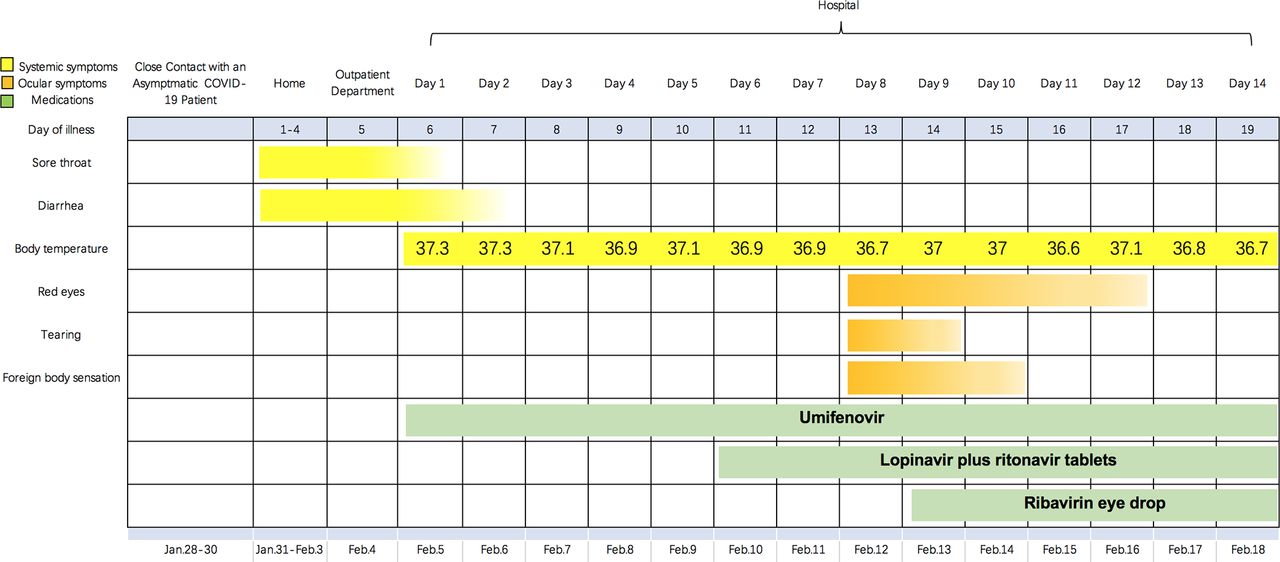
On admission, vital signs, except a body temperature of 37.3°C, were within the normal ranges. Lung auscultation demonstrated rhonchi. For differential diagnosis, other viral respiratory pathogens were tested with negative results. Nasopharyngeal swabs were tested again and found positive for SARS-CoV-2 by Shenzhen Centers for Disease Control (CDC) on day 2 of hospitalisation (day 7 of illness). Umifenovir was administered three times a day. Lopinavir plus ritonavir tablets were administered beginning on day 6 of hospitalisation (illness day 11). Other treatment was largely supportive. After such treatment, the patient’s vital signs were largely stable, apart from a mild fluctuation in body temperature (figure 1). He stated that his symptoms of sore throat and diarrhoea had gradually improved. Samples for repeat SARS-CoV-2 testing were obtained on illness days 13, 17 and 19 and included nasopharyngeal swabs, sputum and saliva specimens (figure 2).

Timeline of systemic and ocular symptoms according to day of illness and day of hospitalisation (28 January 2020 to 18 February 2020). COVID-19, 2019 novel coronavirus disease.
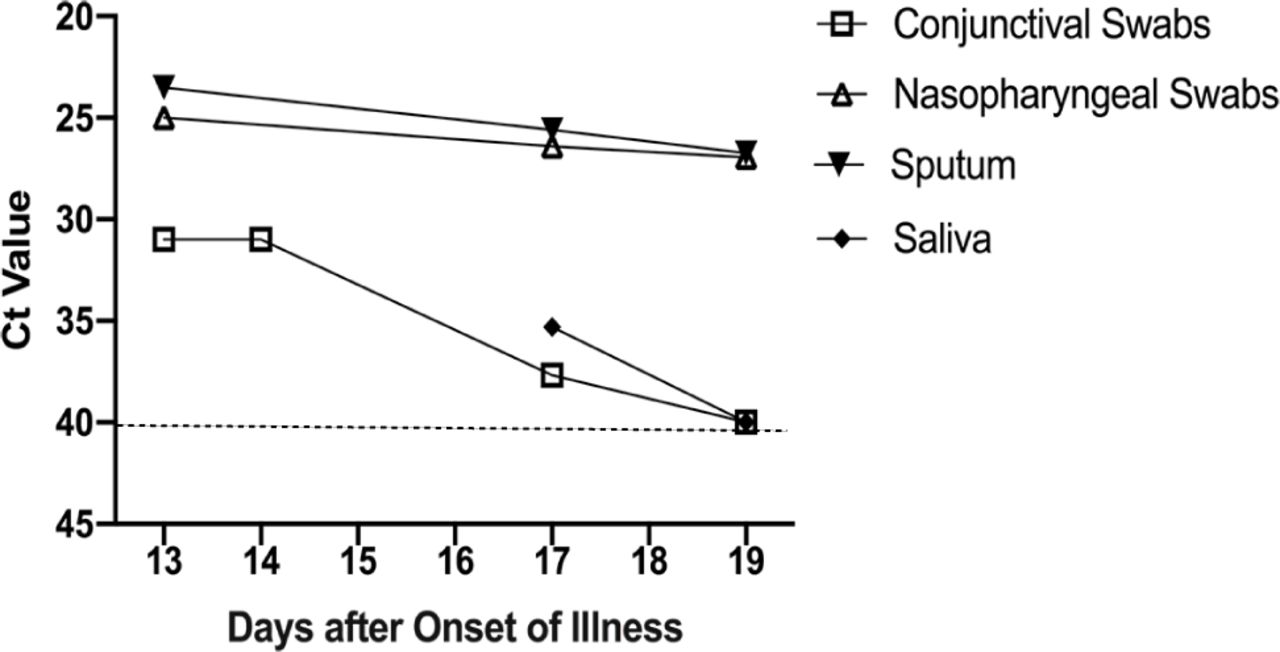
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA detected in different types of clinical samples obtained from the case patient. Dynamic alterations of viral loads in nasopharyngeal swabs, sputum, saliva and conjunctival swabs were shown. Cycle threshold (Ct) values were inversely proportional to viral loads. Negative results are shown with a Ct value of 40.
On day 8 of hospitalisation (day 13 of illness), the patient reported redness, foreign body sensation and tearing in both eyes without blurred vision. He denied touching his eyes with his hands. Best-corrected visual acuities were logMAR 0.10 and 0.05 in the right and left eyes, respectively. Slit lamp examination identified bilateral moderate conjunctival injection, watery discharge, inferior palpebral conjunctival follicles (figure 3) and tender palpable preauricular lymph nodes. No subconjunctival haemorrhage or pseudomembrane were observed. No lesions on the corneal or anterior chamber inflammation were detected. Fundus examination using Kowa non-mydriatic fundus camera (Kowa Company, Nagoya, Japan) revealed unremarkable findings. Macular ultrastructure and thickness measured on optical coherence tomography (Optovue, Fremont, California, USA) were within the normal ranges (figure 4).

Slit lamp examinations showed evidence of acute viral conjunctivitis. The examination on illness day 13 showed moderate conjunctival injection and inferior palpebral conjunctival follicles (A and D). Examinations on illness day 17 (B and E) and illness on day 19 (C and F) demonstrated that treatment with ribavirin eye-drops gradually improved the patient’s symptoms.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fundus examinations on illness day 13, hospital day 8. (A) The fundus photographs were unremarkable. (B) The ultrastructure of the central macula was normal. (C) The central macular thickness in both eyes were within normal ranges.
Conjunctival swabs were taken by putting sterile synthetic fibre swabs into the lower fornix of each eye without topical anaesthesia. The swabs were then inserted into a viral transport medium and stored at 4°C before being tested for SARS-CoV-2. Viral RNA were obtained from the samples with the QIAamp Viral RNA Viral Kit (QIAGEN, Hilden, Germany). A commercial kit (GeneoDX, Shanghai, China) specific for SARS-CoV-2 detection and approved by the China Food and Drug Administration was used to perform RT-PCR. In general, viral loads are inversely correlated with cycle threshold (Ct) values. Ct value of 40 indicates negative results.9 Routine bacterial and fungal cultures were also performed and yielded negative results at 48 hours.
On day 9 of hospitalisation (day 14 of illness), the conjunctival swab specimens proved to be positive for SARS-CoV-2 (Ct value: 31). Ribavirin eye-drops were prescribed to be administered four times per day. A slit lamp examination was carried out daily by one experienced ophthalmologist, who wore personal protective equipment recommended by the Shenzhen CDC. Conjunctival swabs were collected for repeated SARS-CoV-2 detection on illness days 14, 17 and 19 (figure 2).
On day 10 of hospitalisation (day 15 of illness), the patient reported no tearing in both eyes, and the redness and foreign body sensation were reduced. No tender preauricular lymph node was found. On day 11 of hospitalisation (day 16 of illness), he felt no discomfort in both eyes, and only mild redness remained. On day 14 of hospitalisation (day 19 of illness), the patient declared that all ocular symptoms had resolved. A slit lamp examination demonstrated reduction of bilateral conjunctival injection, as well as follicles on the inferior palpebral conjunctiva (figure 3).
The conjunctival swabs initially collected from this patient on day 13 of his illness were positive for SARS-CoV-2 RNA (figure 2). A Ct value of 31 indicated moderate quantity of virus in the conjunctival swabs, but was much lower than what was found in the nasopharyngeal (Ct value: 23.52) and sputum (Ct value: 25) specimens. Conjunctival specimens obtained on day 14 were still positive for SARS-CoV-2 RNA with the same Ct value 31. On day 17 of illness, the conjunctival swabs remained positive (Ct value: 37.67) but showed a trend of decreasing levels. The conjunctival samples tested negative for SARS-CoV-2 on illness day 19.
Discussion
We recorded the ocular complications of a patient with confirmed COVID-19 after 13 days of illness onset. The clinical presentation of this case met the criteria of acute viral conjunctivitis. It is possible that ribavirin eye-drops helped to treat the symptoms. The conjunctival swabs tested positive for SARS-CoV-2 RNA for at least 5 days with the Ct values gradually increasing. However, the detection was much lower in conjunctival swabs than in respiratory specimens. This case illustrates several aspects of ocular complications of COVID-19, including the full clinical course of ocular manifestations and the dynamic changes of SARS-CoV-2 viral detection in conjunctival swab samples.
Currently, our understanding of the possible ocular complications of SARS-CoV-2 infection is very limited. Guangfa Wang, an expert on COVID-19, reported that he developed red eyes several days before the onset of SARS-CoV-2 infection.10 A retrospective study tested conjunctival samples for SARS-CoV-2 RNA in 30 infected patients, and the conjunctival samples from one patient were positive for the viral RNA on 3 days after onset.11 The fact that our patient developed acute viral conjunctivitis with positive SARS-CoV-2 tests in conjunctival swab samples indicated that SARS-CoV-2 could indeed cause ocular complications but not necessarily in the early stage of illness. ACE 2 (ACE2) is a cellular receptor for SARS-CoV-2.12 Given that ACE2 has also been detected in the human retina,13 vascularised retinal pigment epithelium choroid14 and conjunctival epithelia,15 further clinical studies are needed to more fully evaluate the clinical spectrum of ocular diseases caused by SARS-CoV-2 infection.
SARS-CoV-2 RNA was detected in conjunctival sac samples obtained from our patient on days 13, 14 and 17 of illness. However, a previous report in the scientific literature demonstrated the presence of SARS coronavirus in patients’ tears early in the course of the disease.16 Middle East respiratory syndrome coronavirus (MERS-CoV) RNA was also identified at a high concentration in conjunctival swabs from camels at an early stage of infection.17 Our case indicated that the shedding pattern of SARS-CoV-2 may be different from that of SARS-CoV and MERS-CoV in conjunctival specimens. Precaution strategies used in SARS-CoV and MERS-CoV may need to be modified accordingly.
To our knowledge, this was the first report to determine the presence of the viral RNA over time in the conjunctival specimens of a patient with COVID-19. Viral RNA was present in our patient’s conjunctival sacs for at least 5 days. The viral RNA levels in conjunctival specimens were dramatically lower than those in respiratory samples. More viral RNA in conjunctival sacs (inversely related to Ct value)9 was detected 13 days after onset, soon after the symptom onset of acute conjunctivitis. Conjunctival specimens obtained on illness days 13, 14, 17 and 19 showed a trend toward decreasing levels of viral RNA. The result suggested that viral loads in conjunctival specimens gradually decrease over time with less potential for transmissibility accompanied by improvement of the ocular symptoms.
We described the clinical features of acute conjunctivitis occurring 13 days after onset in a patient with SARS-CoV-2 infection. This case report highlights the necessity to further understand the full spectrum, duration and natural history of ocular complications associated with SARS-CoV-2 infection to inform clinical treatment and affect precaution practices. Our case confirmed that SARS-CoV-2 led to ocular complications, but not in the early stage of infection. On the one hand, SARS-CoV-2 in conjunctival specimens might represent a source of spread, particularly with higher viral loads at the acute stage of ocular complications. On the other hand, the conjunctiva might not serve as an ideal site for sampling for early diagnostic tests of SARS-CoV-2 infection. Further study of virus infectivity specifically within ocular tissues would facilitate a better understanding of the pathogenicity of SARS-CoV-2 in the eyes.
References
Footnotes
LC and ML contributed equally.
LL, GZ and JW contributed equally.
Contributors Study design: LL, GZ and JW. Data collection: LC, MC, ZH and NX. Analysis and interpretation of the data: ZZ, KQ, TH and ML. Writing of the report: LC. Revision of the draft: LC, ZZ and GZ. Making the decision to submit the paper for publication: LL, GZ, JW, LC, MC, ZH, NX, ZZ, KQ, TH and ML.
Funding This study was supported by the National Natural Science Foundation of China (Grant No 81900877).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Institutional review board approval was obtained from the Third People's Hospital of Shenzhen.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement Data are available on reasonable request.
Linked Articles
- Commentary
- At a glance