Article Text

Abstract
Aims To describe the distributions of and associations with intraocular pressure (IOP) and circumpapillary retinal nerve fibre layer (cRNFL) thickness in a population-based study.
Methods Northern Ireland Cohort for the Longitudinal Study of Ageing participants underwent a computer-assisted personal interview, a self-completion questionnaire and a health assessment (HA). At the HA, participants underwent IOP measurement using Ocular Response Analyser and spectral-domain optical coherence tomography with Heidelberg Spectralis. Participants also underwent a range of anthropometric, ophthalmic, cardiovascular, cognition and blood tests. Participants who attended the HA and had a vertical cup-to-disc ratio (VCDR) measurement in at least one eye were eligible for the study. Participants without any IOP or cRNFL measurements were excluded from the respective analyses.
Results There were 3221 participants eligible for this study (5753 eyes included in the IOP analysis and 5461 eyes included in the cRNFL analysis). The mean (SD) Goldmann correlated IOP (IOPg) was 15.39 mm Hg (3.55 mm Hg). The mean (SD) average global cRNFL thickness was 94.39 µm (11.18 µm). Increased IOPg was associated with increased age, male sex, hypertension, refractive error (myopic decrease in spherical equivalent) and increased corneal resistance factor, while beta-blocker drug use was associated with lower IOPg in the fully adjusted multivariate analysis. Thinner average global cRNFL was associated with Alzheimer’s disease in the age-adjusted and sex-adjusted model. In the fully adjusted multivariate analysis, increased age, male sex, left eyes, hypertension, increased VCDR, refractive error (myopic decrease in spherical equivalent) and increased IOPg were associated with thinner average global cRNFL, while Parkinson’s disease and current (vs never) smoking status were associated with thicker average global cRNFL.
Conclusions Increased IOP and reduced cRNFL were associated with increased age, myopic refractive error, male sex and hypertension. Alzheimer’s disease was associated with thinner average global cRNFL, while Parkinson’s disease was associated with thicker average global cRNFL.
- Glaucoma
- Anatomy
- Retina
- Intraocular pressure
- Diagnostic tests/Investigation
Statistics from Altmetric.com
INTRODUCTION
High intraocular pressure (IOP) is a risk factor for the development and progression of glaucoma.1 As it is the only known modifiable factor, it is important to understand the systemic and ocular factors that are associated with IOP. This may give further insight into the pathophysiology underlying raised IOP which could lead to the generation of candidate targets for the treatment of glaucoma. A recent European Eye Epidemiology (E3) Consortium meta-analysis that included 46 081 participants from 12 cross-sectional studies across Europe studied the distribution and associations with IOP.2 However, the study participants in the two UK-based studies included in the E3 meta-analysis were not drawn from population representative samples. The UK Biobank study reported the distribution and associations with IOP in over 110 000 participants; however, the study had a very low response rate and largely relied on self-reported comorbidities for the analysis of associations.
Spectral-domain optical coherence tomography (SD-OCT) is currently the most commonly used automated imaging technique for the quantification of structural damage in glaucoma. SD-OCT scans are objective, precise and reproducible. Circumpapillary retinal nerve fibre layer (cRNFL) thickness measurement is recognised as a biomarker which is sensitive for the detection of glaucoma. A number of population-based and clinic-based studies have reported the distributions and associations with average global cRNFL thickness using various SD-OCT devices.3– 6 A recent E3 Consortium meta-analysis that included 16 084 participants from 8 cross-sectional studies across Europe investigated the distribution and associations with average global cRNFL thickness.7 However, the study participants in the UK-based study which was included in the E3 meta-analysis were not drawn from a population representative sample.
The Northern Ireland Cohort for the Longitudinal Study of Ageing (NICOLA) is a relatively large population-based study in the UK. It has a well-defined cohort and is well characterised for multiple potentially relevant factors in the analysis of associations with IOP and cRNFL. The objectives of this study are( 1) to describe the distributions of IOP parameters and cRNFL thickness parameters and (2) to explore the factors associated with IOP parameters and average global cRNFL thickness in the NICOLA study.
METHODS
NICOLA is an ongoing longitudinal cohort study of ageing in a sample of the Northern Ireland population aged 50 years or older. The sampling strategy identified addresses within postcode-based geographic regions (geographic stratification). A fixed interval (systematic) sample was drawn from each postcode-based geographical stratum.8 The NICOLA assessment comprised three elements: (1) a computer-assisted personal interview conducted at the participant’s home by a trained interviewer, (2) a self-completion questionnaire that included the 9-item National Eye Institute Visual Function Questionnaire and (3) a health assessment (HA) including a range of anthropometric, cardiovascular, cognition and blood tests, and an ophthalmic component which was performed at the Northern Ireland Clinical Research Facility.
Data collection for the NICOLA study began in February 2014 and ended in 2018. Details of NICOLA study assessments including the ophthalmic component of the NICOLA study HA can be found in supplementary methods 1 in the online supplementary material and at https://www.qub.ac.uk/sites/NICOLA/.
Supplemental material
Briefly, the HA included ophthalmic history, visual acuity testing with ETDRS LogMAR charts, autorefraction, IOP and corneal biomechanics measurement, retinal stereophotography, SD-OCT scans, anthropometric tests, cardiovascular measurements, blood tests and cognitive testing with the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MCoA).
cRNFL thickness measurements were acquired with the Heidelberg Spectralis SD-OCT device (Heidelberg Engineering, Heidelberg, Germany) using a fixed 12° circle scan and IOP measurements were acquired with the Ocular Response Analyser (ORA; Reichert Ophthalmic Instruments, Depew, New York, USA).
NICOLA participants who attended the HA and had a vertical cup-to-disc ratio (VCDR) measurement in at least one eye were eligible for inclusion in this study. NICOLA participants with a self-reported history of age-related macular degeneration or diabetic retinopathy were excluded from the cRNFL analyses. The prevalence of glaucoma in the NICOLA cohort has been published recently.9
Scans judged to have significant artefact (cropped cRNFL, scans not centred on optic disc) or to be grossly abnormal (significant vitreoretinal traction, hyporeflective intraretinal spaces, epiretinal membrane) were excluded from the analysis. Scans with a proprietary quality score <15 were also excluded from the analysis.
This study was conducted according to the tenets of the Declaration of Helsinki. Ethical approval was obtained from the School of Medicine, Dentistry and Biomedical Sciences Ethics Committee, Queen’s University Belfast and the Northern Ireland’s Health and Social Care Research Ethics Committee A (REC A) (REC reference: 16/NI/0247).
Statistical analysis
Summary statistics for baseline continuous variables (Goldmann correlated IOP (IOPg), corneal compensated intraocular pressure (IOPcc) and cRNFL) and frequencies of categorical characteristics (cRNFL normative database classifications) are reported.
To assess epidemiological associations, IOP, IOPg and IOPcc were each considered as dependent variables in separate linear regression analyses with Generalised Estimating Equations (GEE). The independent variables included in the univariate analyses are described in supplementary methods 2 in the online supplementary material. A linear model with identity link function was used. Subject variables were ‘NICOLA participant identifiers’ and within-subject variables were ‘eyes’ which allowed both eyes of each participant to be included in the analysis while accounting for within-subject correlation. Within-subject level variables were eligible as independent variables within the multivariate analysis. An independent working correlation matrix was selected and a robust estimator was selected to be robust against misspecification of the working correlation matrix.
In each multivariate analysis, we adjusted independent variables from the univariate analysis which were statistically significant at the p<0.05 level for the variables age and sex (Model 1). Independent variables from Model 1 that were statistically significant at the p<0.05 level including age and sex were entered into a multivariate model, with reverse stepwise removal of the least statistically significant at each step. Once reverse stepwise removal of variables was completed, the final multivariate model was determined (Model 2). A p value <0.05 was considered statistically significant.
To assess epidemiological associations with cRNFL thickness, average global cRNFL thickness was considered as the dependent variable in the univariate analysis using linear regression with GEE. The independent variables included in the univariate analysis for the average global cRNFL thickness models are described in supplementary methods 2 in the online supplementary material. Multivariate regression analysis for average global cRNFL thickness followed similar steps as Model 1 and Model 2 in the multivariate regression analysis for IOP parameters. Statistical analysis was performed using a software program (IBM SPSS Statistics for Windows, Version 24.0., IBM Corp,Armonk, New York, USA ).
RESULTS
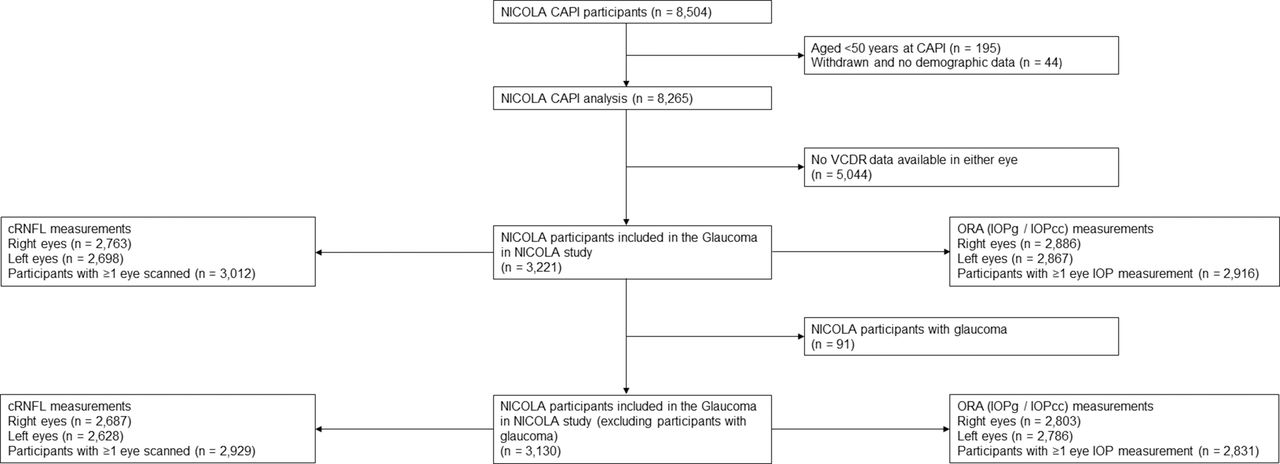
The baseline characteristics of 3221 participants included in the analysis have been reported in detail elsewhere.9 In brief, the mean age of included participants was 64.4 years (SD 8.5 years) and 51.7% were women. There were 91 participants diagnosed with glaucoma and there were 3130 participants without a glaucoma diagnosis. A flow diagram of NICOLA participants and numbers of IOP and cRNFL measurements is outlined in figure 1.

Flow diagram of NICOLA participants and numbers of intraocular pressure (IOP) measurements and circumpapillary retinal nerve fibre layer (cRNFL) measurements.
CAPI, computer-assisted personal interview; cRNFL, circumpapillary retinal nerve fibre layer; IOPcc, corneal compensated intraocular pressure; IOPg, Goldmann correlated intraocular pressure; NICOLA, Northern Ireland Cohort for the Longitudinal Study of Ageing; ORA, Ocular Response Analyser; VCDR, vertical cup-to-disc ratio.
The distributions of IOP measurements are reported in table 1 and figure 2. The mean (SD), 97.5th percentile and 99.5th percentile for IOPg and IOPcc were 15.39 mm Hg (3.55 mm Hg), 23.53 mm Hg and 26.97 mm Hg, and 16.19 mm Hg (3.39 mm Hg), 23.77 mm Hg and 27.40 mm Hg, respectively. The distributions of cRNFL thickness measurements are reported in table 2. The mean (SD), 5th percentile and 1st percentile for cRNFL were 94.39 µm (11.18 µm), 76.00 µm and 64.00 µm, respectively. Summaries of Heidelberg Spectralis proprietary overall scan classifications and average global thickness classifications reported as ‘outside normal limits (ONL)’ and ‘borderline (BL) or ONL’ are shown in table 3. The proprietary normative database generated an ‘ONL’ classification in 12.2% of NICOLA participants and a ‘BL or ONL’ classification in 32.5% of NICOLA participants.
Mean and percentile distributions of intraocular pressure measurements
Mean and percentile distributions of spectral-domain optical coherence tomography average global circumpapillary retinal nerve fibre layer thickness measurements
Classifications of circumpapillary retinal nerve fibre layer (cRNFL) thickness according to Heidelberg Spectralis proprietary normative database for overall classification and average global thickness. Red=outside normal limits; yellow=borderline

{kind=link}
{kind=link}
Histograms of the population distributions of Goldmann correlated intraocular pressure (IOPg; left) and corneal compensated intraocular pressure (IOPcc; right).
Univariate and multivariate analysis models for associations with IOPg and IOPcc are reported in table 4. In the fully adjusted IOPg multivariate model, increased age, male sex, hypertension, refractive error (myopic decrease in spherical equivalent) and increased corneal resistance factor were associated with higher IOPg, while, beta-blocker drug use was associated with lower IOPg. Glaucoma was associated with significantly higher IOPg in the univariate and age-adjusted and sex-adjusted model. In the fully adjusted IOPcc multivariate model, hypertension was associated with higher IOPcc, while increased age, beta-blocker drug use and increased CH were associated with lower IOPcc. Glaucoma was associated with significantly higher IOPcc in the univariate and age-adjusted and sex-adjusted model.
Univariate and multivariate analysis of associations with Goldmann correlated intraocular pressure (IOPg) and corneal compensated intraocular pressure (IOPcc)
Univariate and multivariate analysis models for associations with cRNFL are reported in the online supplementary table. In the fully adjusted cRNFL thickness multivariate model, increased age, male sex, left eyes, hypertension, increased VCDR, refractive error (myopic decrease in spherical equivalent) and increased IOPg were associated with thinner average global cRNFL thickness, while Parkinson’s disease and current (vs never) smoking status were associated with greater average global cRNFL thickness. Glaucoma and Alzheimer’s disease were associated with significantly reduced average global cRNFL thickness in the univariate and age-adjusted and sex-adjusted model.
Supplemental material
DISCUSSION
In this study, we reported the distributions of and associations with IOP and cRNFL thickness measurements in a large population-based study. The aim of our analysis was to identify important ocular, systemic and sociodemographic factors which may confound the interpretation of IOP and cRNFL thickness measurements.
The mean IOPg (15.39 mm Hg) in the NICOLA study was comparable to the E3 population IOP average of 14.8 mm Hg which included various types of tonometry in the meta-analysis.2 The 97.5th and 99.5th percentiles for IOPg were 23.53 mm Hg and 26.97 mm Hg, respectively, and 2 SD above the mean IOPg was 22.49 mm Hg.
As the E3 pooled populations used various methods and devices to measure IOP, the results may not be directly comparable with ORA-derived IOP in the NICOLA study. The UK Biobank and the EPIC-Norfolk eye studies are two UK-based studies which also used ORA to measure IOP. The mean IOP in the NICOLA study was comparable to the UK Biobank study.10 However, our mean IOPg was lower than that reported in the European Prospective Investigation of Cancer (EPIC)-Norfolk eye study (IOPg 16.00 mmHg)11
The epidemiological associations with IOP in the NICOLA study are in broad agreement with findings from other population-based studies and meta-analyses.2 11 12 We reported that increased age was associated with higher IOPg which agreed with the UK Biobank study. However, the EPIC-Norfolk eye study reported that increased age was associated with lower IOPg in multivariate analysis. We reported that increased age was associated with lower IOPcc. The opposing findings for IOPg and IOPcc in the NICOLA study may reflect the different characteristics of the two parameters which are influenced by corneal biomechanical properties. It has been proposed that the measurement of IOPcc is less influenced by the effect of central corneal thickness (CCT); however, CCT was not measured in NICOLA participants.
We reported that male sex and refractive error (myopic decrease in spherical equivalent) were associated with higher IOPg which agreed with the E3 population and the UK Biobank study.2 12 We reported that hypertension was associated with increased IOPg in the final multivariate model and increased systolic blood pressure and diastolic blood pressure were associated with increased IOPg in the age-adjusted and sex-adjusted model. These findings are also consistent with findings from the E3 pooled population, the EPIC-Norfolk eye study and the UK Biobank study.2 11 12
In the NICOLA study, the average mean global cRNFL thickness was 94.39 µm. This is comparable to the mean average global cRNFL thickness in other population-based and clinic-based studies which used the Heidelberg Spectralis device.7 13
The age-related decrease in average global cRNFL thickness was −0.14 µm per year in the fully adjusted multivariate model which was lower than pooled E3 population estimates (−0.35 µm per year, 95% CI −0.60 µm, −0.10 µm per year).7 Male sex, myopic refractive error, increased IOP and hypertension were associated with decreased cRNFL thickness in our study. The direction and significance of these associations are in agreement with those found in the E3 population pooled associations.7 Left eyes were associated with thinner cRNFL compared to right eyes in the multivariate model, but the difference is small and unlikely to be clinically significant.
In our study, self-reported Alzheimer’s disease was associated with significantly thinner cRNFL and this remained significant following adjustment for age and sex. Notably, Alzheimer’s disease was not associated with as much of a reduction in cRNFL thickness compared to glaucoma in the age-adjusted and sex-adjusted model. Alzheimer’s disease was not entered into the final multivariate regression model due to insufficient case numbers which made the model unstable.
Self-reported ‘dementia’ was not associated with thinner cRNFL in our univariate analysis; however, this heterogeneous classification may have included vascular, Lewy body and frontotemporal dementias that may affect the cRNFL in different ways. MCoA score <26, which has been reported to be sensitive and specific for detecting mild cognitive impairment (MCI),14 was associated with thinner cRNFL in our univariate analysis but not after adjusting for age and sex. We found that lower MMSE was not associated with thinner cRNFL in our univariate analysis. However, MMSE does not have an optimal cut-off score for diagnosis and has limitations such as floor and ceiling effects and limited sensitivity to change.15 16
Meta-analyses have shown that cRNFL is thinner in Alzheimer’s disease and MCI.17 18 Also, the UK Biobank study reported that thinner cRNFL was associated with worse cognitive function and those with thinner cRNFL at baseline were more likely to experience cognitive decline over 3 years.19 In contrast, the E3 population and a Japanese population-based study20 found no associations between average global cRNFL thickness and dementia although dementia did show a trend for thinner cRNFL in the E3 population.7 The conflicting results regarding associations between cRNFL and cognitive decline may be due to different definitions of dementia, different cognitive tests used between studies and different devices used to measure the cRNFL. Future longitudinal studies which examine the association between cognitive decline and retinal parameters (eg, macular OCT retinal thickness, macular pigment, quantitative fundus autofluorescence, retinal vessel parameters, OCT angiography, etc) are warranted in the pursuit of objective, non-invasive, easily quantifiable and potentially composite in vivo retinal biomarkers for the early detection of neurodegenerative diseases such as Alzheimer’s disease.
Self-reported Parkinson’s disease was associated with increased cRNFL thickness, and this remained statistically significant following adjustment for age and sex and in the fully adjusted multivariate model. Parkinson’s disease has been associated with decreased cRNFL thickness and decreased macular ganglion cell complex thickness in previous meta-analyses; however, these included only case–control studies which are susceptible to selection bias and spectrum bias.21 22 A possible explanation for the association between Parkinson’s disease and an increase in cRNFL thickness in this study is not immediately apparent. However, Parkinson’s disease is characterised by accumulation of intracellular aggregates of α-synuclein23 which have been demonstrated in the RNFL.24– 26 Therefore, these proteinaceous accumulations, in the early stage of the disease, may cause beading and swelling of the axonal tissue26 which manifests as thickened cRNFL. Nevertheless, our finding should be interpreted with caution.27
Our finding that current smoking was associated with thicker cRNFL in the NICOLA study was in agreement with the E3 population.7 It has been proposed that inhaled neurotoxins in smokers may lead to axonal swelling during axonal degeneration which may manifest as increased cRNFL thickness. However, nicotinic receptor agonists have also been suggested as neuroprotective in the retina.28– 32 In the Singapore Chinese Eye Study, current smoking was found not to be associated with cRNFL thickness,6 and there remains a possibility that the finding in the NICOLA study is due to a chance finding or residual confounding.
The E3 pooled associations found statistically significant associations between average global cRNFL thickness and body mass index, former smoker status and stroke which were not found in the final multivariate regression model in our study. We found no association between average global cRNFL thickness and ocular perfusion pressure which was in agreement with the Beijing Eye Study.4 33
Our study has several strengths and weaknesses. The comprehensive sociodemographic, ocular and health-related data collection enabled the investigation of associations of IOP and cRNFL thickness with a wide range of relevant variables which were selected following a review of the literature. We used robust definitions of comorbidities such as hypertension, diabetes and high cholesterol which incorporated anthropometric and serum measures rather than relying solely on self-reports. Furthermore, we explored psychometric definitions of cognitive decline in addition to self-reported outcomes. There was a robust quality assurance procedure for each cRNFL scan which was consistent with the obvious problems (O), poor signal strengh (S), centration of scan (C), algorithm failure (A), retinal pathology (R), illumination (I), beam placement (B) (OSCAR-IB) consensus criteria for retinal OCT quality assessment,34 and we used the mean of three ORA readings to measure IOP. The large sample size in the NICOLA study and the use of both eyes in multivariate analysis with GEE provided enough power to find epidemiological associations with IOP and cRNFL thickness. This study uncovered some novel associations with cRNFL thickness and some associations that agreed with other population-based studies and meta-analyses. However, it should be emphasised that many statistical tests were performed in the univariate analysis and there is a possibility that some associations represent type I errors. Some of the associations that were found were of modest magnitude and of unknown clinical significance. Also, the cross-sectional design of this study limits causal inferences. Longitudinal follow-up of the NICOLA cohort would provide further insight into the potential causal nature (or otherwise) of the associations. Further weaknesses of our study include that we did not investigate associations with or adjust for topical IOP-lowering medication use or CCT which are important considerations in the management of glaucoma and quantification of IOP.
In conclusion, we have demonstrated that increased IOP and reduced cRNFL thickness are associated with increased age, myopic refractive error, male sex and hypertension. These findings accord with those reported in other population-based studies and meta-analyses. Novel associations between increased cRNFL thickness and Parkinson’s disease and current smoking status may warrant further research.
REFERENCES
Footnotes
Twitter @ruth_hogg.
Acknowledgements We are grateful to all the participants of the NICOLA Study, and the whole NICOLA team, which includes nursing staff, research scientists, clerical staff, computer and laboratory technicians, managers and receptionists. The authors alone are responsible for the interpretation of the data and any views or opinions presented are solely those of the authors and do not necessarily represent those of the NICOLA Study team.
Contributors PMcC: acquisition, design, analysis, interpretation of data, drafting the work, final approval. RH: conception, design, acquisition, analysis, interpretation of data, drafting the work, final approval. DMW: analysis, interpretation of data, final approval. TP: conception, interpretation of data, drafting the work, final approval. SC: design, analysis, drafting the work, final approval. BMcG: design, analysis, drafting the work, final approval. ISY: conception, design, interpretation of data, drafting the work, final approval. FK: conception, design, interpretation of data, drafting the work, final approval. AA-B: conception, analysis, interpretation of data, drafting the work, final approval.
Funding The Atlantic Philanthropies, the Economic and Social Research Council, the UKCRC Centre of Excellence for Public Health Northern Ireland, the Centre for Ageing Research and Development in Ireland, the Office of the First Minister and Deputy First Minister, the Health and Social Care Research and Development Division of the Public Health Agency, the Wellcome Trust/Wolfson Foundation and Queen’s University Belfast provide core financial support for NICOLA. Belfast Association for the Blind provided core financial support for the follow-up visit for expert glaucoma diagnosis and perimetry. The sponsors and funding organisations had no role in the design or conduct of this research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- At a glance