Article Text

Abstract
Aim To report long-term outcomes on best-corrected visual acuity (BCVA) and treatment intervals with a treat-and-extend (T&E) regimen in patients with neovascular age-related macular degeneration (nAMD).
Methods This observational study included treatment-naïve patients with nAMD, treated with aflibercept. A specific T&E protocol without a loading phase and predefined exit criteria was administered. After reaching predefined ‘exit-criteria’, the treatment period was complete, and patients were observed three monthly.
Results Eighty-two patients with a follow-up period of ≥2 years were included. BCVA (mean±SD, ETDRS letters) increased from 51.9±25.2 at baseline to 63.7±17.7 (p<0.0001) at 1 year, 61.7±18.5 (p<0.0001) at 2 years, 62.4±19.5 (p<0.0001, n=61) at 3 years and remained insignificantly higher than baseline at 4 years at 58.5±24.3 (p=0.22). Central subfield thickness (mean±SD, μm) decreased significantly from 387.5±107.6 (p<0.0001) at baseline to 291.9±65.5 (p<0.0001) at 1 year, and remained significantly lower until 4 years at 289.0±59.4 (p<0.0001). Treatment intervals (mean±SD, weeks) could be extended up to 9.3±3.1 weeks at 1 year and remained at 11.2±3.5 weeks at 4 years. Twenty-nine (35%) patients reached exit criteria and continued with three monthly observation only.
Conclusions After 4 years of treatment, initial vision gains were maintained with a reasonable treatment burden, even without an initial loading phase. Our results on functional outcomes are comparable with large controlled studies.
- Neovascularisation
- Retina
- Vitreous
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Intravitreal injections (IVTs) of anti-vascular endothelial growth factor (VEGF) are important to preserve visual acuity in patients with neovascular age-related macular degeneration (nAMD). Large studies have shown the benefits of frequent injections of anti-VEGF agents and the hereby- prevented socioeconomic impacts, considering the high worldwide prevalence of nAMD.1–4 In spite of the excellent therapeutic options, the associated regular injections and visits represent a burden for the often elderly and multimorbid patients.5 As a reaction to the rigid treatment protocols of the pivotal studies with long-term monthly injections, individualised regimens are increasingly popular in daily clinical practice.
In contrast to ‘pro re nata’ (PRN) protocols that usually mandate monthly visits, ‘treat-and-extend’ (T&E) regimens include a disease activity evaluation as well as an IVT of the anti-VEGF agent at every visit. After a loading phase (either two or three monthly injections), predefined stability criteria, evaluated with optical coherence tomography (OCT), and best-corrected visual acuity (BCVA) ensure standardised extension of the visit intervals and injections to up to 16 weeks, depending on the specific regimens. While it is widely common to use a loading dose of three monthly injections, not all registries included a loading phase.6 7 Noninferiority of one versus three initial doses was demonstrated in PRN settings.2 8 It has been shown that T&E regimens require significantly fewer clinical visits than PRN regimens.6 9–11 In recent years, T&E protocols have increasingly been used in patients with nAMD, and current data on visual outcomes and injection intervals have shown encouraging results.12–15 However, most studies do not exceed beyond 12–14 weeks, and evidence about treatment cessation is scarce. Arendt et al pointed out the usefulness of predefined ‘exit-criteria’, to prevent potential unnecessary lifelong treatment.16 More precisely, patients who meet these stability criteria in three consecutive 16 weekly visits can terminate injections. Regular three monthly control visits allow timely identification of potential recurrence, when treatment should be resumed. Since T&E regimens are relatively new in clinical use, reports about long-term outcomes are scarce, and the debate about the ideal treatment protocol is still ongoing.
In our study, we report functional and anatomical 4-year outcomes from our specific T&E regimen with exit-strategy in patients treated with aflibercept for choroidal neovascularisation (CNV), secondary to age-related macular degeneration.
METHODS
This was a single-centre retrospective observational study conducted at the Department of Ophthalmology at the University Hospital in Bern, Switzerland and included patients first presenting between April 2014 and March 2016. Patients with treatment-naïve, newly diagnosed nAMD with CNV and associated visual impairment without restriction of lesion size were included (table 1). Active nAMD lesions were defined as lesions with either subretinal fluid (SRF) and/or intraretinal fluid (IRF). All patients were started on a T&E protocol for intravitreal treatment with aflibercept (EYLEA, Regeneron, Tarrytown, NY, USA). The study was approved by the local ethics committee (KEK No. 093/13) and was conducted in accordance with the International Conference on Harmonisation—Good Clinical Practice guidelines and in compliance with the Declaration of Helsinki. None of the patients had previous injections with anti-VEGF agents. If both eyes were affected, the first diagnosed eye was included in the study. Unless clinical diagnosis of nAMD was obvious, the diagnosis was confirmed by fluorescein angiography. Open inclusion criteria ensured best possible real-life representation. Patients were excluded if the main visual impairment was not caused by nAMD. These conditions included significant fibrosis, geographic atrophy, late-stage or uncontrolled glaucoma, retinal detachment, visually significant cataract, aphakia, vitreous haemorrhage, proliferative diabetic retinopathy or CNV of any cause other than nAMD. We excluded patients who did not adhere to the treatment schedule, namely if injections were behind schedule >2 weeks, or if BCVA or OCT examination was not possible repeatedly due to incompliance or physical or cognitive incapability.
Demographics and baseline characteristics
T&E regimen
An outline of our Bern T&E protocol has been published previously and is shown in figure 1. Briefly, patients underwent ETDRS visual acuity testing and spectral-domain OCT (Heidelberg Engineering, Heidelberg, Germany) imaging including central subfield thickness (CST) measurement, followed by an IVT of 2 mg aflibercept at each visit. The second injection was administered 4 weeks after the initial treatment. Direct extension of the injection interval by 2 weeks was possible thereafter, if predefined stability criteria were reached. Two independent stability criteria were defined (at least one required): (1) no evidence of any IRF or SRF or sub-retinal pigment epithelium (RPE) fluid in the OCT and (2) SRF <50 μm and/or present sub-RPE fluid, no IRF, AND no change in SRF and sub-RPE fluid with stable BCVA at the third consecutive visit. Treatment intervals were extended until the maximal extension interval of 16 weeks was reached OR stability criteria were no longer fulfilled. Treatment intervals were then shortened by 1 week until stability was reached again. Once stability was reached again, the treatment interval was kept unchanged for the next 6 months. If the patients met the stability criteria at three consecutive visits of 16-week intervals, the ‘exit-criteria’ were met, and the patients terminated the therapy. In the best possible scenario, patients needed 10 injections before treatment completion. Clinical visits without injections ensured disease control after therapy termination. If at any time patients showed signs of recurrent disease, the T&E protocol was resumed from the beginning.

Outline of the Bern treat-and-extend regimen. (A) Treatment algorithm: 4 weeks after the first injection, disease activity evaluation and a second injection take place. In case of stability, extension of the intervals by 2 weeks is triggered. If stability criteria are not fulfilled, a repeat injection takes place 4 weeks later. If patients show signs of active disease at any time, the intervals are shortened by 1 week (asterisk), until disease stability is reached. After shortening of the interval, extension is not possible for the following 6 months. (B) Outline of the best-case scenario with the minimal number of 10 injections in 2 years. nAMD, neovascular age-related macular degeneration.
Statistical analysis
Visual acuity data failed commonly used normality tests (Shapiro-Wilk, D’Agostino-Pearson, Anderson-Darling and Kolmogorov-Smirnov). Therefore, the non-parametric Wilcoxon signed-rank test was used analyse BCVA, CST and treatment interval differences as previously in a similar setting.15 We applied the last-visit-carried-forward principle for missed visits, and patients lost to follow-up were analysed up to the time of dropout and then excluded from statistical analysis. Patients were followed up after cessation of therapy (patients in remission), and their visual acuity and CST data are included in the statistics. Data are presented as the mean±SD, and p<0.05 values were considered statistically significant.
RESULTS
Of the 131 patients with newly diagnosed nAMD, 82 (46 female) were followed up for at least 2 years and included in the study (figure 2). At baseline, the mean age was 81.6±8.8 years (range, 59–97) and 36 (44%) patients were pseudophakic. Table 1 illustrates the demographics and baseline characteristics. The mean duration of the follow-up period amounted to 3.5±0.65 (mean±SD) years, while the mean number of injections of the patients who completed at least 2 years of therapy was 19.2±9.0 (n=82, mean±SD). Sixty-one patients had a follow-up period of at least 3 years, and 50 patients of 4 years.

Flow diagram illustrating the number of patients in the study, according to their treatment-status ‘exit’ or ‘injections’, total number and lost to follow-up. Exit-patients suffering from recurrence went back to injections (asterisk).
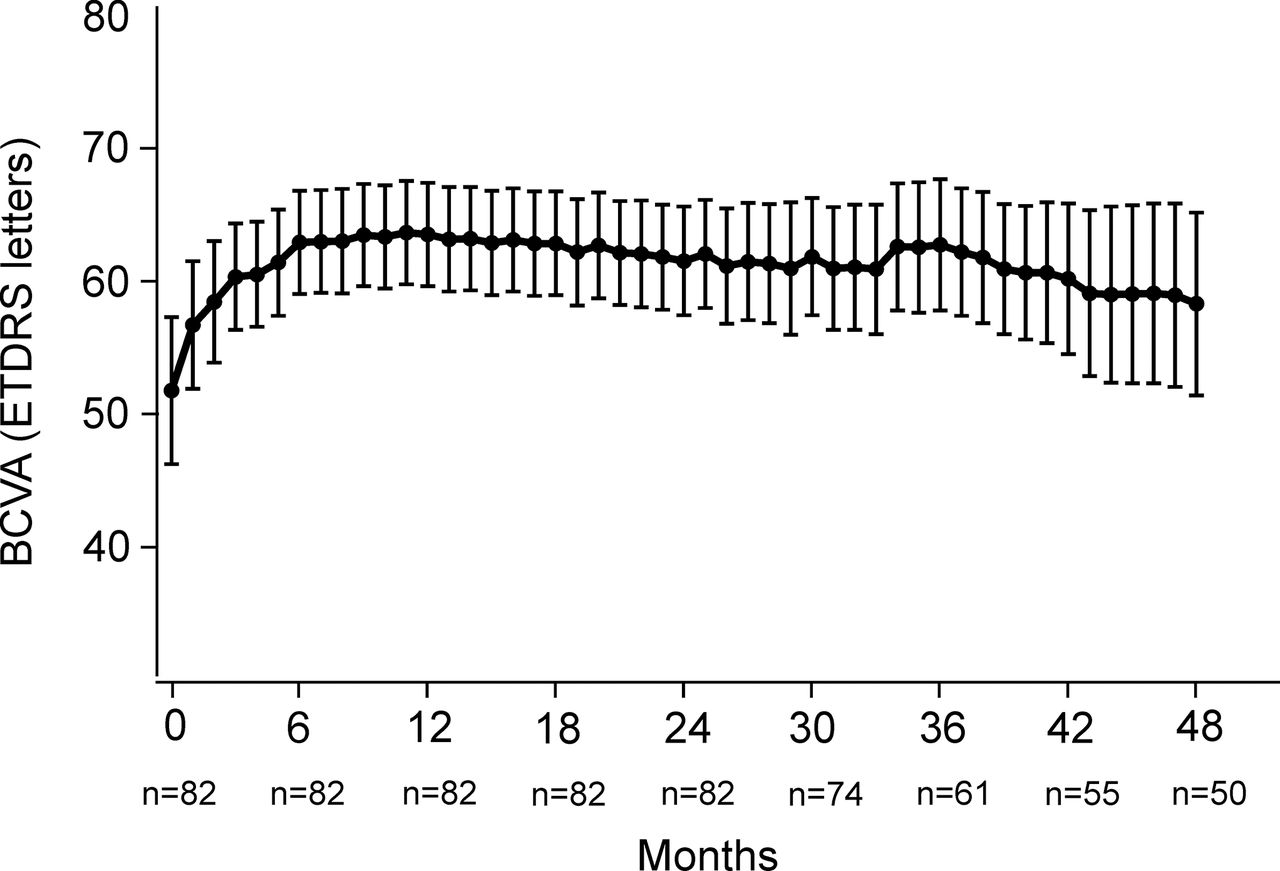
The mean BCVA increased from 51.9±25.2 (mean±SD, median: 60) letters at baseline to 63.7±17.7 letters (+11.8, p<0.0001, median: 68) at 1 year, 61.7±18.5 letters (+9.8, p<0.0001, median: 65) at 2 years, 62.4±19.5 (+10.5, p<0.0001, median: 68) at 3 years, and 58.5±24.3 (+6.6, p=0.22, median: 65) letters at 4 years, as shown in figure 3.
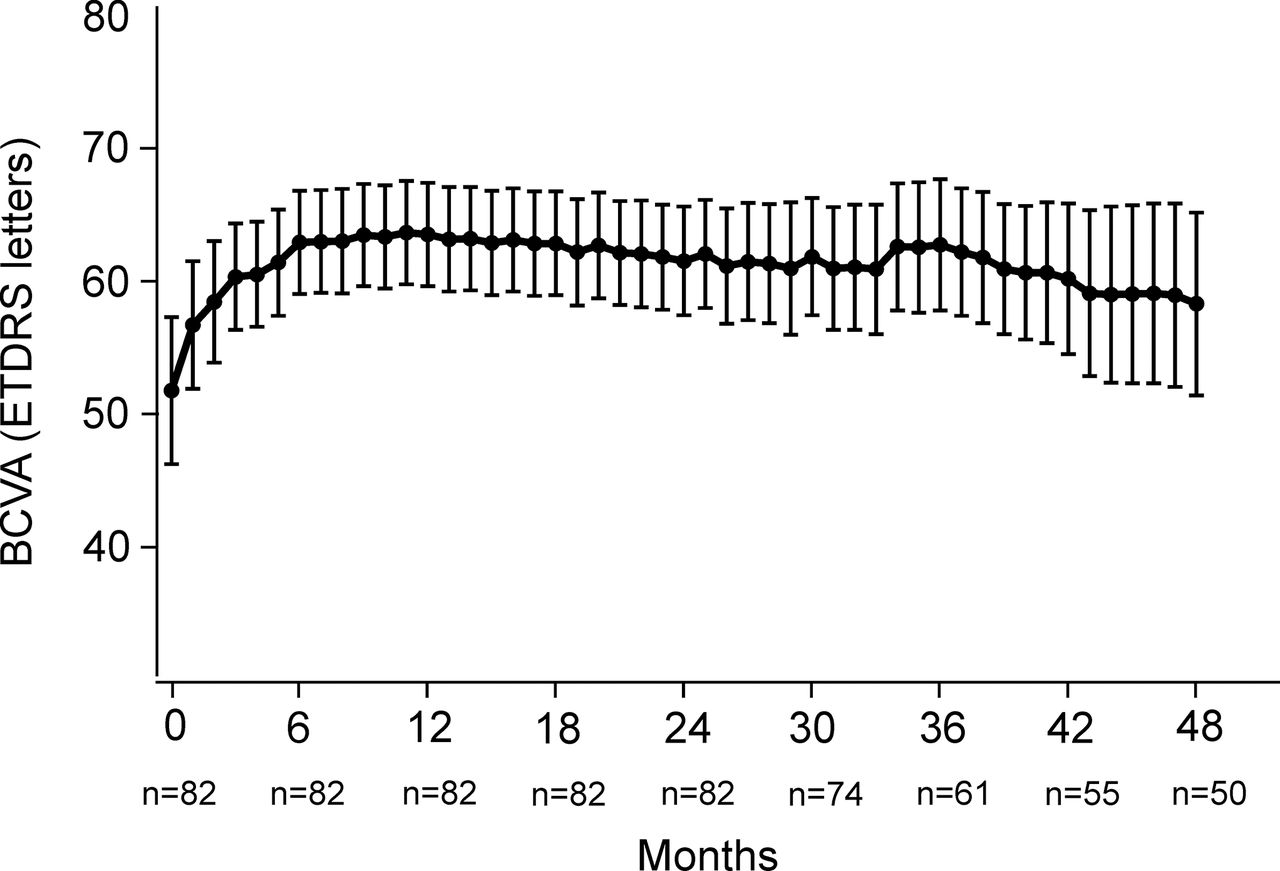
Visual acuity data of all patients (injections+exit) from baseline until month 48. Values are displayed as mean±95% CI. BCVA, best-corrected visual acuity.
The mean CST decreased significantly from 387.5±107.6 μm (mean±SD) at baseline to 291.9±65.5 μm (−95.6, p<0.0001) at 1 year, and remained significantly lower until 4 years at 289.0±59.4 μm (−98.5, p<0.0001), as shown in figure 4.

Central macular subfield thickness data of all patients (injections+exit) from baseline until month 48. Values are displayed as mean±95% CI.
Treatment intervals started at 4 weeks and were extended up to 9.3±3.1 weeks (mean±SD) after 1 year, 12.7±4.2 weeks after 2 years, 11.9±3.9 weeks after 3 years and remained stable at 11.2±3.5 weeks after 4 years, as shown in figure 5. Fifty per cent of the patients reached a median treatment interval of at least 10 weeks (5.2 injections per year). After 2 years, the interval was extended up to a median of 14.0 weeks (3.7 injections per year, n=82). After 3 years, the median interval decreased to 12.6 weeks (4.1 injections per year, n=43), and ended at 11.0 weeks (4.7 injections per year, n=32) after 4 years of treatment. The mean total number of injections for patients under treatment amounted to 8.1±2.0 (n=82) after the first, 13.2±4.1 (n=82) after the second, 19.4±6.6 (n=43) after the third and 24.9±6.8 (n=32) after the fourth year of treatment. The mean number of injections per year amounted to 8.1±2.0 injections (n=82) in the first, 5.5±2.5 injections (n=82) in the second, 4.8±2.5 injections (n=43) in the third and 5.0±1.6 injections (n=32) in the fourth year.

Interval between injections of patients under treatment from baseline until month 48.
Direct extension without loading phase was possible in 42 (51%) of the patients. Two (5%) of these patients had an immediate relapse after initial extension.
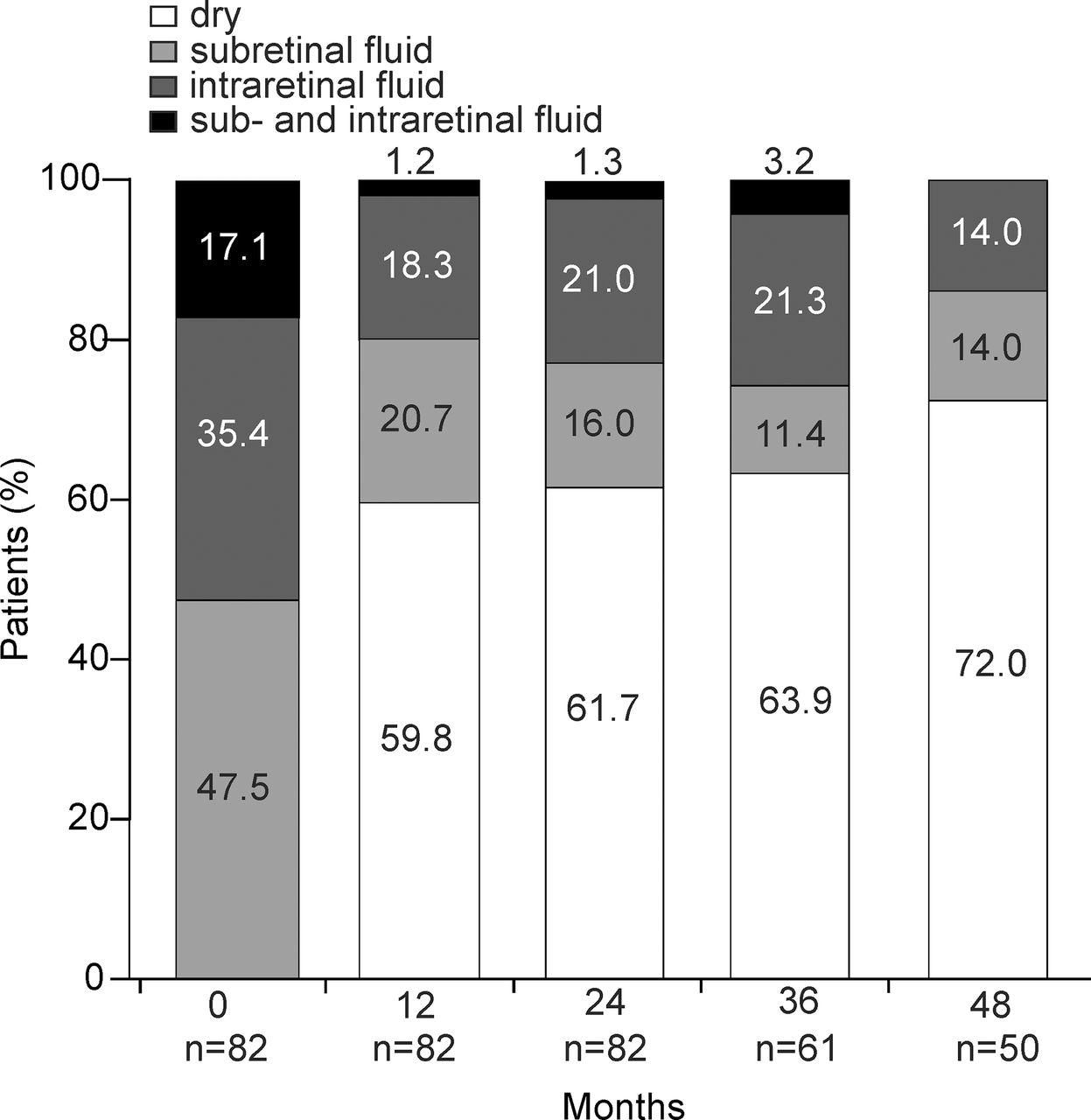
Out of the included 82 patients, 29 (35%) reached the ‘exit-criteria’ and terminated the therapy after 2.6±0.55 (mean±SD) years. Twelve (15%) patients reached the exit-criteria after the minimal number of no more than 10 injections and were considered ‘rapid responders’, whereas 10 and 7 patients reached the exit-criteria in the third and fourth year, respectively. Seventy patients (85%) needed reduction of the treatment interval at least once, or needed more time for the initial extension of the intervals, due to disease activity. The rapid responders did not show significant differences from the other patients in any observed parameter. Visual acuity did not correlate to the injection intervals nor to the total number of injections at any time of the observed period. Qualitative analyses of OCT characteristics are shown in figure 6. At baseline, 47.5% of the patients showed only SRF, 35.4% presented only IRF and 17.1% had both IRF and SRF. After 4 years, 72% of CNVs were inactive, 14.0% had only SRF and 14.0% showed IRF.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Segregation of patients according to OCT findings (dry, subretinal fluid, intraretinal fluid, and subretinal and intraretinal fluid) at each year of follow-up. OCT, optical coherence tomography.
Eight patients (28%) reaching the exit criteria suffered from a recurrence in the observation period, and therapy was resumed after 52.24±25.9 weeks (mean±SD, range: 21.9–111.3). Eighteen (62%) exit patients were followed without recurrence until year 4, two patients went to private ophthalmologists and one died.
DISCUSSION
Our data documents stable visual acuity in most of our followed patients, even after 4 years of follow-up. This finding is comparable to results from other recently published studies.15 17–20 We observed a relatively low baseline vision of 51.9 letters, partially explained by the fact that our clinic often treats patients after referral from local ophthalmologists, and that our inclusion criteria were relatively loose. The excellent mean BCVA gain of 11.8 letters after 2 years was maintained and resulted in a visual acuity of 58.5 letters after 4 years, which is slightly lower than in the VIEW 1 extension study (62.8 letters).19 Our findings are comparable to results from a recent study by Traine et al, conducted in a similar population, where a BCVA gain of 6.0 letters at 2 years and 3.6 letters at 4 years was reported.15 Gayadine-Harricham et al observed a BCVA-improvement of 7.3 letters at 1 year and 6.2 letters at 4 years.21 Another study reported a BCVA gain of 6.6 at 3 years.22 In general, our data support the T&E protocol with extension of the intervals as soon as disease stability is documented. In summary, our visual acuity data are consistent with expectations in this setting.
Our OCT data showed stable long-term CST and suggests a constant proportion of fluid-free retina throughout years 1–4. These findings are again consistent with previous studies.15 23 Furthermore, this supports the hypothesis that the slow decrease in visual acuity from years 1 to 4 is mainly caused by the dry AMD component and fibrosis, but not recurrent activity of the CNV.
Regarding injection frequency, our study results are comparable to the VIEW 1 extension study and the study from Traine et al. An extension of the intervals beyond 14 weeks after 2 years was possible in about 50% of the patients, 40% without recurrence. The option of treatment exit in our study should be considered as well, as it decreases the overall injection frequency when compared to studies lacking this option.
The proportion of 29% of the patients fulfiling the exit-criteria with an acceptable recurrence rate after therapy cessation in this study supports the use of a predefined exit plan and suggests that this T&E algorithm with exit-strategy generates good results with a reasonable treatment burden. It is of great importance to observe patients closely after treatment cessation in order not to miss recurrence. The safety of an exit option was affirmed by a study of Adrean et al. Although a mean of 4 letter loss occurred at recurrence, BCVA completely recovered after treatment was resumed.24 The difference to the report of Arendt et al,16 who reported an exit rate of 12%, might be explained by the fact that this study only included therapy-naïve patients while the study by Arendt et al also included previously treated patients with nAMD. Supposedly, therapy termination should follow a defined algorithm to ensure repeatability and comparability of outcomes in long-term studies. Of note, a meta-analysis by Okada et al on ranibizumab in patients with nAMD suggested superiority of T&E regimen relative to PRN treatment and reported comparable outcomes to monthly dosing regimen.25
Our data furthermore support the usage of a T&E regimen without a loading phase, since disease activity was only observed in two patients after early extension.
This study, however, might be flawed by non-compliance and selection bias. Patients who interrupt therapy in the first 2 years and never return to the clinic would probably suffer worse outcomes that are not accounted for in this analysis. In addition, such patients have a higher risk of recurrence. Also, we cannot speculate about exit patients who were lost to follow-up. These patients might suffer from undetected recurrence. Our high lost to follow-up rate has to be considered when looking at our data. Finally, our results have to be interpreted with caution because of the retrospective nature but encourage the launch of larger prospective studies.
CONCLUSION
This ‘real-life’ report presents long-term results that are largely consistent with prospective controlled multicenter trials and support the use of T&E regimens with exit-strategy but without loading phase in patients with newly diagnosed nAMD. A clearly defined exit-strategy is mandatory to ascertain standardised treatment termination and consistent outcomes.
REFERENCES
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AE: lecturer fees and travel support from Bayer, grant and educational support from Novartis, consultant for Allergan. MM: consultant – Bayer, Gensight, Zeiss; financial support – Bayer; employee – Isarna (CMO). SW: Allergan, Bayer, Novartis, Heidelberg Engineering, Hoya, Optos, Euretina. Martin Zinkernagel: Allergan, Bayer, Novartis, Heidelberg Engineering.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.
Linked Articles
- At a glance