Article Text

Abstract
Background We examined the associations between the 6-year incidence of age-related macular degeneration (AMD) and vision-related quality of life (VRQoL), and the contribution of presenting visual acuity (VA), in an Asian population.
Methods Fundus images from the Singapore Chinese Eye Study, a population-based cohort study (baseline: 2009–2011; follow-up: 2015–2017), were graded using a modified Wisconsin age-related maculopathy grading system. Incident AMD was defined as no baseline AMD in both eyes and early/late AMD in the worse eye at follow-up. Presenting VA was assessed using the logarithm of the minimum angle of resolution chart at 4 m under standard lighting conditions with habitual correction. Multiple linear regression models determined the associations between AMD incidence with changes in the Rasch-transformed scores of the Reading, Mobility and Emotional VRQoL domains of the 32-item Impact of Visual Impairment (IVI-32) questionnaire, adjusted for traditional confounders. The contribution of presenting VA to changes in VRQoL was also estimated.
Results Of the 2251 participants without AMD at baseline (mean age (SD): 57.7 (9) years, 51.4% women), 101 (4.5%) and 11 (0.5%) developed incident early and late AMD at follow-up, respectively. Incident late AMD was associated with significant 30.3%, 32.5% and 30.9% decrements in Reading, Mobility and Emotional IVI scores, respectively. The contribution of presenting VA ranged between 1.62% and 4.35% of the observed decrements. No significant associations were noted with incident early AMD.
Conclusion Incident late AMD had a substantial impact on all aspects of VRQoL, with presenting VA contributing only minimally to this longitudinal relationship.
- vision
Data availability statement
Data are available upon reasonable request. Due to Singapore’s strict data sharing law, any data requests will be considered on a case-by-case basis.
Statistics from Altmetric.com
Introduction
Age-related macular degeneration (AMD), a chronic irreversible retinal disease that results in loss of central vision, accounts for approximately 13% of blindness in older adults.1 The global prevalence of AMD is expected to increase to 288 million by the year 2040,2 with half of all patients predicted to be residing in Asia as a result of an unprecedented age shift consequent to population ageing; as well as the adoption of a westernised lifestyle and diet.2
Numerous cross-sectional studies in Western and Asian populations have consistently shown that both early and late AMD are associated with poorer vision-related quality of life (VRQoL).3–6 Unfortunately, only one population-based cohort study exists evaluating the impact of AMD incidence and progression on VRQoL in elderly Caucasian women.7 This is a critical knowledge gap, as understanding the longitudinal impact of AMD from the patient’s perspective using population-based data is important in informing public health and clinical decisions related to the detection, intervention and long-term management of this visually debilitating disease.8 Indeed, our group has previously demonstrated that preventing the development of vision loss, rather than stopping existing visual deterioration, may be a better strategy to avoid significant decrements in VRQoL in older individuals.9 Importantly, there is also evidence showing that visual acuity (VA) contributes only fractionally to VRQoL reductions in persons suffering from vision loss,10 which has important implications in disease management, as VA is the primary clinical marker by which clinicians assess treatment/intervention efficacy.
To address these gaps, we examined the 6-year associations of AMD incidence and progression with VRQoL, quantified with the 32-item Impact of Visual Impairment (IVI-32) questionnaire, in a population-based Asian Chinese cohort, and explored the contribution explained by the corresponding change in VA experienced by these individuals. We hypothesise that both incidence and progression of AMD will be associated with significant decrements in VRQoL, with greater QoL reductions observed in those with incident (early and/or late) AMD, as those with existing AMD may have developed compensatory strategies to cope with their visual deficits.11 We also postulate, based on previous research conducted, that changes in VA in these individuals will explain at best ~40% of the VRQoL decrements.
Methods
Study design and population
Participants were recruited from the Singapore Chinese Eye Study (SCES), a population-based cohort study of ethnic Chinese individuals living in Singapore. The baseline visit (SCES-1) was conducted between 2009 and 2011,12 while the 6-year follow-up visit (SCES-2) was held between 2015 and 2017.13 Of the 3353 participants recruited at baseline, 321 were ineligible to participate in the 6-year follow-up assessment owing to death, migration to other countries, or the development of severe cognitive or mobility impairments. Of the remaining 3032 eligible individuals, 2661 (87.8% response rate) participated in SCES-2. We excluded 82 without gradable fundus images, 14 with late AMD at baseline and 175 with incomplete covariate data, leaving 2390 participants for inclusion in analyses. All assessments were conducted at the Singapore National Eye Centre, with study protocols following the principles of the Declaration of Helsinki. Written informed consent from participants was obtained prior to study commencement.
Assessment and definition of AMD
Two-field colour fundus photographs of both eyes, one centred on the fovea and one on the optic disc, were taken for all participants using a digital retinal camera (Canon CR-DGi, Canon, Tokyo, Japan) following pupil dilation. AMD was graded using the modified Wisconsin age-related maculopathy grading system14 into early AMD, defined by the presence of any soft drusen and increased/decreased retinal pigment; or the presence of large soft drusen (≥125 µm in diameter) with a large drusen area >500 µm in diameter or large (≥125 µm) indistinct soft drusen in the absence of signs of late AMD; and late AMD, characterised by the presence of geographical atrophy or exudative macular degeneration or both.15 For the purpose of our analyses, incident AMD was defined as absence of any AMD in both eyes at baseline and presence of early AMD or worse in the worst affected eye at follow-up, while AMD progression was defined as the presence of late AMD at follow-up from early AMD in the worse affected eye at baseline.
Assessment of VRQoL
Impact of Visual Impairment-32
The IVI-32 questionnaire comprises three domains that quantify vision-specific functioning, that is, Reading and Accessing Information (‘Reading’) and Mobility and Independence (‘Mobility’); and Emotional Well-being (‘Emotional’).16 17
Rasch analysis was used to assess the psychometric properties of the IVI-32 using the Andrich rating scale model18 with Winsteps software (V.3.92, Chicago, Illinois, USA),19 and to convert raw questionnaire scores into data approximating interval-level measurement20 expressed in log of the odds units, or logits. A higher score indicated better visual ability. Scores were reversed during Rasch analysis so that a high person measure (in logits) indicates that a person possesses a high level of visual ability. In addition, participant data were anchored to item measures and structure calibrations at baseline in order to generate valid pre–post person measures.21 Differential item functioning (item bias) for time (baseline vs follow-up) was then assessed to establish that observed differences between scores were valid indicators of changes over time.22
During Rasch analysis, we found evidence of multidimensionality in the overall scale. As such, we split the IVI into its three component subscales and conducted Rasch analysis separately on each scale. Two misfitting items were deleted from each of the Mobility (items 4 and 5) and Reading (items 1 and 2) scales. Following these minor amendments, all three scales demonstrated good psychometric properties.
Assessment of presenting VA
High-luminance, high-contrast VA was assessed uniocularly, with the participant wearing their habitual correction, using a logarithm of the minimum angle of resolution (LogMAR) chart (Lighthouse International, New York, USA) at 4 m under standard lighting conditions (85 cd/m2). The presenting VA of the better eye for both baseline and follow-up visits was included in analyses based on our previous work comparing the use of worse eye and better eye VA with binocular VA when quantifying the impact of VA loss on VRQoL.23
Assessment of other covariables
Participants underwent a comprehensive, standardised examination to collect clinical and questionnaire data. Trained interviewers administered questionnaires to collect demographic information, sociodemographic characteristics (education, income level, occupation), lifestyle factors (smoking, alcohol), self-reported family and medical history (diabetes, hypertension, thyroid diseases, stroke, cardiovascular disease (CVD), current medication use), in English or Mandarin according to participant preference. Systolic (SBP) and diastolic blood pressure (DBP) were measured two times using a digital BP monitor (Dinamap Pro Series DP110X-RW; GE Medical Systems Information Technologies). A third measurement was obtained if the two previous SBP readings differed by more than 10 mm Hg or if DBP readings differed by more than 5 mm Hg. The average value of the two closest values for each parameter was used in analyses. Hypertension was defined as having an SBP of ≥140 mm Hg or a DBP of ≥90 mm Hg, or self-reported history of hypertension or antihypertensive medication use. Non-fasting blood samples were collected for assessments of haemoglobin A1C (HbA1c), random glucose, and total high-density lipoprotein, low-density lipoprotein cholesterol and triglycerides. All samples were analysed at the Singapore General Hospital Hematology Laboratory. Estimated glomerular filtration rate (eGFR) was also calculated from plasma creatinine using the Chronic Kidney Disease (CKD) Epidemiology Collaboration equation, and CKD was classified as eGFR <60 mL/min/1.73 m2. Diabetes was defined as random glucose ≥11.1 mmol/L, HbA1c ≥6.5%, diabetic medication use or self-reported history of diabetes24 25; while hyperlipidaemia was defined as total cholesterol ≥6.2 mmol/L or lipid-lowering medication use. CVD was defined as self-reported history of angina, myocardial infarction or stroke. Presence of other eye diseases (diabetic retinopathy, cataract, undercorrected refractive error and glaucoma) was assessed using standardised protocols detailed elsewhere.13 14
Statistical analysis
Mean differences in baseline sociodemographic, clinical data and QoL scores between those with no, incident early and incident late AMD were assessed using the analysis of variance for continuous data and χ2 test for categorical data, where appropriate. The associations between AMD incidence and progression with changes in the three VRQoL scores from baseline to follow-up were assessed using multiple linear regression models, adjusted first for age, gender and factors found to be significantly different between those with and without incident AMD, plus variables that are traditionally adjusted for in QoL analyses (model 1). These factors include baseline age, gender, race, baseline better eye presenting VA, baseline QoL (Reading, Mobility and Emotional) scores, education and income levels, presence of any other eye diseases and presence of diabetes, hypertension, CVD and CKD. We then additionally adjusted for the change in better eye presenting VA (model 2). Because of the extremely small number of persons with baseline and follow-up IVI data experiencing AMD progression (N=1), we did not undertake analysis of the association between AMD progression and the three IVI domain scores.
To facilitate interpretation of the β coefficients in a clinically meaningful way, the coefficients were used to calculate the adjusted means for the follow-up QoL outcomes at each disease state (ie, incident early and late AMD; AMD progression), which were then compared against that of the appropriate reference categories (no incident AMD and no AMD progression, respectively). The difference with the reference categories was presented as percentage change and we regarded p values of <0.05 from two-sided tests to indicate statistical significance.
Lastly, we explored the contribution of the change in presenting VA to the change in VRQoL outcomes by examining the difference in the β coefficient between the models without and with presenting VA (ie, model 1 and model 2, respectively), with this difference presented as a percentage of the β coefficient of model 2.
All statistical analyses were performed using the Stata Statistical computer package (STATA Statistical Software, V.16, Statacorp, College Station, Texas, USA).
Results
Of the 2390 individuals included in this analysis (mean age (SD): 58.0 (8.9) years, 51.4% women), 2251 had no AMD in either eye at baseline. At the 6-year follow-up visit, 101 (4.5%) and 11 (0.5%) developed early AMD and late AMD in at least one eye. Of the 139 individuals with early AMD in at least one eye at baseline, only 1 (0.7%) experienced disease progression. Table 1 summarises the above information, together with the corresponding baseline and follow-up VA and QoL scores.
Summary of VA and VF-11 by AMD severity at baseline and follow-up
Table 2 compares the baseline clinical and sociodemographic characteristics of participants with and without incident (early and late) AMD at the 6-year follow-up. We found that those with incident any AMD had worse Reading, Mobility and Emotional scores, and were older, less likely to be women, more likely to have ≤6 years’ education, more likely to have income <SG$2000, and more likely to have hypertension and CKD (all p<0.05).
Comparison of participant baseline sociodemographic and clinical characteristics by AMD incidence
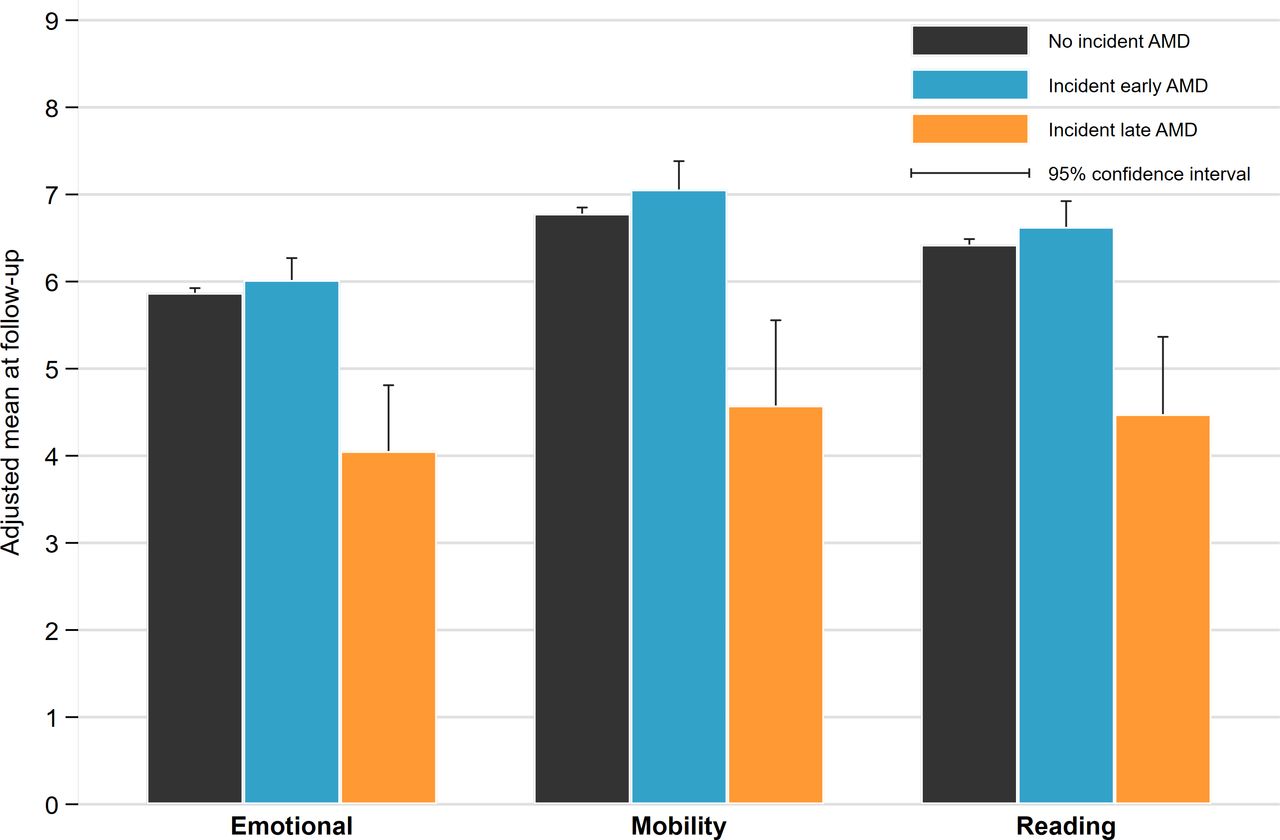
Table 3 shows the associations between AMD incidence (early and late) and the change in the three IVI scores. In multivariable models (model 1), we found that persons with incident late AMD had, on average, a 31.5% (β: −2.02, 95% CI: −2.91 to −1.13; p<0.001), 33.9% (β: −2.30, 95% CI: −3.28 to −1.32; p<0.001) and 31.6% (β: −1.85, 95% CI: −2.61 to −1.10; p<0.001) greater decreases in the Reading, Mobility and Emotional IVI scores, respectively, compared with those without incident late AMD. These associations remained significant even after adjusting for presenting VA (model 2). Conversely, incident early AMD was not associated with greater decrements in any of the VRQoL outcomes. Figure 1 shows the adjusted mean outcome measures at follow-up stratified by disease severity.
{kind=link}
Adjusted mean follow-up quality of life scores by the incidence of AMD. AMD, age-related macular degeneration.
Association between 6-year age-related macular degeneration (AMD) incidence and vision-related quality of life score
Table 4 shows the contribution of better eye presenting VA to these observed decrements in VRQoL outcomes. As can be seen, these contributions range between 1.62% for the Emotional domain, and 4.35% for the Mobility domain. As noted in the Methods section, we did not undertake analyses pertaining to the associations between AMD progression and the three VRQoL domains due to the lack of progression cases in population (N=1).
Comparison of the β coefficient of variation for incident AMD-VRQoL models with and without presenting visual acuity
Discussion
In this study, we found that those who developed late AMD had significantly greater VRQoL decrements compared with those who did not, with change in presenting VA contributing <5% to these observed decrements. Our results suggest that preventing the development of late AMD remains paramount to avert substantial VRQoL deterioration in elderly individuals; and although poor VA is evident in late-stage AMD, there are other non-VA-related contributors (eg, contrast sensitivity changes) that clinicians should pay close attention to when monitoring their patients’ AMD treatment outcomes.
Our finding that only individuals who developed late AMD at the 6-year follow-up visit reported significantly greater decrements in all aspects of VRQoL, as compared with individuals who remained AMD-free at 6 years, supports previously published cross-sectional clinical data from our group showing significant and substantial decrements in Reading, Mobility and Emotional IVI scores in individuals with late AMD.5 Importantly, a change in presenting VA appears to contribute only minimally (<5%) to the above relationship, suggesting that the detrimental impact on VRQoL may be driven by the disease’s deleterious effect on other aspects of the visual system, such as decreased contrast sensitivity and visual distortion.26 The fact that the mean better eye presenting VA of participants who developed late AMD within this 6-year timeframe was 0.27 LogMAR units (equivalent to ~6/12 Snellen acuity) tends to reinforce our findings that relatively good presenting VA is not necessarily associated with good VRQoL. Taken together, our data suggest that the use of standard high-luminance VA as the main clinical marker to assess AMD progression and associated intervention efficacy may warrant re-evaluation as it clearly does not reflect the the impact of the disease on VRQoL.
Our findings, however, contrast with that of the only other prospective population-based Study of Osteoporotic Fractures, which found no significant changes in VRQoL, assessed using the 9-item National Eye Institute Visual Function Questionnaire, in women with incident disease over a 5-year follow-up period.7 In contrast, they observed a significant 13% decline in those that progressed from early to late AMD within this 5-year timespan. While several factors may underlie this disparity in incidence findings, including differences in study sample, assessment methodology and data analytics; we unfortunately did not have enough statistical power to carry out progression analyses (N=1). As such, even though our data appear to support our hypothesis that preventing the development to late AMD is important in maintaining functional vision, larger studies with more progression cases are needed to confirm progression findings and add to the current evidence base.
Contrary to our hypothesis, incident early AMD was not associated with worse VRQoL at follow-up. This is not surprising given that those with early AMD may have few, if any, visual symptoms. This non-significance may have been further compounded by the fact that the IVI-32 was designed to be vision specific, and hence may have been unable to assess more subtle early disease-specific effects, for example, low-luminance visual difficulties and financial concerns related to specialist visits.27 28 As such, the lack of a psychometrically sound AMD-specific QoL instrument to comprehensively quantify the early and/or disease-specific impact of AMD and its related treatments from the patient’s perspective29 is a knowledge gap that needs to be urgently addressed, as research and clinical disease management moves towards personalised and value-based care.30 Our group is currently developing an AMD-specific instrument using item banking and computerised adaptive testing methods that allow for targeted administration of items based on participants’ previous responses.31 Such an instrument would enable a rapid, yet comprehensive assessment of the patient-reported impact of AMD and its associated treatment on QoL outcomes.32
Strengths of our study include its population-based design; a comprehensive and standardised clinical and questionnaire assessment protocol enabling a clear and concise grading of AMD status at baseline and follow-up visits, as well as the ability to adjust for a range of potentially confounding factors; and the use of Rasch analysis to psychometrically validate and transform ordinal questionnaire responses into interval-level measures, hence increasing measurement precision.33 Limitations include the small number of AMD progression cases within our sample (N=1), as well as the low numbers of persons with late AMD (N=11) that precluded attempts to determine how disease progression impacted on VRQoL, as well as whether differential associations exist between the different AMD subtypes (ie, geographical atrophy, neovascular AMD and polyploidal choroidal vasculopathy) and VRQoL. Moreover, our findings were specific only to the Chinese population, and may not be generalisable to Malay and Indian individuals with AMD. In addition, the targeting of the IVI-32 to our population was poor (ie, the items were too ‘easy’ relative to respondent’s ability levels). Although a perennial issue that affects population-based samples, likely because of the low number of persons in the population with visual complaints, this alone should not detract from the significance of our findings. Lastly, our use of the Wisconsin AMD grading system did not allow us to explore the impact of the incidence and progression of intermediate AMD on QoL. Larger cohort studies using more precise AMD grading schemes, such as that used in the Age-Related Eye Diseases cohort studies,34 are needed to address this limitation.
In conclusion, we found that individuals with incident late AMD experienced substantial (>30%) decrements in all aspects of VRQoL compared with those without the disease, with presenting VA contributing only minimally to these decrements. Our results suggest that targeted public health awareness and ocular screening programmes are needed to prevent the development of AMD in the elderly population; and clinicians need to be aware that patients with AMD with good presenting VA may not necessarily have good VRQoL. Moreover, clinicians may also wish to prescribe additional support, in the form of low vision services, occupational therapy or evidence-based psychological counselling, to patients with recent-onset late AMD in order to preserve functional independence in these individuals. In addition, future longitudinal studies in patients with AMD using a comprehensive and sophisticated AMD-specific instrument are needed to fully elucidate the QoL impact of this vision-threatening disease.
Data availability statement
Data are available upon reasonable request. Due to Singapore’s strict data sharing law, any data requests will be considered on a case-by-case basis.
Ethics statements
Patient consent for publication
Ethics approval
The baseline study received approval from the Singapore Eye Research Institute (SERI) Institutional Review Board (R498/47/2006), while the follow-up study was approved by the SingHealth Institutional Review Board (#2015/2279).
References
Footnotes
Contributors Study design: ELL, TYW and C-YC. Study conduct: REKM, NK and ZLT. Provided materials: TYW, ELL and C-YC. Data analysis/interpretation: REKM, ATLG, EKF and ELL. Manuscript drafting: REKM, ATLG and EKF. Manuscript proofing: KYCT, ACST, GCMC, ZLT, NK, TYW, C-YC and ELL.
Funding This research is supported by the Singapore Ministry of Health’s National Medical Research Council (STaR/0003/2008, NMRC/CIRG/1417/2015, NMRC/CIRG/1488/2018 and NMRC/OFLCG/004a/2018), the Singapore Bio Imaging Consortium (C-011/2006) and the Biomedical Research Council (08/1/35/19/550). ELL and C-YC are supported by the National Medical Research Council (NMRC) Senior-Clinician Scientist Awards (#NMRC/CSASI/0009/2016 for ELL; #NMRC/CSASI/0012/2017 for C-YC), and REKM is supported by the NMRC Transition Award (#MOH-TA19may-0002).
Disclaimer The funding bodies had no role in the design and conduct of this research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance