
Abstract
The aim of the study was to enhance our understanding of the pathogenesis of the ataxia of Charlevoix–Saguenay, based on the findings presented herein. Five patients with a molecular diagnosis of this disease underwent clinical, radiological, ophthalmologic and electrophysiological examinations. Five novel mutations, which included nonsense and missense variants, were identified, with these resulting in milder phenotypes. In addition to the usual manifestations, a straight dorsal spine was found in every case, and imaging techniques showed loss of the dorsal kyphosis. Cranial MRI demonstrated hypointense linear striations at the pons. Tensor diffusion MRI sequences revealed that these striations corresponded with hyperplastic pontocerebellar fibres, and tractographic sequences showed interrupted pyramidal tracts at the pons. Ocular coherence tomography demonstrated abnormal thickness of the nerve fibre layer. Electrophysiological studies showed nerve conduction abnormalities compatible with a dysmyelinating neuropathy, with signs of chronic denervation in distal muscles. The authors suggest that the hyperplastic pontocerebellar fibres compress the pyramidal tracts at the pons, and that the amount of retinal fibres traversing the optic discs is enlarged. These facts point to the contribution of an abnormal developmental mechanism in the ataxia of Charlevoix–Saguenay. Accordingly, spasticity would be mediated by compression of the pyramidal tracts, neuromuscular symptoms by secondary axonal degeneration superimposed on the peripheral myelinopathy, while the cause of the progressive ataxia remains speculative. The distinctive aspect of the dorsal spine could be of help in the clinical diagnosis.
Similar content being viewed by others


Introduction
The autosomal recessive spastic ataxia of Charlevoix–Saguenay (ARSACS) is a disease caused by mutations in the SACS gene, located on chromosome 13q12.12 [39]. Believed at first to be restricted to Canada, ARSACS has been diagnosed in various countries afterwards, and the two initial founder mutations identified in the province of Quebec have increased to more than 70, coming from around the world [11, 25, 28].
In this article, the authors present five patients with a molecular diagnosis of ARSACS, together with the results of clinical, radiological, ophthalmologic, electrophysiological and genetic examinations. On the basis of the findings obtained in these studies, a pathogenic hypothesis is proposed, different from the neurodegenerative genesis attributed to this disease.
Patients and methods
Five patients, in whom a diagnosis of ARSACS was suspected, underwent the following procedures:
-
1.
A complete clinical evaluation.
-
2.
An imaging study comprising cranial CT and MRI examinations. Spinal X-ray and MRI scans were done in two patients.
-
3.
An ophthalmologic survey, consisting of visual acuity and field tests, stereophotographs of the optic discs, and retinal nerve fibre layer (RNFL) assessment by monochromatic photography and ocular coherence tomography (OCT).
-
4.
An electrophysiological study that included motor and sensory nerve conduction studies; F wave latencies and blink reflexes. Concentric needle electromyography of proximal and distal muscles was also performed. Somatosensory, auditory, electroretinogram and visually evoked potentials were recorded, as well as sympathetic skin responses.
-
5.
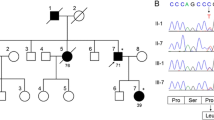
A molecular study, in which total DNA was purified from peripheral blood. The coding exons and flanking introns of SACS were amplified by polymerase chain reaction, purified and bidirectionally sequenced using oligonucleotide primers [12]. The presence of large-scale gene deletions in SACS was ruled out by multiple ligation-dependent probe amplification and quantitative-PCR protocols, described elsewhere [38]. Segregation of mutations with the disease was analyzed in close relatives, whenever possible. New mutations were also ruled out in over 300 ethnically-matched control chromosomes.
This study was approved by the local ethics committee. Every patient gave informed consent for its realization, according to the Declaration of Helsinki.
Results
Clinical findings
The series comprised four women and one man, aged 37–57 years. Every patient displayed pes cavus and hammertoes. In addition, a straight dorsal spine, a posterior flat rib cage with protruding scapulae, together with normal muscle strength in the scapular girdle, were also found (Fig. 1).

a, b Note straight dorsal spine, flat posterior rib cage and protruding scapulae in two patients. Absence of dorsal kyphosis and lack of bone and soft tissue abnormalities in X-ray (c) and MRI (d) scans. Spinal cord atrophy is evident in image D
Patients 1 and 2 experienced a late progression of disease (at 42 and 31 years of age, respectively), after displaying abnormal gait since infancy. On the opposite, patients 3, 4 and 5 suffered progression since disease onset.
Severe spasticity was present in the hips and knees. The patellar reflexes were always preserved, while the achilles and brachioradialis were abolished; only patient 2 had spared distal tendon reflexes. Extensor plantar responses were found in every instance.
Mild distal weakness was present in the upper limbs. In the lower limbs, it was mild in patients 1 and 2, and moderate in the others. Vibration sense was diminished in the lower limbs in patients 1 and 2, and absent in the remaining. Gait was limited to a few steps with bilateral support; only patient 2 retained independent ambulation.
Dysmetria was moderate in patients 1 and 2, and severe in the others. Gaze evoked nystagmus and non-smooth ocular pursuit were present in every case. Mild dystonic posturing of the hands was observed in patient 4.
Radiological findings
T1-weighted sagittal midline cranial MRI scans revealed atrophy of the superior cerebellar vermis, upper cervical cord and cerebral cortex, while the brainstem appeared to be of normal size. Proton density, T2 and fluid-attenuation inversion recovery (FLAIR) axial sequences demonstrated paramedial, bilateral and parallel linear hypointensities in the basis and tegmentum of the pons, together with thick middle cerebellar peduncles.
Single-voxel spectroscopic analyses of the pons, using 1.5 and 3 Tesla machines, verified a mild elevation of the choline/creatine ratio, characteristic of normal white matter. Diffusion tensor colour encoded MRI maps demonstrated: (1) an occupation of the pontine basis and tegmentum by pontocerebellar fibres; (2) thin and abnormally placed pyramidal tracts at the pons; (3) abnormally thick middle cerebellar peduncles; and (4) normal medial lemnisci (Fig. 2).

Diffusion tensor colour MRI maps of the pontine structures (blue, craniocaudal fibres; green, anteroposterior fibres; red, latero-lateral fibres). a, c Normal configuration of the pons in a control subject: pyramidal tracts, medial lemnisci and superior cerebellar peduncles (blue), pontocerebellar fibres (red), and middle cerebellar peduncles (green). b, d In an ARSACS patient, small and laterally placed pyramidal tracts; occupation of the basis and tegmentum pontis by pontocerebellar fibres, and thick middle cerebellar peduncles
Diffusion tensor tractographies showed that the pyramidal tracts were interrupted at the pons, although the pyramids showed a normal size and location at the medulla. An extremely large amount of pontocerebellar fibres was detected, which compressed the pyramidal tracts and gave place to unusually thick middle cerebellar peduncles (Fig. 3).

Diffusion tensor tractographies. a, c, e Normal control appearance of the pyramidal tracts, medial lemnisci and middle cerebellar peduncles. b, d, f Images from ARSACS patients. b Note interruption of the pyramidal tracts at the pons. d Increased number of fibres in the middle cerebellar peduncles. f Greatly increased amount of pontocerebellar fibres, thickened middle cerebellar peduncles and normal appearance of the descending pyramidal tracts
X-ray films revealed a straight spine, an absence of the dorsal kyphosis and a lack of bone abnormalities in the tested patients (Fig. 1c). Dorsal spine MRI scans confirmed these findings, without disclosing soft tissue anomalies (Fig. 1d).
Ophthalmological findings
Normal visual acuities and mild peripheral campimetric non-specific defects were found in every case. Monochromatic photographies showed increased visibility of the RNFL, while OCT demonstrated an increased thickness of this layer, which ranged from 125–220 μm.
Electrodiagnostic findings
The results are presented in Tables 1, 2 and 3. Every tested nerve showed abnormalities of motor and sensory conduction that fell into the demyelinating range. The amplitudes of the motor and sensory potentials were low, although associated with significant increases in the temporal dispersions of action potentials on distal and proximal stimulation, even in the lower limbs.
Minimal F wave latencies and F wave latency chronodispersions were prolonged. So were the blink reflex latencies. Sympathetic skin responses were normal, as reported previously [16].
Electromyography revealed signs of chronic denervation in distal muscles, though not so in proximal ones; the recruitment pattern was reduced in every tested muscle.
Somatosensory, brainstem auditory and visual evoked responses showed increased latencies and prolonged central conduction times, which doubled normal values on occasion.
Molecular findings
Patient 1 exhibited the hemizygous mutation c.13405G > C/p.A4469P, which replaces alanine 4469 for proline in the functionally relevant HEPN domain [4]. The other allele, inherited from her mother, harboured a large genomic deletion (Δ) that encompassed SACS, as described elsewhere [38].
Patient 2 harboured a c.1894C > T substitution (p.R632 W) on the paternal allele, and a c.12973C > T variant (p.R4325X) on the maternal one. The p.R632 W mutation affects a highly conserved residue in sacsin, whereas p.R4325X predicts premature protein truncation.
Patients 3 and 4 were sibs and harboured the nonsense mutation c.832C > T/p.Q278X in compound heterozygosity with c.9670C > T/p.R3224X on the paternal allele; both variants predict sacsin truncation at positions 278 and 3,224, respectively.
Patient 5, an offspring of consanguineous parents, demonstrated the homozygous mutation c.3198T > A/p.C1066X, which predicts early sacsin truncation. Each parent carried the mutation in heterozygous form.
Discussion
ARSACS usually presents with early onset lower-limb spasticity, cerebellar ataxia, peripheral neuropathy, and skeletal and retinal anomalies [7, 8, 10, 31], in spite of cases with incomplete clinical expression [34] or late onset [5]. Although the resulting clinical picture is easily recognizable, some aspects of the disease need to be defined better, as will be considered below.
In addition to the well-known skeletal abnormalities of pes cavus and hammertoes [8], an alteration of the dorsal kyphosis was observed in every patient presented herein. The dorsal spine appeared straight, and the posterior rib cage flat; and despite an absence of muscle weakness, the superior angles of the scapulae stuck out from the thoracic wall, exhibiting the peculiar appearance shown in Fig. 1. X-ray and MRI scans showed loss of the physiological dorsal kyphosis, without bone or soft tissue anomalies. As scoliosis is the spinal abnormality most frequently associated with spinocerebellar degenerations, the observed straight spine could represent a skeletal anomaly characteristic of ARSACS.
Dystonia has occasionally been reported in ARSACS [39], and abnormal posturing of the hands was noted in patient 4, which did not cause any motor handicap. Thus, dystonia seems to be infrequent and mild in this disease.
MRI scans showed atrophy of the cerebellum, cerebral cortex and spinal cord. A pontine hypointense linear striation was found in every patient; this finding has been claimed as unique to ARSACS [23].
In an effort to determine the nature of the hypointense striation, spectroscopy and diffusion tensor MRI sequences were performed. Although a spectroscopic analysis gave normal results, diffusion tensor maps showed that the hypointense striation corresponded with pontocerebellar fibres, and that the pyramidal tracts were thin and out of their normal location.
Tractographic MRI sequences showed that the pyramidal tracts were interrupted by an abnormally large number of pontocerebellar fibres, which gave the basis pontis a bulky appearance and constituted thick middle cerebellar peduncles.
Tensor diffusion MRI has been used to assess some degenerative ataxias, and atrophy of the nervous structures was found in every case [22, 37, 43]. Thus, the increased amount of pontocerebellar fibres detected in our patients does not suggest a degenerative origin, but would be more evocative of a developmental one. In this case, the pontocerebellar fibres would compress the pyramidal tracts at the pons since the embryonic period, causing spasticity from a very early age, as reported [7–10]. Although the corticospinal tracts were reported to be small at the pons in ARSACS, and the pontine nuclei, preserved, the pontocerebellar fibres were not detailed [7, 9, 10]. Therefore, a review of the pathological findings should be carried out in this disease, in order to confirm the proposed hypothesis.
Most of the pontocerebellar fibres use glutamate as a neurotransmitter [26]. Taking into account the increased amount of pontocerebellar fibres found in the images presented herein, it is plausible that glutamate excitotoxicity could bring about neuronal death in the cerebellar cortex [2, 21, 32]. This phenomenon could be responsible for the cerebellar atrophy evident on MRI scans, and for the progressive ataxia associated with ARSACS, of more tardive appearance than spasticity [7–10]. Damage to the spinocerebellar tracts and the proprioceptive pathways could contribute to the genesis of the ataxia, as well.
Although two spasticity-lacking phenotypes of ARSACS have been described, these have been attributed to the presence of severe muscle hypotonia, not to an absence of spasticity along the disease course. Besides, bilateral Babinski signs were found in these patients, which disclosed the presence of a pyramidal syndrome [33, 34].
An increased visibility of the retinal nerve fibres, which embedded vessels in the peripapillary region, was reported in the original description of ARSACS [8]. Colour stereophotographs and monochromatic photographs showed enhanced visibility of the RNFL in every patient presented here, while OCT demonstrated an increase in average thickness of the RNFL, which ranged from 125 to 220 μm, as compared with a mean of 96 ± 7 μm in healthy volunteers [17, 29]. Increased thickness of the RNFL has also been described by other authors, with the use of OCT [13, 41]; an enlarged amount of nervous fibres probably accounts for these findings.
Visual acuity was normal herein, and only mild and peripheral visual defects were found. These results rule out the possibility of deposition of myelin in the retina, because myelin, being opaque to light, would have caused severe loss of visual acuity, as well as significant campimetric defects.
The issue of the peripheral nerve participation in ARSACS has not been definitely established. It has been claimed to be a myelinopathy [31], an axonopathy [12, 14], or a disease bearing similarity with the intermediate forms of Charcot–Marie–Tooth neuropathy [6, 16].
Our electroneurographic findings (Table 1) showed that, when action potentials were found, the majority of motor and sensory nerves disclosed abnormalities of conduction that fell into the demyelinating range. Distal motor latencies were prolonged, and minimum F wave latencies and chronodispersions, increased. A noteworthy finding was an increase in the distal, and also in proximal–distal, temporal dispersions of the action potentials, which was found in most of the motor and sensory nerves that could be tested. This result indicates that fast and intermediate myelinated fibres did not exhibit uniform nerve conduction velocities, and means that the damage to the myelin sheath had a multifocal distribution [35, 36].
A multifocal pattern of involvement has been found in anomalies of myelin metabolism and diseases of Schwann cells, in addition to dysimmune demyelinating neuropathies [20]. It is known that Schwann cells exert influence on axonal properties, and that changes induced by abnormal myelin may cause axonal degeneration at distal regions [18, 24]. In this survey, electromyographic signs of chronic denervation were found in distal muscles of the limbs, though not so in proximal ones (Table 2).
Systematic studies of evoked potentials have seldom been performed in ARSACS. The results in Table 3 show abnormalities in the somatosensory, auditory and visually evoked responses. When these could be obtained, increased latencies and conduction times were found, pointing to abnormal conduction in the central pathways [6], except for normal visual evoked responses in patient 2, which have been previously described in ARSACS [16].
To summarize, the electrophysiological findings were consistent with a peripheral and central myelinopathy, as demonstrated by the slow conduction velocities and increased temporal dispersion of action potentials in the peripheral nerves, and the prolongation of latencies and central conduction times in the evoked responses. A superimposed peripheral axonal involvement was also present, as mentioned above. These results are in line with those reported previously, which proposed that the neuropathy in ARSACS was caused by a developmental defect of myelination, to which a degenerative process of peripheral axons was added [31]. Therefore, it seems certain that sacsin must exert some influence on central and peripheral myelin, although its presence in the peripheral nervous system has not been examined yet.
ARSACS is caused by recessive mutations in the SACS gene, located on chromosome 13q12.12 [39]. It has one large exon with an open reading frame of 11.487 nucleotides [15], eight newly identified 5′ smaller exons [27], and at least a non-coding one [40]. The nine exons consist of over 15.000 bp and encode sacsin, a 4.579 amino acid protein [39, 40]. This contains an N-terminus ubiquitin-like (UbL) domain (amino acids 1–124), able to interact with the proteasome [30], a J domain (which is the defining feature of the Hsp40 family of Hsp70 co-chaperones) between amino acids 4322–4370, and a C-terminus HEPN domain involved in nucleotide binding, between residues 4,451 and 4,567 [4]. Sacsin also contains an N-terminus recurring arrangement of three adjacent 360 amino acid domains, which has been termed “sacsin repeating region”. This kind of repeating regions are usually placed in proteins that contain a C-terminus J domain [3].
SACS mRNA has been detected by in situ hybridization in all areas of the human brain, especially in the cerebral cortex, hippocampus and cerebellum, and also in pancreas, connective tissue and skeletal muscle [15].
The mutations in SACS presented in this work are novel, except for p.R4325X [1, 42], and were not detected in over 400 Mediterranean control chromosomes. The affected residues are conserved during evolution, and very likely make these new variants disease-causative. Although functional analyses were not possible, in silico predictions using the HumVar-trained PolyPhen2 v2.0, anticipated that the new changes were probably pathogenic [11]. Although it has not been possible to establish a precise genotype–phenotype correlation in ARSACS [5], it seems clear that in this observation, patients who harboured missense mutations on one allele displayed milder phenotypes than those who bore nonsense ones. Unfortunately, the number of patients presented herein is too short to draw a definite correlation.
In conclusion, ARSACS has not demonstrated the behaviour of a degenerative disorder, defined by cell loss and tissue atrophy. Instead, the presence of abnormal amounts of pontocerebellar and retinal fibres would rather suggest a disorder of development in its genesis. As would the electrophysiological records, indicative of a dysmyelinating process. Phenomena derived from these factors could cause spasticity (compression of the pyramidal tracts), ataxia (cerebellar atrophy and spinocerebellar tract dysmyelination), and progression of the neuromuscular manifestations (secondary axonal degeneration). The hypothesis that diseases of development may aggravate after birth, as proposed in this article, has been considered previously [19]. The possibility that ARSACS could be a storage disease has also been taken into account, although extensive metabolic screening did not uncover anomalies [23].
Consequently, the evolution of symptoms in ARSACS is not uniform [9]. Spasticity is present from very early in life and does not seem to worsen. Visual field defects, probably secondary to a disproportionate number of retinal fibres traversing the optic disk, are not symptomatic. In contrast, clinical deterioration is due to an increasing involvement of the cerebellum and peripheral nervous system, which causes ataxia and weakness.
The role played by sacsin in the manifestations of ARSACS remains to be established; however, it seems apparent that nonsense mutations with a loss of function are associated with more severe progressive symptoms.
Our pathogenetic proposal needs confirmation by means of studies that corroborate the results presented in this article, while the relevance of the molecular findings awaits further functional tests.
Finally, the distinctive aspect of the straight dorsal spine could be an aid in the clinical diagnosis of ARSACS.
References
Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, Bork P, Kondrashov AS, Sunyaev SR (2010) A method and server for predicting damaging missense mutations. Nat Methods 7:248–249
Albin RL, Greenamyre JT (1992) Alternative excitotoxic hypotheses. Neurology 42:733–738
Anderson JF, Siller E, Barral JM (2010) The sacsin repeating region (SSR): a novel HSP90-related supra-domain associated with neurodegeneration. J Mol Biol 400:665–674
Anesi L, de Gemmis P, Pandolfo M, Hladnik U (2010) Two novel homozygous SACS mutations in unrelated patients including the first reported case of parental UPD as an etiologic cause of ARSACS. J Mol Neurosci 43:346–349
Baets J, Deconinck T, Smets K, Goosens D, Van den Bergh P, Dahan K, Schmedding E, Santens P, Rasic VM, Van Damme P, Robberecht W, De Meirleir L, Michielsens B, Del-Favero J, Jordanova A, De Jonghe P (2010) Mutations in SACS cause atypical and late-onset forms of ARSACS. Neurology 75:1181–1188
Berciano J, García A, Infante J (2010) Peripheral nerve involvement in hereditary cerebellar and multisystem degenerative disorders. In: Said G, Krarup C (eds) Peripheral Nerve Disorders. Handbook of Clinical Neurology. Elsevier Sci, Amsterdam (in press)
Bouchard JP (1991) Recessive spastic ataxia of Charlevoix-Saguenay. In: de Jong JMBV (ed) Handbook of Clinical Neurology. Hereditary neuropathies and spinocerebellar atrophies, vol 60. Elsevier Sci, Amsterdam, pp 452–559
Bouchard JP, Barbeau A, Bouchard R, Bouchard RW (1978) Autosomal recessive spastic ataxia of Charlevoix-Saguenay. Can J Neurol Sci 5:61–69
Bouchard JP, Brais B, Dupré N, Rouleau GA (2007) Hereditary ataxias and spastic parapareses in north eastern Canada. In: Brice A, Pulst SM (eds) Spinocerebellar Degenerations. The ataxias and spastic paraplegias. Butterworth Heinemann Elsevier, Philadelphia, pp 222–243
Bouchard JP, Richter A, Melançon SB, Mathieu J, Michaud J (2000) Autosomal recessive spastic ataxia (Charlevoix-Saguenay). In: Klockgether T (ed) Handbook of ataxia disorders. Marcel Dekker, New York, pp 311–324
Bouhlal Y, Amouri R, El Euch-Fayache G, Hentati F (2011) Autosomal recessive spastic ataxia of Charlevoix-Saguenay: an overview. Parkinsonism Relat Disord 17:418–422
Criscuolo C, Banfi S, Orio M, Gasparini P, Monticelli A, Scarano V, Banfi S, Filla A (2004) A novel mutation in SACS gene in a family from southern Italy. Neurology 62:100–102
Desserre J, Devos D, Sautière BG, Debruyne P, Santorelli FM, Vuillaume I, Defoort-Dhellemmes S (2011). Thickening of Peripapillar Retinal Fibers for the Diagnosis of Autosomal Recessive Spastic Ataxia of Charlevoix-Saguenay. Cerebellum. doi:10.1007/s12311-011-0286-x
El-Euch-Fayache G, Lalani I, Amouiri R, Turki I, Ouahchi K, Hung WY, Belal S, Siddique T, Hentati F (2003) Phenotypic features and genetic findings in sacsin-related autosomal recessive ataxia in Tunisia. Arch Neurol 60:982–988
Engert JC, Berube P, Mercier J, Dore C, Lepage P, Ge B, Bouchard JP, Mathieu J, Melançon SB, Schalling M, Lander ES, Morgan K, Hudson TJ, Richter A (2000) ARSACS, a spastic ataxia common in north eastern Quebec, is caused by mutations in a new gene encoding an 11.5-kb ORF. Nat Genet 24:120–125
García A, Criscuolo C, De Michele G, Berciano J (2008) Neurophysiological study in a Spanish family with recessive spastic ataxia of Charlevoix-Saguenay. MuscleNerve 37:107–110
García-Martin E, Pinilla I, Idoipe M, Fuertes I, Pueyo V (2010). Intra and interoperator reproducibility of retinal nerve fiber and macular thickness measurements using cirrus Fourier-domain OCT. Acta Ophthalmol. doi:10.1111/j.1755-3768.2010.02045.x
Hattori N, Yamamoto M, Yoshihara T, Koike H, Nakagawa M, Yoshikawa H, Ohnishi A, Hayasaka K, Onodera O, Baba M, Yasuda H, Saito T, Nakashima K, Kira J, Kaji R, Oka N, Sobue G, the Study Group for Hereditary Neuropathy in Japan (2003) Demyelinating and axonal features of Charcot-Marie-Tooth disease with mutations of myelin-related proteins (PMP22, MPZ and Cx32): a clinicopathological study of 205 Japanese patients. Brain 126:134–151
Landrieu P, Kamoun F (2003) Au carrefour de la pathologie développementale et de la pathologie dégénérative: les maladies cérébelleuses de la première enfance. Démembrement et approche pratique. Rev Neurol 159:382–394
Lewis RA, Sumner AJ (1999) Electrophysiologic features of inherited demyelinating neuropathies: a reappraisal. Ann NY Acad Sci 883:321–335
Lipton SA, Rosenberg PA (1994) Excitatory amino acids as a final common pathway for neurological disorders. N Engl J Med 330:613–622
Mandelli ML, De Simone T, Minati L, Bruzzone MG, Mariotti C, Fancellu R, Savoiardo M, Grisoli M (2007) Diffusion tensor imaging of spinocerebellar ataxias types 1 and 2. Am J Neuroradiol 28:1996–2000
Martin MH, Bouchard JP, Sylvain M, St-Onge O, Truchon S (2007) Autosomal recessive spastic ataxia of Charlevoix-Saguenay: a report of MR imaging in 5 patients. Am J Neuroradiol 28:1606–1608
Martini R (2001) The effect of myelinating Schwann cells on axons. MuscleNerve 24:456–466
Okawa S, Sugawara M, Watanabe S, Toyoshima I (2006) A novel sacsin mutation in a Japanese woman showing clinical uniformity of autosomal recessive spastic ataxia of Charlevoix-Saguenay. J Neurol Neurosurg Psychiatry 77:280–282
Ottersen OP, Walberg F (2002) Neurotransmitters in the cerebellum. In: Manto MU, Pandolfo M (eds) The cerebellum and its disorders. Cambridge University Press, Cambridge, pp 38–48
Ouyang Y, Takiyama Y, Sakoe K, Shimazaki H, Ogawa T, Nagano S, Yamamoto Y, Nakano I (2006) Sacsin-related ataxia (ARSACS): expanding the genotype from the gigantic exon. Neurology 66:1103–1104
Ouyang Y, Segers K, Bouquiaux O, Wang FC, Janin N, Andris C, Shimazaki H, Sakoe K, Nakano I, Takiyama Y (2008) Novel SACS mutations in a Belgian family with sacsin-related ataxia. J Neurol Sci 264:73–76
Pablo LE, García-Martín E, Gazulla J, Larrosa JM, Ferreras A, Santorelli FM, Benavente I, Vela A, Marín MA (2011) Retinal nerve fiber hypertrophy in ataxia of Charlevoix-Saguenay patients. Mol Vis 17:1871–1876
Parfitt DA, Michael GJ, Vermeulen EGM, Prodromou NV, Webb TR, Gallo JM, Cheetham ME, Nicoll WS, Blatch GL, Chapple JP (2010) The ataxia protein sacsin is a functional co-chaperone that protects against polyglutamine-expanded ataxin-1. Human Mol Genet 18:1556–1565
Peyronnard JM, Charron L, Barbeau A (1979) The neuropathy of Charlevoix-Saguenay ataxia: an electrophysiological and pathological study. Can J Neurol Sci 6:199–203
Schorge S, van de Leemput J, Singleton A, Houlden H, Hardy J (2010) Human ataxias: a genetic dissection of inositol triphosphate receptor (ITPR1)-dependent signalling. Trends Neurosci 33:211–219
Shimazaki H, Takiyama Y, Sakoe K, Ando Y, Nakano I (2005) A phenotype without spasticity in sacsin-related ataxia. Neurology 64:2129–2131
Shimazaki H, Sakoe K, Niijima K, Nakano I, Takiyama Y (2007) An unusual case of a spasticity-lacking phenotype with a novel SACS mutation. J Neurol Sci 255:87–89
Stanton M, Pannoni V, Lewis RA, Logigian EL, Naguib D, Shy ME, Cleland J, Herrmann DN (2006) Dispersion of compound muscle action potential in hereditary neuropathies and chronic inflammatory demyelinating polyneuropathy. MuscleNerve 34:417–422
Tankisi H, Pugdahl K, Johnsen B, Fuglsang-Fredericksen A (2007) Correlations of nerve conduction measures in axonal and demyelinating polyneuropathies. Clin Neurophysiol 118:2383–2392
Taoka T, Kin T, Nakagawa H, Hirano M, Sakamoto M, Wada T, Takayama K, Wuttikul C, Iwasaki S, Ueno S, Kichikawa K (2007) Diffusivity and diffusion anisotropy of cerebellar peduncles in cases of spinocerebellar degenerative disease. Neuroimage 37:387–393
Terracciano A, Casali C, Grieco GS, Orteschi D, Di Giandomenico S, Seminara L, Di Fabio R, Carrozzo R, Simonati A, Stevanin G, Zollino M, Santorelli FM (2009) An inherited large scale rearrangement in SACS associated with spastic ataxia and hearing loss. Neurogenetics 10:151–155
Vermeer S, Meijer RPP, Pijl BJ, Timmermans J, Cruysberg JRM, Bos MM, Schelhaas HJ, van de Warrenburg BP, Knoers NV, Scheffer H, Kremer B (2008) ARSACS in the Dutch population: a frequent cause of early-onset cerebellar ataxia. Neurogenetics 9:207–214
Vermeer S, Meijer RPP, Hofste TGJ, Bodmer D, Bosgoed EA, Cremers FP, Kremer BH, Knoers NV, Scheffer H (2009) Design and validation of a conformation sensitive capillary electrophoresis-based mutation scanning system and automated data analysis of the more than 15 kbp-spanning coding sequence of the SACS gene. J Mol Diagn 11:514–523
Vingolo EM, Di Fabio R, Salvatore S, Grieco G, Bertini E, Leuzzi V, Nesti C, Filla A, Tessa A, Pierelli F, Santorelli FM, Casali C (2011) Myelinated retinal fibers in autosomal recessive spastic ataxia of Charlevoix-Saguenay. Eur J Neurol 18:1187–1190
Yamamoto Y, Nakamori M, Konaka K, Nagano S, Shimazaki H, Takiyama Y, Sakoda S (2006) Sacsin-related ataxia caused by the novel nonsense mutation Arg4325X. J Neurol 253:1372–1373
Ying SH, Landman BA, Chowdhury S, Sinofsky AH, Gambini A, Mori S, Zee DS, Prince JL (2009) Orthogonal diffusion-weighted MRI measures distinguish region-specific degeneration in cerebellar ataxia subtypes. J Neurol 256:1939–1942
Acknowledgments
The authors wish to thank Drs. Jorge Artal, José Luis Capablo, Manuel Gracia-Naya and Pilar Larrodé for referral of patients; Dr. Elena García, for help with the ophthalmological part of this article, and Mr. Juan Luis Fuentes, for the ophthalmologic photographs. We also thank Ms. Stephanie Lyon, for linguistic assessment. This work is dedicated to the memory of Paloma Agüeras (1958–2009).This work was supported by grants of the Italian Ministry of Health (Ricerca Corrente, RC-FSM-02/2010) and of the European Union for EUROSPA (E-RARE grant IT0807), to FMS; and by a grant of the Centro de Investigación Biomédica en Red de Enfermedades Neurodegenerativas and Fondo de Investigaciones Sanitarias (PI07/132E to JB).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gazulla, J., Benavente, I., Vela, A.C. et al. New findings in the ataxia of Charlevoix–Saguenay. J Neurol 259, 869–878 (2012). https://doi.org/10.1007/s00415-011-6269-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-011-6269-5