Article Text

Abstract
Background and purpose Intra-arterial chemotherapy for retinoblastoma has been adopted as a first-line treatment option by numerous tertiary centers. The effect of intra-arterial chemotherapy on future rates of metastatic disease as well as on globe salvage in advanced eyes remains relatively unknown.
Methods A search of PubMED, MEDLINE, EMBASE, and Web of Science electronic databases was conducted from inception until January 2019 for studies with a minimum of 10 patients reporting outcomes and complications following intra-arterial chemotherapy for retinoblastoma.
Results A total of 20 studies met the inclusion criteria for analysis, comprising 873 patients and 1467 eyes. Only one study was comparative; there was substantial heterogeneity in reported outcomes and several overlapping patient cohorts that were published. Across all studies, 174 of 1467 eyes were enucleated (11.8%). Metastatic disease occurred in 8 of 513 patients (1.6%). Globe salvage was achieved in 318 of 906 (35.6%) cases of advanced retinoblastoma. The most common ocular complication was retinal detachment, occurring in 23% of eyes, and the most common systemic complications were transient fever and nausea/vomiting.
Conclusions There is a paucity of higher-level evidence with adequate follow-up surrounding the long-term safety of intra-arterial chemotherapy and effect on metastasis in retinoblastoma. Studies to date have been limited by short-term follow-up. Longitudinal prospective studies could provide greater insight into the ability of intra-arterial chemotherapy to reduce the risk of retinoblastoma metastasis.
- intervention
- guidewire
- orbit
Statistics from Altmetric.com
Introduction
Retinoblastoma (Rb) is the most common primary intraocular tumor in children and remains a devastating globe- and life-threatening disease, affecting up to 8000 patients across the world annually.1 Since the pioneering of ophthalmic artery chemosurgery, intra-arterial chemotherapy (IAC) has become first-line therapy for Rb at several tertiary ocular centers worldwide, with applications for both primary and salvage treatment, allowing salvage of advanced eyes that would have been previously enucleated.2 3 IAC importantly eschews several complications associated with systemic chemotherapy such as ototoxicity and neurotoxicity.4 Prior to the IAC era, nearly 80% of advanced (International Classification Retinoblastoma group (ICRB) group D and E) eyes went on to enucleation.5 Despite potential efficacy for globe salvage, the subsequent rate of metastatic disease in IAC-treated patients with Rb remains undetermined.
A previous systematic review in 2016 by Yousef and colleagues provided an extensive assessment of the evidence for IAC use in Rb.6 Since this study there have been several further series published.3 7–11 However, multiple reporting of the same patient cohorts and lack of higher-level comparative data make critical evaluation of complication and outcome rates difficult. Thus, the aim of the present study was to provide a collated updated summary of the safety and efficacy of IAC in Rb, with a focus on advanced disease.
Methods
Literature search strategy
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. PubMed, MEDLINE, EMBASE, and Web of Science electronic databases were searched from inception until January 2019 for English language studies. The following terms were combined to maximize the search strategy: intra-arterial, selective chemosurgery, retinoblastoma, intra-arterial therapy. The search strategy was optimized by a medical reference librarian with input from the authors.
Selection criteria
Inclusion criteria for eligible studies comprised all studies reporting at least one ocular outcome (rate of enucleation or globe salvage, metastatic disease, or intraocular recurrence) following IAC treatment for Rb. Studies reporting combined use of IAC with concurrent intravitreal therapy were included. Case reports, conference presentations, editorials, reviews, non-English studies, and studies with fewer than 10 patients were excluded, as well as studies only reporting use of intravitreal chemotherapy.
When institutions published duplicate studies with accumulating numbers of patients or increased lengths of follow-up, or when studies reported multiple time courses of the same treated cohort, only the most complete reports were included.
Independent screening of all available titles and abstracts was performed by two reviewers using the pre-defined inclusion and exclusion criteria (KR, WB). Full-text review of articles identified in screening was then performed by two reviewers (KR, WB), with application of inclusion criteria. Disagreement was resolved through inter-reviewer discussion.
Data extraction
All data were extracted from article texts, tables, and figures through use of a standardized form. Reviewers (KR and WB.) independently evaluated each included article with any discrepancy resolved by discussion to reach consensus. Information was collected on study characteristics, baseline demographics of study patients, grade of Rb, laterality, globe salvage and enucleation rates, complication rates, and technical success of delivery.
Bias assessment
Given the lack of comparative, studies, the Newcastle–Ottawa scale was not applicable for assessment of risk of bias. An alternative scale for single-arm series was not found.
Statistical analysis
Lack of comparative studies precluded the ability to perform a meta-analysis for efficacy measures such as either OR or relative risk. From each cohort, the cumulative incidence and 95% CI of globes undergoing subsequent enucleation following IAC was calculated, where reported. For ‘advanced’ eyes (defined as ICRB group D and E eyes) the cumulative incidence of globe salvage and 95% CI was also calculated. Event rates were then pooled in a meta-analysis of proportions across reporting studies using a random effects model. The heterogeneity of treatment effect across studies was evaluated using the I2 statistic, where I2 >50% suggests substantial heterogeneity. All statistical analyses were conducted using STATA 14 (STATA Corp, College Station, Texas, USA).
Results
Search strategy
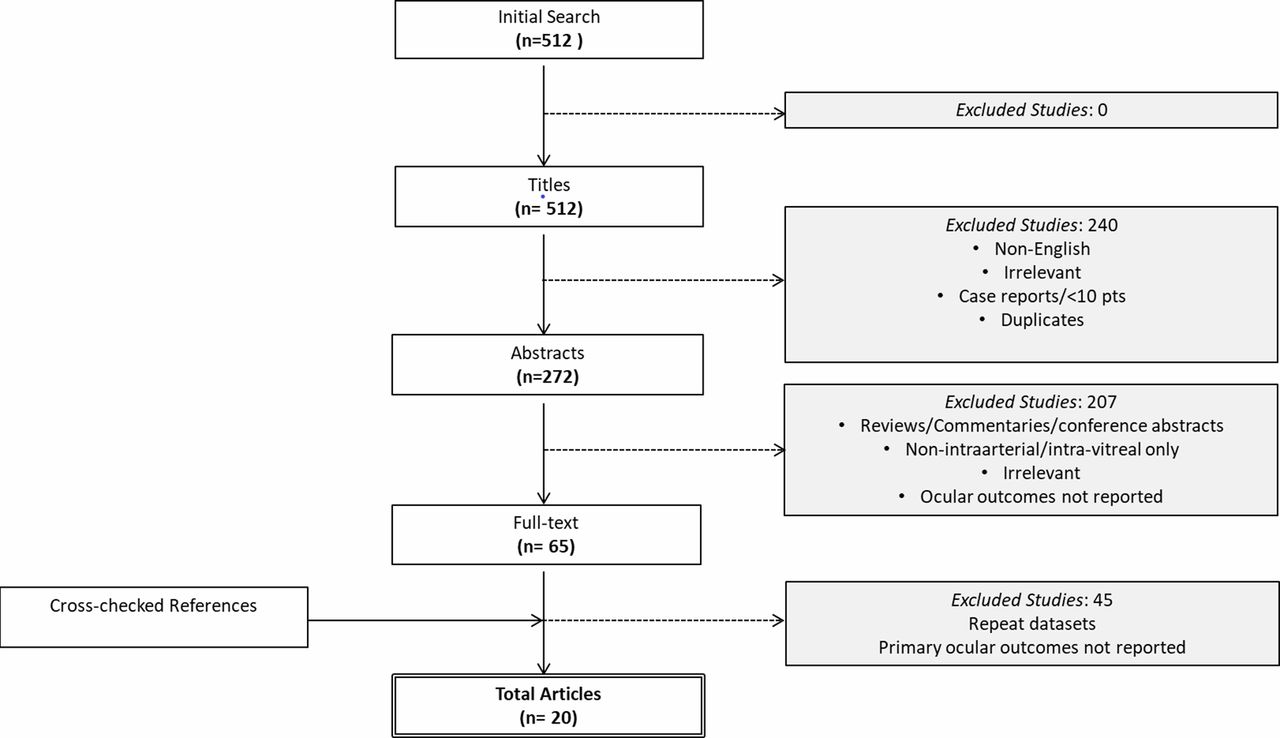
A total of 512 references were identified through all electronic database searches (figure 1). After exclusion of non-English, duplicate, or irrelevant references, 272 potentially relevant articles were assessed. Following comprehensive title and abstract screening, 65 articles remained for full-text evaluation. Twenty of these studies met the inclusion criteria, comprising 873 patients, 1467 eyes, and 2872 infusion procedures2–4 7–26 (study details provided in table 1). Median follow-up time was 24.1 months (range 8.7–79). Two studies were prospective while the remainder were retrospective, and the earliest study was published in 2011. All studies were single-arm retrospective series without a comparative group. The most commonly used chemotherapeutic regimens were two-drug regimens consisting of combined melphalan, carboplatin, or topotecan.

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram depicting literature search strategy.
Baseline study characteristics
Enucleation rate
Sixteen studies explicitly reported enucleation rates following IAC. Enucleation was performed in 174 eyes out of 543 (32%). After pooling single-arm studies, the overall effect sizes of the proportion of eyes undergoing enucleation was 0.29 (95% CI 0.19 to 0.39) as depicted via Forest plot (figure 2). Only one study (Hua et al, 2018) reported an enucleation rate above 50%.
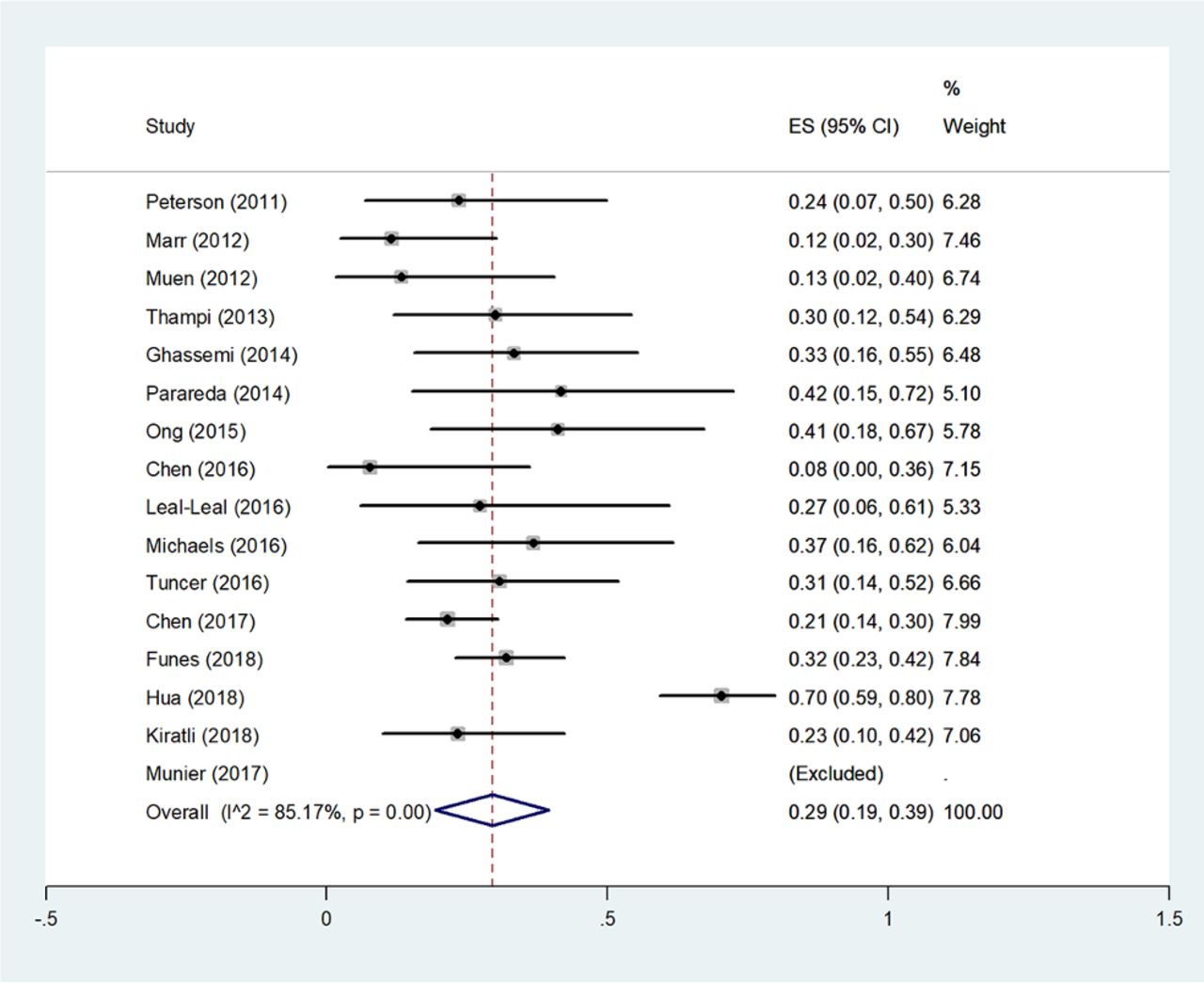
Forest plot depicting overall effect sizes of the proportion of eyes experiencing enucleation.
Rate of metastatic disease
Six studies reported rates of metastatic disease following IAC (table 2). Metastatic disease occurred in 8 of 513 patients (1.6%).
Globe salvage in advanced disease versus low-group eyes
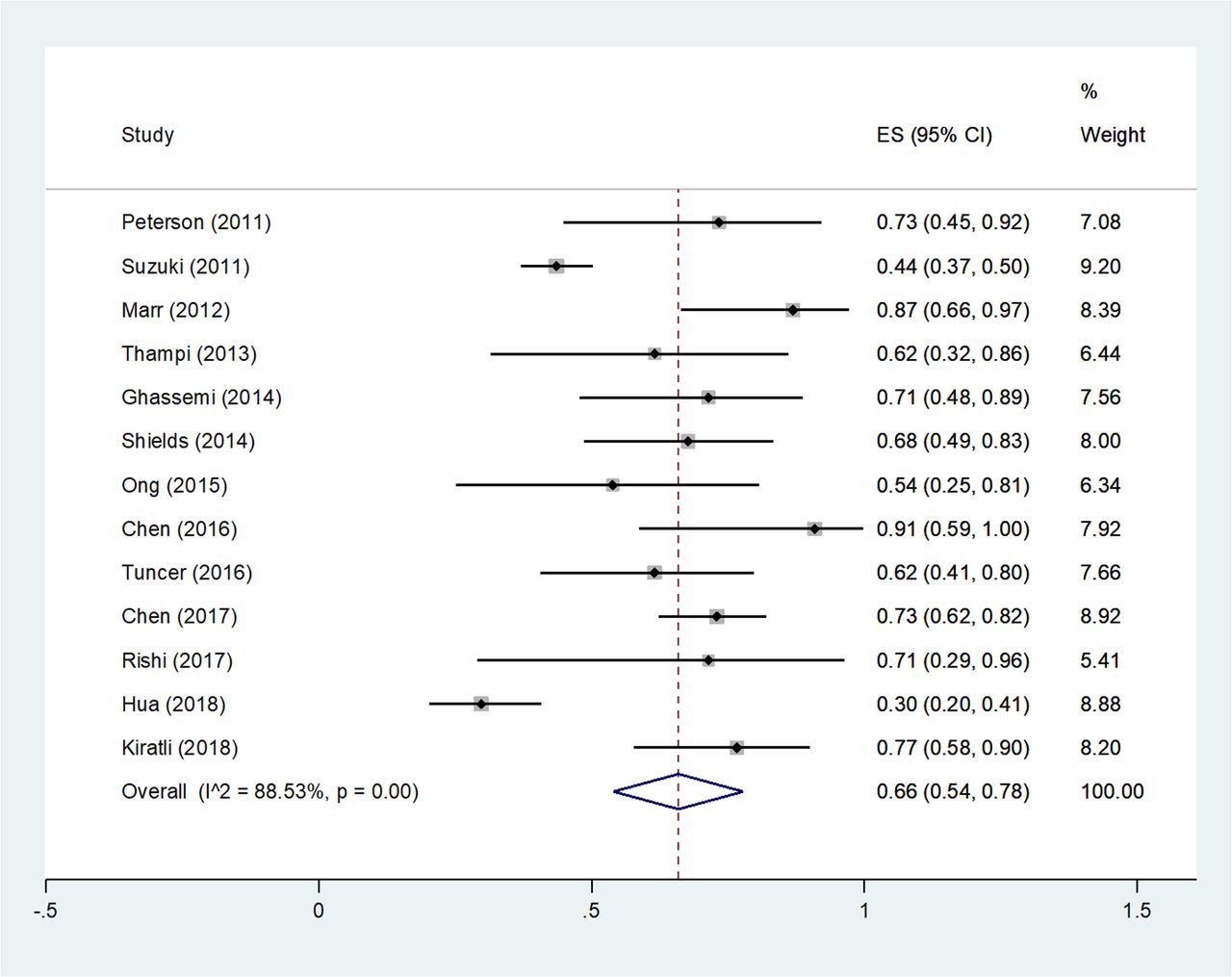
Thirteen studies (1220 eyes) reported globe salvage rates by ICRB group, comprising 314 group A–C eyes and 906 D–E eyes. The overall globe salvage rate was 46.7% (676/1446 eyes). Globe salvage was achieved in 199 (63.3%) group A–C eyes and 318 (35%) group D–E eyes. Following pooling, the overall effect size for the proportion of advanced eyes achieving globe salvage was 0.66 (95% CI 0.54 to 0.78; figure 3).
{kind=link}
{kind=link}
{kind=link}
Forest plot depicting overall effect size for proportion of eyes achieving globe salvage.
Ocular complications
Retinal or choroidal ischemia was reported in 38 of 289 eyes (13.1%), retinal detachment in 21 of 90 (23.3%), chorioretinal atrophy in 35 of 542 eyes (6.4%), vitreous hemorrhage in 50 of 421 (11.9%), periocular edema in 25 of 182 (13.7%), oculomotor nerve palsy in 8 of 32 (25%), and cataract in 6 of 25 (24%) (see online supplementary table 1).
Supplementary file 1
Cerebrovascular and systemic complications
Ophthalmic artery vasospasm was observed intra-procedurally in 29 of 363 cases (8.0%). Neutropenia occurred in 38 of 230 cases (16.5%), nausea and vomiting in 63 of 541 patients (11.6%), bronchospasm in 10 of 122 patients (8.2%), and fever in 35 of 216 (16.2%) (see online supplementary table 1).
Discussion
This meta-analysis of 20 studies assessing outcomes and complications following IAC for Rb highlights the safety and efficacy of this technique and its ongoing potential role in the treatment of advanced Rb. The results of this study demonstrate improved enucleation rates following IAC for Rb, with 35% globe salvage in advanced eyes. Overall, the rate of systemic complications was low, although vascular ischemia, retinal detachment, and vitreous hemorrhage are prevalent secondary effects, ranging from 13% to 23%.
Yousef and colleagues previously provided a comprehensive review of IAC for Rb.6 In their pooled analysis, globe salvage was achieved across 66% of eyes, with a 2.1% metastatic rate. However, as similarly highlighted in this study, there was substantial heterogeneity in reporting of outcomes with not all studies explicitly specifying globe salvage rates. Lack of sufficient follow-up further resulted in few studies reporting metastatic disease rates. Grading of Rb disease advancement was not standard and further limited potential analyses stratifying outcomes by Rb group. Here we have attempted to collate reported metastatic rates (where available) and provide stratified subanalysis of outcomes in advanced eyes (Group D–E) and non-advanced eyes (A–C). Their study underscores the relatively low quality of studies assessing the role for IAC in Rb. Moreover, an additional 12 studies have been published since Yousef and colleagues’ review that were eligible for inclusion in this analysis.
Most commonly used techniques include a transfemoral approach using a 4F pediatric guide catheter, and then superselective ophthalmic artery catheterization just proximal to the ostium with a microcatheter.2 The microcatheter is most commonly not allowed to enter the ophthalmic artery in order to avoid wedging of blood flow into the artery and intimal trauma during chemotherapy injection.27 In the included studies, technical success of delivery was high, ranging from 90% to 100% (table 1). Advances in neurovascular microcatheter delivery systems and increasing wealth of experience could additionally explain the tendency towards near complete technical success with IAC estimated in this analysis.
In the review by Yousef and co-authors the globe salvage rate in Intraocular Retinoblastoma Classification (IIRC) D–E eyes was 57% from 456 eyes and overall globe salvage was achieved in 66% of eyes. In contrast, our results suggest that, in advanced eyes, the globe salvage rate may not be as high as previously believed (35% in this study). The decision to undertake IAC in these patients must thus be made on an individual patient basis, with careful weighing of risk-benefit. In the study by Yousef and colleagues it was not clear how many of these eyes required adjunctive treatment such as external beam radiation to prevent enucleation, however. Arguably often understated in the decision-making process is parent refusal for enucleation due to cosmesis and visual loss, despite significantly advanced eye disease. We therefore aimed to focus on metastatic rates as well as globe salvage rates, in contrast to the 2016 stuudy by Yousef et al in which included studies were insufficiently granular to extract rates of metastasis. As observed from this analysis, the majority of studies focused solely on globe salvage and prevention of enucleation but failed to report rates of subsequent metastasis. The utility of globe salvage, particularly in advanced eyes, is questionable if there is a substantial risk of metastatic involvement.6 In these cases, enucleation could perhaps be a more prudent strategy. For group E eyes, in particular, there was a large degree of variability of globe salvage rates ranging from 30% to 100%.2 4 13 Our analysis furthermore highlights that evidence for IAC in Rb has improved since Yousef and colleagues’ review, although it remains restricted to retrospective cohort studies. Nonetheless, our results reinforce the safety of IAC for Rb, together with the results of Yousef et al. Despite these fluctuations, as evidenced from the Forest plot, the rate of globe salvage has not increased substantially since 2011. In a recent meta-analysis comparing intravenous chemotherapy (IVC) with IAC, IAC resulted in higher globe salvage rates in ICRB group D eyes, but not in groups B, C, or E compared with IVC.28
IAC has been associated with several ocular and systemic complications, as well as potential cerebrovascular complications from procedure-related morbidity. The most common ocular complications were retinal detachment, choroidal or retinal ischemia, vitreous hemorrhage, and chorioretinal atrophy. Retinal detachment occurred in nearly a quarter of treated eyes and could represent an under-recognized phenomenon in patients with Rb treated with IAC. Retinal detachment and vitreous haemorrhage represent transitory less clinically significant complications that are typically self-limiting with conservative management. Ischemic events, on the other hand, represent a greater source of morbidity as potentially permanent vision-threatening complications of IAC treatment. Ophthalmic artery vasospasm was the most commonly reported cerebrovascular complication, occurring intraoperatively in 8% of cases. In one series ophthalmic artery obstruction during delivery was reported in 2% of patients, but the management and subsequent outcomes were not specified by the author.2 In the vast majority of these cases, vasospasm was transient and self-limiting. In contrasting, the incidence of retinal ischemia has diminished following super-selective catheter placement at the ostium of the ophthalmic artery, as opposed to more distal placement within the vessel itself. The most common systemic complications were neutropenia and fever. No requirement for transfusion was reported by any of the studies also reporting rates of neutropenia. Few studies specified neutropenia grade. Bronchospasm requiring bronchodilator therapy also occurred in nearly 10% of cases.
Uncertainty persists surrounding the metastatic rate of IAC-treated Rb. As demonstrated by this analysis, there is a paucity of evidence—owing to lack of studies with sufficiently long-term follow-up—assessing the risk of metastasis, particularly in advanced grade eyes. In their recent 10-year experience with IAC at the Memorial-Sloan Kettering Cancer Center, Francis and colleagues reported 88% progression-free survival at 1 year.8 The incidence of orbital versus systemic metastases and rates of pineoblastoma in hereditary Rb patients were unfortunately not specified by the included studies. Importantly, in comparison with systemic chemotherapy, IAC has minimal ability to prevent systemic metastases or pinealoblastoma occurrence due to negligible systemic absorption.27 Both this study and the study by Yousef et al have estimated metastatic rates to be in the order of 1.5–2.5%,6 but this is likely to be an underestimation given that a higher rate of advanced eyes with greater metastatic potential go on to be enucleated. Moreover, long-term IAC experience was limited to a handful of high-volume ‘centers of excellence’.8 Similar to other technical procedures reliant on operator experience and quality of peri-/postoperative care, the success rate of IAC in treating Rb at smaller centers could be lower and incur increased morbidity.
Limitations of study
Unfortunately, the ability to perform more detailed analysis was limited by lack of granularity in published study data. All included studies were non-comparative except for one, and therefore precluded the ability to perform a pairwise meta-analysis comparing IAC with alternative therapy. Additionally, the presence of repeated published datasets with heterogenous outcomes and complications across cohorts made coherent analysis of complications difficult. Few studies explicitly detailed ocular, cerebrovascular, and systemic complications. The ability to draw meaningful conclusions regarding the safety and long-term efficacy thus arguably remains limited in light of a relatively poor evidence base from which to draw. Only seven studies explicitly reported outcomes using the ICRB scale for advanced eyes. The high number of duplicated series additionally inflates the evidence base for IAC therapy.6 When removing duplicative publications, the literature remains composed of single-institution case series. Nonetheless, this study provides pooled event rates for systemic and ocular complications that can potentially be used to guide intervention. In order to improve the ability to make meaningful inferences, future studies may be well-suited by explicitly reporting Rb group by classification. Individual patient-level data for smaller cohorts in particular may serve to minimize the heterogeneity that was encountered in this study and provide more optimal information for meta-analysis.
Conclusions
IAC is a safe and efficacious treatment option for Rb. The evidence surrounding the use of IAC for Rb remains low level and heterogeneous. There was a paucity of literature pertaining to the incidence of orbital metastases and pineoblastoma. IAC can prevent the need for immediate enucleation, but its effect on long-term metastatic disease remains unclear.
Outcomes
References
Footnotes
Contributors KR and WB designed study, performed the literature search, selected studies for inclusion in the meta-analysis, abstracted data, performed statistical analysis, and drafted and revised the manuscript. LAD and JSP revised and drafted the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.