Article Text

Summary
Angle closure glaucoma, both acute and chronic, is a major cause of blindness worldwide. Transscleral cyclophotocoagulation (TSCP) is conventionally undertaken non-urgently in patients with advanced glaucoma and poor visual potential with poor control of intraocular pressure (IOP). We describe a case of a patient with refractory acute angle closure glaucoma and severe pain in whom emergency TSCP was undertaken 12 h after presentation, reducing the IOP from 68 to 10 mm Hg. Further, a patient with chronic angle closure glaucoma underwent TSCP, reducing the IOP from 78 to 14 mm Hg. Both patients consequently underwent uneventful phacoemulsification cataract surgery with preservation of visual acuity and long-term IOP control. TSCP may achieve prompt IOP control and symptomatic relief in the acute setting in patients with acute and chronic forms of angle closure glaucoma refractory to medical therapy. TSCP may reduce the risk of definitive surgical intervention by temporising phacoemulsification or trabeculectomy surgery until the IOP is well controlled.
Statistics from Altmetric.com
Background
Transscleral cyclophotocoagulation (TSCP)—or cyclodiode laser—is a technique used to ablate the ciliary body using a diode laser directed through the sclera of a closed globe in patients with intractable glaucoma refractory to medical and/or surgical therapies. TSCP is cyclodestructive, and therefore it is conventionally indicated in the control of high intraocular pressure (IOP) in patients with poor visual potential, such as neovascular glaucoma.1 Increasing experience with TSCP is expanding the range of indications to patients with excellent visual potential, and with earlier roles in the management of patients with several forms of glaucoma.2 ,3
We present our experience with two patients with acute (AACG) and acute-on-chronic angle closure glaucoma who underwent emergency TSCP to achieve acute IOP control, following which definitive interventions could be safely undertaken.
Case presentation
Case 1
A 40-year-old man presented with a 12 h history of right ocular pain, redness, visual loss, nausea and vomiting with onset 6 h after pupillary dilation following a consultation for consideration of cataract surgery. There was no ocular history or ocular trauma. On examination, the right visual acuity was perception of light. The right eye was injected with a fixed, mid-dilated pupil and generalised corneal oedema. The right anterior chamber was shallow with a peripheral iridocorneal touch peripherally. The left anterior chamber was of moderate depth. His IOPs measured 78 and 18 mm Hg on the right and the left eyes, respectively. Gonioscopy revealed 360° of angle closure in his right eye, not responding to indentation. His left drainage angle was wide open through 360°. There was an intumescent white cataract present on the right eye; the fundus was not visible.
The patient was admitted and received treatment with topical aproclonidine 1%, bimatoprost 0.03%, timolol 0.25%, dorzolamide 2% and pilocarpine 2% to the right eye. Acetazolamide 500 mg was administered both orally and intravenously. Two hours later, the right IOP was measured at 68 mm Hg. Despite an intravenous infusion of mannitol, and a repeated intravenous infusion of acetazolamide, the right IOP remained elevated at 65 mm Hg. The patient was in excruciating pain with intractable nausea, not responding to oral analgesia and systemic anti-emetics. Severe corneal oedema prevented YAG iridotomy or argon laser iridoplasty. Anterior chamber paracentesis was not considered safe due to a very shallow anterior chamber and intumescent cataract. Therefore, the patient underwent emergency 360° TSCP (G-probe, Iris Medical Instruments, Mountain View, California, USA; 20 shots×1450–1510 mW×2 s) under Sub-Tenon's anaesthetic 12 h after presentation. The 3 and 9 o'clock positions were spared to avoid the long ciliary nerves. The pulse energy was titrated, reducing the power below the threshold at which an audible pop could be heard.
The right ocular pain and nausea had subsided by the following morning; his right IOP was recorded as 10 mm Hg. Systemic acetazolamide was discontinued. Rapid resolution of corneal oedema enabled right YAG peripheral iridotomy, which was undertaken later that day (figure 1A). Two days later, the patient underwent right phacoemulsification cataract surgery with intraocular lens implantation. A prior core vitrectomy was performed to deepen the anterior chamber.
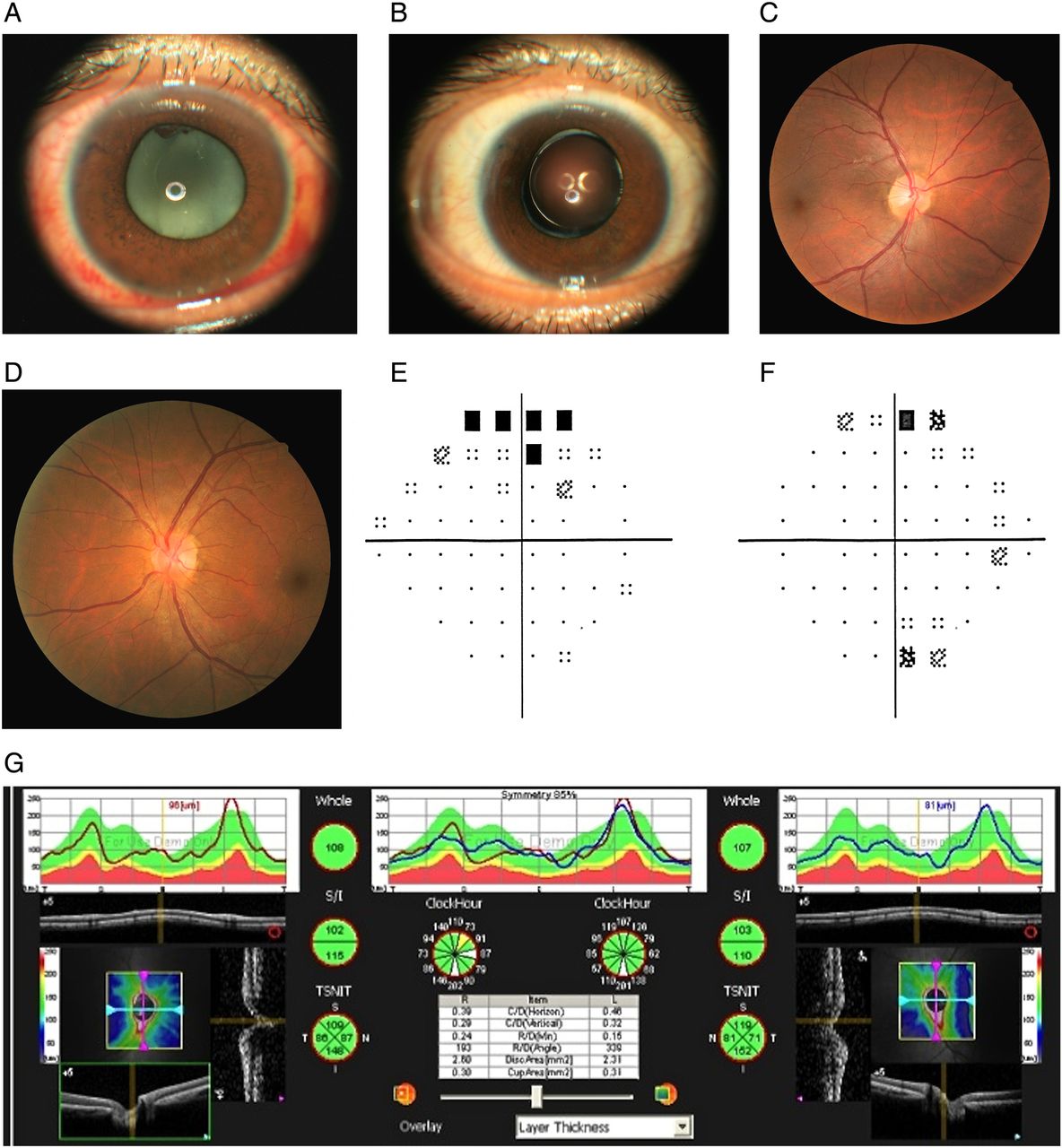
Clinical images of a patient presenting with acute angle closure glaucoma. (A) Anterior segment photograph of a patient in case 1 immediately prior to right phacoemulsification cataract surgery. The white intumescent cataract is demonstrable, with a clear cornea following Transscleral cyclophotocoagulation 3 days previously, and a peripheral iridotomy is visible superotemporally. The pupil is tonically dilated following acute angle closure glaucoma and an inflammatory iris debris is visible superiorly. (B) Postoperative appearance demonstrating a centred intraocular lens and clear ocular media. Optic disc photograph of the right eye (C) and left eye (D) demonstrating a healthy but asymmetrical neuroretinal rim with a subtle right temporal disc pallor. The maculae appear within normal limits. Automated visual field analysis (pattern SDs are presented) 24–2 reveals a right superior arcuate scotoma (E) and grossly full visual field in the left eye (F). Reliability indices for automated visual field results are: <5% false-positive and false-negative errors, with fewer than 10% fixation losses. Retinal nerve fibre layer analysis reveals symmetrical optic disc parameters between the right and left eyes excluding glaucomatous optic neuropathy (G).
At the postoperative review, his visual acuity was 6/6 OU with IOP 13 mm Hg without topical antihypertensives (figure 1B). Peripheral iridotomies were patent with one quadrant of peripheral anterior synechiae, and trabecular meshwork identifiable in the remainder of the drainage angle OD. Optic disc appearance revealed a healthy neuroretinal rim and absence of glaucomatous optic neuropathy, although subtle temporal optic disc pallor was present (figure 1C, D). Automated visual field analysis demonstrated a mild right superior arcuate field defect with generalised depression in field (figure 1E). The left visual field was full (figure 1F). Optic nerve head analysis identified a symmetrical profile, excluding a significant loss of retinal ganglion cells in the right eye (figure 1G).
Case 2
A 70-year-old woman was referred from a primary care eye service to eye casualty with bilateral visual field defects, optic disc changes and an IOP of 78 mm Hg in both eyes. She reported haloes around lights but had no other symptoms. There was no ocular history of note. Her refraction was −0.50 DS OD, +0.25 DS OS. On examination, visual acuities were 6/24 in both eyes, improving to 6/9 with pinhole on the left eye only. The conjunctiva was white, the cornea was clear and the anterior chamber was quiet bilaterally. IOP was measured at 78 mm Hg OD and 80 mm Hg OS. Gonioscopy identified Schwalbe's line only bilaterally. Fundal examination revealed deeply cupped optic discs bilaterally (figure 2A, B). This presentation suggested a chronic rather than an acute onset of raised IOP.

{kind=link}
{kind=link}
Clinical images of a patient presenting with chronic angle closure glaucoma. Optic disc photographs demonstrating advanced glaucomatous optic neuropathy, right (A) worse than left (B), with an inferior neuroretinal rim thinning more prominently than superior thinning. (C) Automated visual field analysis (10–2: pattern SDs are presented) of the right eye demonstrating advanced visual field constriction but relative sparing of the central 3°. (D) The 24–2 automated field analysis of the left eye demonstrating a superior arcuate scotoma with an inferior nasal step in keeping with optic disc appearance. Reliability indices for automated visual field results are: <5% false-positive and false-negative errors, with fewer than 10% fixation losses.
Conventional medical therapy was started immediately and IOP fell to 22 mm Hg OD and 23 mm Hg OS. Bilateral YAG iridotomies were performed. Dorzolamide 2% two times a day, timolol 0.5% two times a day and aproclonidine 1% three times a day were continued in both eyes together with intensive topical steroids.
One week later, IOP had risen to 31 mm Hg OD, 30 mm Hg OS. The iridotomies appeared patent. Topical steroids were tapered and bimatoprost drops added to both eyes. Over the next few weeks, IOP fell slightly, medication was reviewed and the need for either a trabeculectomy or cataract operation was discussed with the patient. The angle was thought to be very narrow but no peripheral anterior synechiae (PAS) were present. Three months following the initial presentation, IOP became markedly elevated once again, 78 mm Hg OD and 30 mm Hg OS. The angle appeared closed, and could not be opened with indentation. Conventional treatment including intravenous mannitol was started with a view to undertake urgent cataract surgery. Although the right peripheral iridotomy (PI) was thought to be patent, a further laser PI was performed. The pressure remained elevated at 56 mm Hg, however. A TSCP laser was performed (Iris Medical, 22 shots, 2 s duration 1500–2000 mW over 360° avoiding the 3 and 9 o'clock positions to avoid the long ciliary nerves and reduce postoperative pain).
The next day, the pressure fell to 30 mm Hg in the right eye. One week later, it was 18 mm Hg OD and 22 mm Hg OS, and the anterior chamber was noted to be significantly inflamed despite topical steroid treatment. Significant PAS were noted in the right eye, whereas the left angle was open but narrow. First the right eye and then the left eye cataract surgery were subsequently performed. Postoperatively, IOP remained in the 20s and a left trabeculectomy augmented with mitomycin C was undertaken, followed by right trabeculectomy with mitomycin C. At the last follow-up, some 4 years after presentation, the visual acuity was recorded as 6/9 OD, 6/4 OS; IOP 14 mm Hg OD, 10 mm Hg OS on latanoprost to the right eye. The fields have remained stable, although with severe loss in the right eye (figure 2C, D).
Discussion
AACG is a leading cause of blindness worldwide,4 ,5 and is a sight-threatening ophthalmic emergency. Lens induced acute secondary angle closure glaucoma (ACG) can be precipitated by an intumescent cataract and following pupillary dilation, as in case 1. Equatorial growth of the crystalline lens slackens the suspensory ligament of the lens allowing forward movement of the lens resulting in iridocorneal contact, iris bombe and pupillary block. The majority of patients with AACG respond to topical antihypertensive agents, reducing corneal oedema to permit definitive YAG laser iridotomy, breaking the underlying mechanism of pupil block. Sequential lensectomy with or without trabeculectomy may then be undertaken if indicated. A minority of patients with AACG do not respond to topical and systemic antihypertensive agents.3 ,6 Corneal oedema may prevent laser intervention (argon iridoplasty or YAG iridotomy) even if the cornea can be temporarily cleared, and a shallow anterior chamber risks injury to the lens capsule if paracentesis is attempted. Emergency phacoemulsification or trabeculectomy surgery in AACG is challenging,7 with a poor intraoperative view conferring increased risk of operative complications (such as corneal endothelial damage/posterior capsular rupture, etc) and sudden ocular decompression from a high starting IOP risking suprachoroidal haemorrhage and permanent visual loss.7 Moreover, uncontrolled IOP at the time of trabeculectomy surgery in patients with AACG is associated with an increased risk of failure (approximately 35%).7
Cyclodestructive strategies aim to ablate the ciliary body, reducing the production of aqueous humour, and consequently reduce IOP. Treatment modalities include open globe procedures such as endoscopic cyclophotocoagulation, or closed globe procedures such as TSCP (diode laser) or cryotherapy.8 Endoscopic cyclophotocoagulation has been developed to selectively ablate the ciliary body under direct visualisation, often performed in combination with cataract extraction.9
TSCP has recently been described as a safe and effective management strategy in AACG refractory to medical therapies to achieve IOP control.3 ,6 One series identified five patients with refractory AACG who underwent non-urgent TSCP between 2 and 23 days of presentation with all patients maintaining 6/12 vision or better following delayed, sequential lensectomy. All five patients had an IOP of 17 mm Hg or lower; only one patient remained on topical antihypertensive agents.3 No intraoperative complications were reported during delayed lensectomy after IOP control had been instituted.3 A Chinese patient cohort with AACG who underwent TSCP followed by combined phacotrabeculectomy identified slightly poorer IOP control, although laser iridotomy and/or iridoplasty had not been undertaken prior to TSCP in this series.6
Our patient with AACG underwent immediate TSCP, 12 h after presentation, after treatment failure on topical and systemic hypertensive agents. To the best of our knowledge, this is the earliest TSCP attempted in this setting. The successful outcome in this case may be related to the urgency with which TSCP was undertaken—out of hours under Sub-Tenon's block to avoid any anaesthetic-related delays—which risks progressive and swift glaucomatous optic atrophy and a poorer visual outcome. Clinical assessment and retinal nerve fibre layer imaging did not detect evidence of glaucoma in this patient, although an early superior visual field deficit was identified. Emergency TSCP also helped to relieve excessive pain and intractable nausea experienced by the reported patient, which had abated by the following morning. The severity of his symptoms suggested that 360° TSCP was appropriate, although given his excellent visual prognosis only 20 pulses were administered. It may be an acceptable strategy to consider sectoral TSCP initially and determine the clinical response. The treatment approach will vary according to symptoms, IOP, ocular comorbidities and visual potential in each individual patient. His visual acuity at discharge was 6/6 in the affected eye and IOP 13 mm Hg without topical agents.
Ophthalmologists caring for patients with refractory AACG must consider emergency TSCP to achieve prompt IOP control and as an effective analgesic strategy when medical treatment fails and laser therapy cannot be undertaken. A prospective randomised trial comparing long-term outcomes in patients with AACG undergoing primary TSCP versus acute phacoemulsification or trabeculectomy surgery is required. It is highly likely that protracted periods of excessively high IOP will result in severe structural and functional changes, reversible if a physiological IOP is quickly restored.10
TSCP has been evaluated in the setting of chronic ACG (CACG) refractory to medical management, predominantly in cohort studies from Asia where angle closure is prevalent.11 ,12 Chronic or subacute onset angle closure may not produce significant corneal oedema and it is likely that laser peripheral iridotomy will be undertaken. However, this intervention alone may not achieve IOP control, particularly in East Asian eyes.6 ,12 Intraocular procedures such as lensectomy and trabeculectomy may be similarly undesirable in the setting of uncontrolled IOP.7
TSCP is a valuable treatment option in patients with uncontrolled CACG. A case series of 13 patients undergoing TSCP for CACG identified it as a safe and effective management strategy, with 12 patients maintaining an IOP below 21 mm Hg without medications11 without any reported complications at 2-year follow-up. However, the treatment effect was noted to reduce after 24 months in this series, and retreatment may be required. Female gender and age over 50 have been identified as significant factors predicting response to TSCP. The IOP response rate in patients with CACG is high,12 particularly when compared to the response in patients with neovascular, traumatic and uveitic glaucoma. Some caution must be noted when comparing studies and racial groups where ACG is prevalent; the number of laser applications and laser energy used varies between studies, as do the end points defining success. Asian eyes may not respond in an equivalent manner to lighter coloured eyes, and the postoperative inflammatory reaction following TSCP may vary; this may further hamper cross-comparison of data.
TSCP is not without risk. It has been associated with postoperative iritis, hypotony, scleral thinning or perforation,13 necrotising scleritis,14 corneal oedema, conjunctival burns, pain or raised IOP. Increasing experience worldwide with TSCP has optimised laser settings to reduce the incidence of adverse outcomes, with numerous series reporting lack of complications.11 However, a series of patients with nanophthalmic angle closure all suffered choroidal detachment following TSCP.15 Micropulse TSCP has been developed with one series of 40 patients suggesting an 80% success rate of IOP control with or without medications with no loss of visual acuity at 18 months or hypotony.16 Variations in the mode and amplitude of TSCP delivery and increasing reports of safety are likely to augment confidence in the procedure in adult and paediatric populations. Furthermore, TSCP is likely to emerge as the primary treatment option in patients with good visual potential, in whom topical treatments are insufficient and open globe surgical procedures are not desired.
This case series illustrates the value of early TSCP in the management of patients with good visual potential with intractable AACG and CACG. In AACG, TSCP permitted acute control of IOP and relief of severe ocular pain and intractable nausea and vomiting, a benefit of TSCP not emphasised in other reported cases. In CACG, TSCP permitted safe and uneventful phacoemulsification and trabeculectomy surgery, with reduction in the requirement for long-term topical antihypertensive agents. We suggest that ophthalmologists consider primary TSCP prior to surgical intervention in patients with refractory AACG and CACG in whom YAG laser treatment cannot be undertaken, and where high IOP prevents safe operative intervention.
Learning points
Angle closure glaucoma—both acute and chronic—is one of the leading causes of blindness worldwide.
Transscleral cyclophotocoagulation appears to be a safe and effective management strategy in angle closure glaucoma refractory to medical therapies to achieve intraocular pressure (IOP) control.
Ophthalmologists should consider primary transscleral cyclophotocoagulation in patients with refractory acute or chronic angle closure glaucoma in whom YAG laser treatment cannot be undertaken, and where high IOP prevents safe operative intervention.
References
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.