Article Text

Summary
A 3-year-old child sustained severe ocular surface burns in her left eye after accidental lime injury. Despite appropriate management in the acute stage, she developed limbal stem cell deficiency (LSCD) in that eye. This was initially treated with autologous ex vivo cultivated limbal epithelial transplantation (CLET), which unfortunately failed after 6 months resulting in recurrence of LSCD. One year following CLET, she underwent simple limbal epithelial transplantation (SLET) using autologous donor tissue from the healthy fellow eye. Successful restoration of the ocular surface following SLET combined with amblyopia therapy led to significant cosmetic and functional improvement. One year following SLET her vision in the left eye was 20/80 and she continues to maintain a stable, avascular and completely epithelised corneal surface. This case illustrates that SLET is effective in treating LSCD even in cases that are conventionally considered to be at high risk for failure of limbal stem cell transplantation.
Statistics from Altmetric.com
Background
Simple limbal epithelial transplantation (SLET) is a novel surgical technique of limbal stem cell transplantation (LSCT), which obviates the need for laboratory processing and utilises minimal donor tissue. Thus, SLET is an alternative technique of LSCT that is affordable, easily replicable and safer for the donor eye.1 Previous studies have demonstrated that among patients with limbal stem cell deficiency (LSCD), children2 ,3 and those with multiple prior ocular surface procedures3 ,4 are unlikely to benefit from LSCT. In contrast to conventional expectations, this case demonstrates the efficacy of SLET in successfully treating a case at high risk of failure of LSCT.
Case presentation
A 3-year-old girl sustained accidental chemical injury to her left eye while playing with a packet of edible lime or ‘chuna’ in February 2010. Ocular examination under general anaesthesia confirmed that the right eye was unaffected. In the left eye, residual lime particles were observed in the upper and lower fornices, the cornea and limbus were almost completely de-epithelised with considerable corneal stromal haze and there were large epithelial defects on the bulbar conjunctiva both superior and inferiorly (figure 1A). Although the view was hazy in the left eye, the posterior pole could be visualised and appeared normal. Debridement of the residual ocular lime was performed and amniotic membrane graft was placed on the ocular surface to cover the corneal and conjunctival epithelial defect. She was prescribed tapering doses of topical prednisolone acetate 1% eye drops and seen again after 4 weeks. At this visit in May 2010, her visual acuity was counting fingers (CF) at half metres in the left eye. A clinical impression of LSCD was made based on ocular examination, which revealed symblepharon formation with forniceal shortening and conjunctivalisation of the corneal surface (figure 1B).

{kind=link}
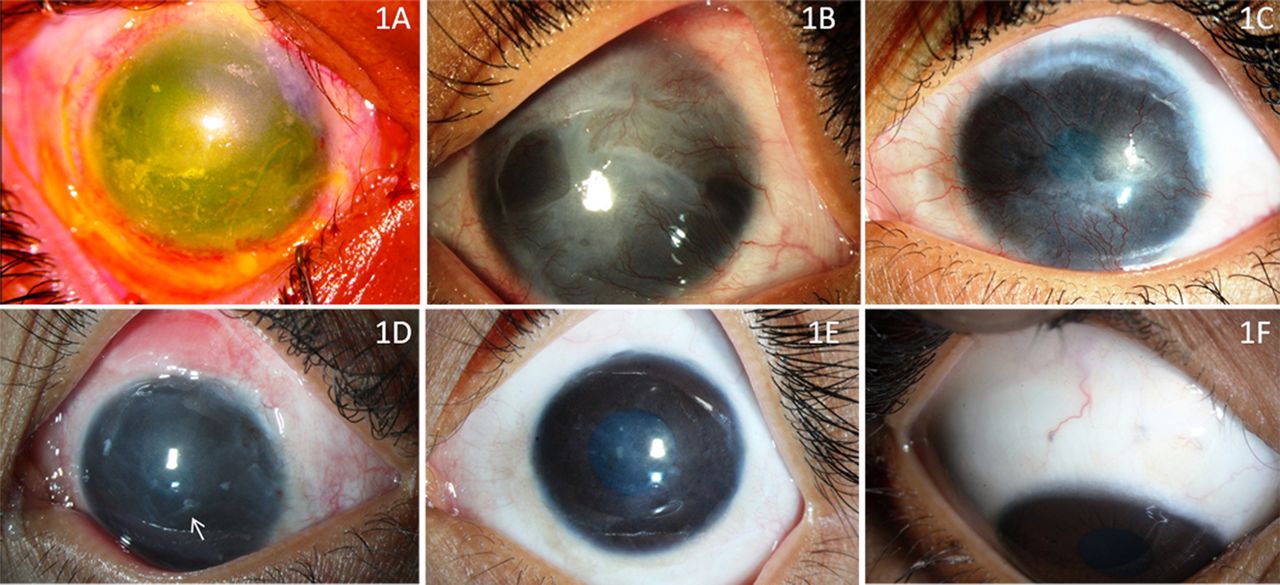
(A) Clinical photograph of the left eye showing extensive corneal limbal and conjunctival epithelial defect with corneal stromal haze, 3 days following lime injury. (B) Same eye 6 months after amniotic membrane grafting, showing conjunctivalised ocular surface, suggestive of limbal stem cell deficiency (LSCD). (C) Same eye 1 year after autologous cultivated limbal epithelial transplantation (CLET), showing a vascular and conjunctivalised ocular surface suggestive of recurrence of LSCD following CLET. (D) Postoperative photograph of the left eye 3 weeks after autologous simple limbal epithelial transplantation (SLET), showing an epithelised corneal surface with few limbal transplants in place (arrow). (E) One year post-SLET the left eye shows a stable, epithelised and avascular corneal surface with significant improvement in corneal clarity. The corrected visual acuity at this stage was 20/80. (F) Right eye showing healthy donor sites with no ocular surface deficits.
As the child carried a significant risk of developing severe amblyopia in her left eye, a decision to intervene surgically was made in October 2010. A limbal biopsy was taken from the unaffected eye; the limbal epithelium was cultured on a human amniotic membrane (hAM) substrate in the laboratory for 2 weeks; and a monolayer of expanded limbal epithelial cells along with the hAM graft were transplanted onto the ocular surface of the left eye after removing the pathological pannus. Postoperatively, she received prednisolone acetate 1% eye drops in tapering doses. Despite initial recovery the ocular surface progressively deteriorated over the course of the next year with recurrence of LSCD. In December 2011, 22 months following the initial injury and 14 months after autologous cultivated limbal epithelial transplantation (CLET) her vision was still CF at half metres with conjunctivalisation of the corneal surface (figure 1C).
Treatment
Although, in children, severe initial injury requiring hAM grafting and previously failed LSCT are all known high-risk factors for failure of subsequent limbal transplantation procedures, we decided to make another attempt to salvage vision in this child's left eye. Only this time round we performed SLET instead of CLET, because of the favourable experience we have had with this new technique in adults with similar injuries. In February 2012, a tiny 2 mm limbal biopsy was obtained from her right eye; at the same sitting the pannus covering the left eye was excised and a hAM graft was placed on the bared ocular surface with fibrin glue; the biopsied tissue was cut into small pieces and fixed on the hAM over the cornea with fibrin glue.
Outcome and follow-up
Postoperatively, topical prednisolone acetate 1% eye drops in tapering doses over 6 weeks along with antibiotic drops for 1week were prescribed. Her parents were advised to patch her right eye 3 h a day for treatment of amblyopia. At the 1 month postoperative visit, her visual acuity had improved to CF at 2 m. Central corneal clarity had improved and the surface was completely epithelised (figure 1D).
At 6 months postoperatively, her unaided visual acuity was 20/200 in the left eye. The corneal surface was completely epithelised, stable and avascular. 13 months after SLET in March 2013, visual acuity in her left eye was improving to 20/80 (−4.25 D sph with −1.75 D cyl×180°). Intraocular pressure in right and left eye was 18 and 14 mm Hg respectively. The cornea continued to maintain a stable, avascular and epithelised surface (figure 1E). On examination of the right eye both donor sites were healthy without conjunctivalisation (figure 1F). The fundus was normal in both eyes. She was advised to continue right eye patching with full refractive correction in the left eye.
Discussion
Although CLET has become popular in the treatment of LSCD especially in eyes with ocular burns, the outcomes of CLET in children have been suboptimal.2 ,3 The success rate of CLET (including both primary and repeat surgery) in curing LSCD is 46.7% in children2 as compared with 90.14% in adults.4 ,5 In addition, this particular case had other high-risk factors of failure of LSCT in the form of two prior failed ocular surface procedures (hAM grafting and CLET).3–5 Conventional wisdom would have been in favour of refraining from further surgical interventions in view of the high-risk of failure. The only certainty with such a conservative approach, however, was dense amblyopia in the affected eye. In view of our recent success with SLET in adults1 we decided to try this new technique of LSCT instead of CLET in this child. SLET has the advantage over CLET of being a single-stage procedure, easily replicable, and not requiring expensive laboratory support; while retaining the main benefit of CLET in using minimal donor tissue.1
SLET effectively restored the corneal surface and improved vision in the recipient eye without harming the donor eye. It must also be acknowledged that factors other than the surgical technique may have contributed to the final clinical outcome such as immediate and proper surgical management in the acute phase and spacing of the subsequent procedures with adequate gaps of several months to allow for the ocular surface inflammation to subside. This case also highlights two additional points. First, that complicated cases of ocular burns may take more than one surgical procedure for optimum clinical outcome. It is therefore important for both the physician and the parents to remain committed to these children despite initial setbacks. Second, ocular surface restoration must be accompanied by adequate amblyopia therapy, which again requires a sincere and committed effort from the parents.
Learning point
-
This case illustrates that autologous simple limbal epithelial transplantation can be successful in restoring the ocular surface and improving vision even in a child with severe unilateral limbal stem cell deficiency following ocular burns, which is conventionally considered to be at high risk of failure of limbal transplantation.
-
Multiple surgical procedures may be required for visual rehabilitation of patients with complicated ocular surface burns.
-
In paediatric cases, ocular surface restoration must be accompanied by adequate amblyopia therapy.
Footnotes
-
Contributors VSS, SB, SB and IL were involved in conception and design, analysis and interpretation of the data. SB, VSS, IL and SB were involved in acquisition of the data, critical revision, drafting of manuscript. SB, VSS, IL and SB were involved in final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.