Article Text

Abstract
Background/aims: Age related macular degeneration (ARMD) is a common ophthalmological disorder that can significantly impair a patient’s ability to function independently and potentially have a dramatic impact on health related quality of life. The aim of this study is to evaluate the quality of life of patients with ARMD, through the use of utility evaluation, and assess whether clinicians and healthy volunteers appreciate the impact of ARMD on health related quality of life.
Methods: A standardised questionnaire using the time-tradeoff method of utility analysis was created to assess health related quality of life. This questionnaire was distributed to 115 patients with ARMD. A similar questionnaire was distributed to 142 healthy volunteers and 62 clinicians who were asked to assume that they had ARMD. Comparisons were made among the responses from the members of the three groups.
Results: There was a significant difference in the utility scores among respondents with mild, moderate, and severe ARMD when compared to members of the general public and clinicians who were asked to assume they had each severity of ARMD. For mild ARMD the mean utility scores were 0.932, 0.960, and 0.832, for the general public, clinicians, and patients respectively (F = 21.7; p <0.001). No significant difference was found between the community members and clinicians (p <0.166); however, the patient group differed significantly from the general public (p<0.001) and clinician (p <0.001) groups. The utility scores for moderate ARMD for the general public, clinicians, and patients were 0.918, 0.877, and 0.732, respectively. (F = 34.6, p <0.001). There was no significant difference between the general public and clinicians (p <0.143); however, the patient group differed significantly compared with the general public (p <0.001) and clinician (p <0.001) groups. The utility scores for people with severe ARMD in the general public, clinician, and patient groups were 0.857, 0.821, and 0.566, respectively (F = 45.5; p <0.001). No significant difference was shown between the community members and clinicians (p <0.386); however, a significant difference was seen when comparing the patient group with the community member and clinician (p<0.001) groups.
Conclusion: Clinicians and community members may greatly underestimate the impact of mild, moderate, and severe ARMD on health related quality of life.
- age related macular degeneration
- quality of life
- utility scores
Statistics from Altmetric.com
Age related macular degeneration (ARMD) is one of the most common causes of vision loss in the United States.1 The progressive deterioration in central vision that is typical in patients with ARMD often precludes performance of activities of daily living, such as reading and driving. The impact that this ocular condition has on health related quality of life can be devastating.2
As health policy makers look to reform the US healthcare system, many believe that patient perspectives regarding quality of life with various health states should be considered. A technique that has been gaining popularity as an effective means of quantifying health related quality of life is the time-tradeoff method of utility analysis.3 Like other measures of quality of life, such as the Short Form 36 (SF-36),4 the Quality of Well-Being Index,5 and the Activities of Daily Vision Scale,6 utility measures such as the time-tradeoff and standard gamble techniques have been proved to be reliable and valid predictors of health related quality of life.7 However, these methods have the unique advantage of quantifying quality of life by generating a possibly more encompassing8 numerical value, known as a health status indicator, which represents one’s quality of life in a given health state.8 Such a score can be used by investigators to make quality of life comparisons between age related macular degeneration (ARMD) and other medical conditions. Moreover, these scores can be incorporated into analyses to determine the cost effectiveness of various interventions.
The purpose of this study was to utilise the time-tradeoff method of utility assessment to quantify the quality of life of a group of patients with ARMD and to assess whether members of the general public without ARMD and medical clinicians who treat patients with ARMD can appreciate the impact that ARMD has on quality of wellbeing.
MATERIALS AND METHODS
Participant selection
Enrolment criteria included an age of 18 years or older and an ability to complete a self administered questionnaire. Three groups of respondents were enrolled—patients with ARMD, members of the general public who denied having ARMD, and clinicians. Patients were considered to have ARMD if, on ophthalmic examination, the posterior segment showed macular drusen in association with retinal pigment epithelial disturbances. Patients with bilateral disciform scars were assumed to have acquired these scars secondary to ARMD. We stratified patients with ARMD into three groups on the basis of best corrected visual acuity (BCVA): patients with a BCVA in the better eye of 20/30, 20/40 to 20/100, and 20/200 or worse were considered to have mild, moderate, and severe ARMD, respectively.
The clinician group included third and fourth year medical students, house officers, and attending physicians from US medical centres. Ophthalmic clinicians were excluded. Patients with ARMD were recruited from two of the authors’ (GCB and MMB) clinical practices. Members of the community asked to assume they had each severity of ARMD were recruited on a random basis from various public places—such as parks and busy city streets in downtown Philadelphia. Each participant was given an explanation of the study purpose before providing consent to participate. This study was approved by the institutional review board of Wills Eye Hospital, Philadelphia, Pennsylvania.
Time-tradeoff methodology
Using the time-tradeoff technique of utility assessment, a questionnaire was designed to quantify respondents’ health related quality of life. The questionnaire consisted of two sections. The first section asked personal and demographic information, including age, sex, and race/ethnicity. In the second section there was a two part question:
How many additional years do you expect to live?
For the following question, assume that you are a patient suffering from (mild, moderate or severe age related macular degeneration). Suppose researchers developed a new technology that could permanently cure you of this condition. The technology always works but decreases your survival. Essentially, the treatment theoretically enhances your quality of life, but decreases the length of time you live. What is the maximum number of years, if any, that you would be willing to give up if you could receive this technology and be cured forever of this condition?
Members of the general public and clinicians were asked how much of their theoretical remaining time they would be willing to forego for each level of ARMD severity—mild, moderate, and severe. Patients with ARMD were not asked about mild, moderate, or severe disease, but only about their clinical situation. The data were collected for consecutive ARMD patients, clinicians, and members of the general public over a 1 year period from February 2000 to February 2001. Data on respondents from the general public who were employed in the healthcare industry but who did not directly treat patients with ARMD were eliminated from our analysis to prevent potential bias. Other reasons for exclusion were admission by a clinician that he/she has ARMD; failure to report current age or oldest age to which one expects to live (which precludes calculation of a utility score); or expression of the age to which one expects to live to be as “forever” or as a non-specific value, such as “80+ years.” For people whose response for expected maximum age was expressed as a range, such as “80–90 years,” we used the average of the two outer limit values to calculate a utility score.
Calculation of utility scores
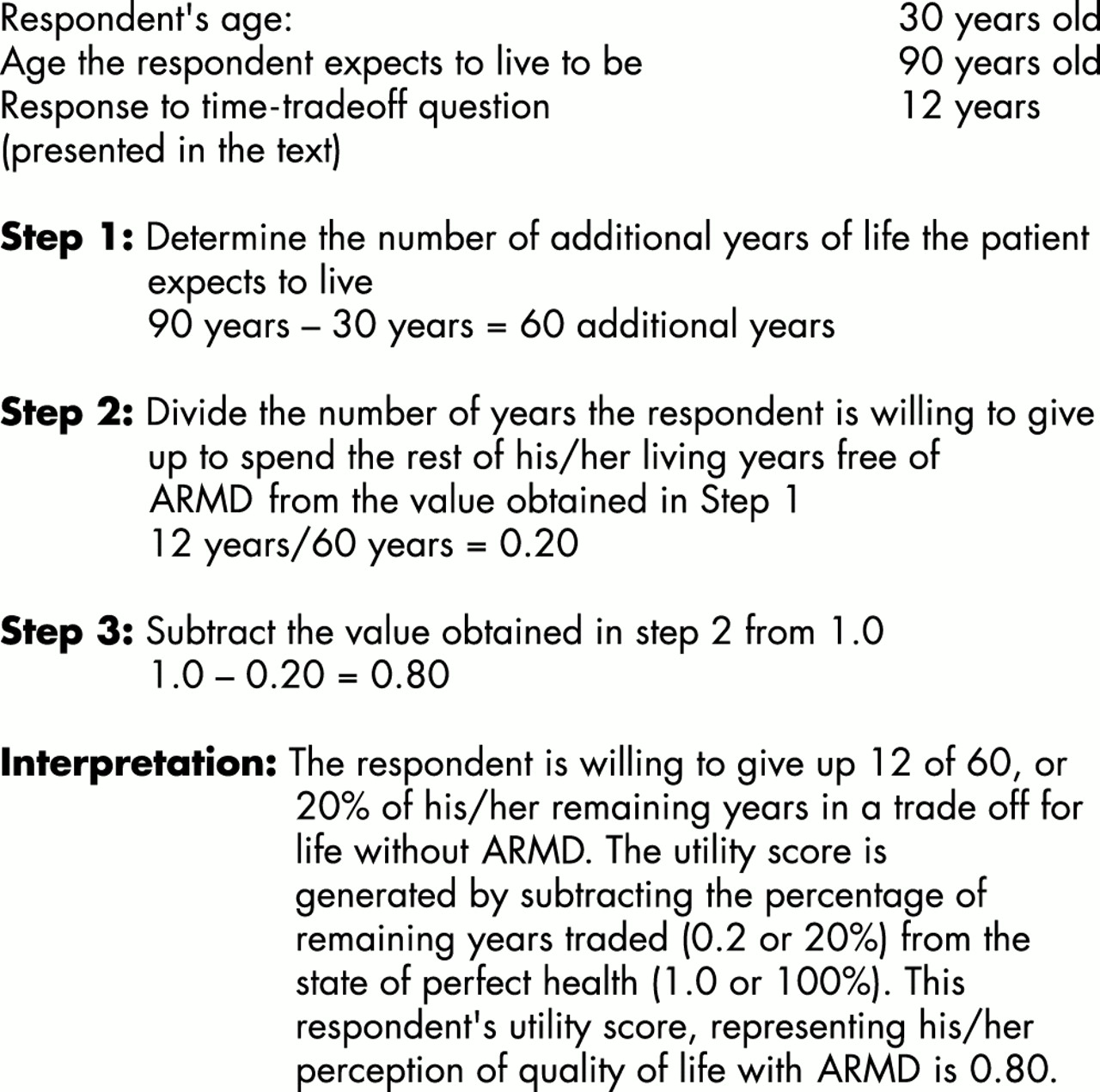
By incorporating the participants’ stated age, the estimated age to which they expect to live, and maximum number of years they would theoretically be willing to forego in order to be cured permanently of ARMD, the time-tradeoff technique was employed to generate a utility score for each respondent. The utility score is a representation of the relative desirability of a particular state of health for a specified length of time compared with the reference states of death (utility score = 0) and perfect health (utility score = 1.00).8–12Figure 1 shows the method used to calculate utility scores. This methodology has been described previously.3,10,11

{kind=link}
An example of how to calculate a utility score.
Statistical analysis
All data were calculated using SPSS, version 10.1 for Windows (SPSS, Chicago, IL, USA). Descriptive characteristics of the sample were calculated for the entire cohort and for each of the three groups. Sample size was determined using Sample Power 2 (SPSS, Chicago, IL, USA). Assuming a two sided α of 0.05 and a minimum mean difference of 15% in mean utility values among the cells, 34 patients were needed per group to have a power of 90%. A one way analysis of variance (ANOVA) was performed to determine whether between group differences were significant for current age, and the χ2 test was used to evaluate the categorical variables of race/ethnicity and sex. Mean utility scores and categorised utility scores were generated for each of the three groups for mild, moderate, and severe ARMD. A one way ANOVA was used to detect any significance in the difference among the three groups for utility score. If a significant difference was detected, the Bonferroni multiple comparison test was employed to determine which groups differed significantly from the others.13 A one sample Kolmogorov–Smirnov (KSZ) test was performed to assess whether each set of utility scores follows a parametric or non-parametric distribution.13 For utility scores confirmed as non-parametric by the KSZ test, a Kruskal-Wallis test was employed to determine significant differences in the utility scores of respondents from each group.14 For all tests, a p value less than or equal to 0.05 was considered statistically significant.
RESULTS
Among 339 people who filled out the health related quality of life questionnaire, 15 (4.4%) were excluded from our analysis because of failure to state current age, age to which respondent expected to live, or the number of years traded. The proportion of participants excluded from our analysis was similar in the general public group and the ARMD patient group. Of the 324 participants (95.6%) whose data were included in our analysis, 115 (35.5%) had ARMD, 142 (43.8%) were community members who denied having ARMD, and 62 (19.1%) were providers of care. Among the 115 respondents with ARMD, 34 (29.6%) cases had mild disease, 47 (40.9%) had moderate disease, and 37 (32.2%) had severe disease.
Table 1 shows the demographic characteristics for the study sample stratified by group. There was a significant difference in age among the groups (p <0.0005). Patients with ARMD were the oldest (mean 75.1 years) followed by the general public (mean 44.3 years) and then the clinicians (mean 29.0 years). Women constituted 64.7% (n=77) of the patient group, 57.7% (n=86) of the general public group, and 42.1% (n=24) of the clinician group. The difference in sex among respondents from the three groups was statistically significant (χ2 = 7.70; df=2; p = 0.021). For patients with ARMD, 99.2% were white compared with 89.3% of the community members and 75.9% of the clinicians. Using the χ2 test, this difference in race-ethnicity was also deemed to be significant. (χ2 = 25.29; df=2; p <0.0001).
Demographic characteristics of participants
Comparisons by severity of ARMD
Mild
Table 2 shows the distribution of utility scores for the three groups for mild, moderate, and severe ARMD. The utility scores for respondents with mild ARMD in the general public, clinician, and patient groups were 0.932, 0.960, and 0.832, respectively. Differences in utility scores among the groups using the ANOVA were significant (F = 21.7; p <0.001). No significant difference was found between the community members and clinicians (p <0.166) when the Bonferroni method of accounting for multiple comparisons was employed; however, the patient group differed significantly from the general public (p<0.001) and clinician (p <0.001) groups. Since the KSZ test showed the utility scores to follow a non-parametric distribution (KSZ = 4.29, p <0.001), the Kruskal-Wallis test was performed, which also demonstrated a statistically significant difference among the three groups of respondents (Kruskal-Wallis χ2 = 16.33; df = 2; p <0.0001).
Utility scores by group for each severity of ARMD
Moderate
The utility scores for moderate ARMD for the general public, clinicians, and patients with moderate ARMD were 0.918, 0.877, and 0.732, respectively. There was a significant difference in utility scores among the groups, using the ANOVA (F = 34.6, p <0.001). There was no significant difference between the general public and clinicians (p <0.143) when the Bonferroni method of accounting for multiple comparisons was employed; however, the patient group differed significantly compared with the general public (p <0.001) and clinician (p <0.001) groups. Using the Kruskal–Wallis test also showed a statistically significant difference among the three groups (Kruskal–Wallis χ2 = 34.06, df = 2; p <0.0001).
Severe
The utility scores for people with severe ARMD in the general public, clinician, and patient groups were 0.857, 0.821, and 0.566, respectively. There was a significant difference in utility scores among the groups using the ANOVA (F = 45.5; p <0.001). When the Bonferroni method of accounting for multiple comparisons was employed, no significant difference was shown between the community members and clinicians (p <0.386); however, a significant difference was seen in a comparison between the patient group compared with the community members and clinicians (p <0.001) groups. Using the Kruskal–Wallis test also showed a statistically significant difference among the three groups (Kruskal–Wallis χ2 = 51.34; df = 2; p <0.0001).
DISCUSSION
Utility analysis was originally designed to assess individual preferences under situations of uncertainty, and to assist individuals in making rational decisions when faced with uncertainty.3 Recently investigators have applied this method to the field of medicine to appreciate how individuals make difficult decisions regarding their health. The current investigation utilised the time-tradeoff method of utility analysis to quantify the health related quality of life of patients with mild, moderate, and severe ARMD. We also sought to determine whether members of the general public and clinicians could appreciate the impact that this sight threatening condition can have on quality of wellbeing.
The mean utility scores representing quality of life for individuals with mild, moderate, and severe ARMD were 0.832, 0.732, and 0.566, respectively. These values indicate that, on average, individuals with more clinically severe ARMD have a self perception of health related quality of life (HRQOL) that is significantly worse than that of individuals with more mild ARMD. Investigators who have used other, more traditional, quality of life measures such as the Activities of Daily Living Scale, the Instrumental Activities of Daily Living Index, and the Quality of Well-Being Scale, also have found a decrease in perceived HRQOL among patients as the severity of ARMD increases.2,15 Similar to the findings from the current investigation, Mangione found that individuals with more clinically severe ARMD had poorer scores on the Activities of Daily Living Scale, reflecting a decrease in perceived HRQOL.15 These studies and a study by Hazel and colleagues found that the inability to perform certain tasks, such as driving a vehicle or reading, significantly affected one’s quality of wellbeing.2,15,16
The importance of recognising the impact that ARMD has on HRQOL is twofold. Firstly, it justifies the allocation of more resources to support efforts to retard the progression of ARMD. Secondly, it serves as an impetus to create low vision aids and other devices that enable those with poor vision to continue with activities of daily living.
A benefit of the time-tradeoff method of utility analysis over a number of the more traditional measures of quality of life is the generation of a single score representing an individual’s quality of life in a given state of health. Mean utility scores for mild, moderate, and severe ARMD can then be compared to scores generated for other medical conditions to appreciate the relative desirability of living with one versus another medical condition. Table 3 compares the mean utility scores for mild, moderate, and severe ARMD with previously reported utility values.11,17–20 As the table indicates, the mean quality of life score for moderate ARMD is similar to that of class II coronary heart disease; quality of life with severe ARMD is slightly worse than class III or IV coronary heart disease. From the conditions listed in the table, the only two conditions for which patients have been willing to trade a greater amount of time than severe ARMD are bilateral blindness and severe cerebrovascular disease, which often affects multiple sensory and motor modalities—including vision. Our contention that impaired vision has a devastating impact on HRQOL is further supported by a report by Williams and colleagues who used the Quality of Well-Being Scale and Profile of Mood States2 to assess quality of life and emotional distress. They found that the HRQOL for ARMD is significantly worse than that for age matched controls as well as for individuals suffering from other chronic medical conditions such as chronic obstructive pulmonary disease, acquired immunodeficiency, and those undergoing bone marrow transplantation.2
Utility scores for various health states*
The second goal of this investigation was to assess whether members of the general public and clinicians who manage patients with ARMD can appreciate the impact this condition has on HRQOL. When comparing the mean utility scores for the patients with mild, moderate, and severe ARMD versus the utility scores for members of the general public and clinicians asked to assume they have each severity of ARMD, we found that members of the general public and clinicians considerably underestimate the impact that mild, moderate, and severe ARMD has on quality of wellbeing. Deduced from the mean utility scores, Table 4 shows how many days respondents from the general public, clinicians, and patients with each severity of ARMD would be willing to forego to live the remainder of time free of each severity of ARMD if they were to live only one more year. As the table illustrates, neither the general public nor the clinicians can appreciate how devastating an impact this condition can have on quality of life.
Number of days members of each group would forego to live the remainder of one additional year free of each severity of ARMD*†
This is, to the best of our knowledge, the first study of its kind seeking to assess whether non-ophthalmic clinicians can fully appreciate the impact that ARMD has on HRQOL. Ophthalmologists, however, when posed the same clinical questions, also dramatically underestimated the deleterious effect upon patient quality of life caused by ARMD.21 A number of investigators have performed similar analyses for other medical conditions. The observed discrepancy between the preferences of clinicians and patients has been demonstrated for hypertension, multiple sclerosis, depression, and total hip arthroplasty.17,22–24 A study by Jachuck found that in a sample of 75 patients taking antihypertensive medications, 100% of the doctors caring for these patients felt the quality of life of their patients improved after initiating therapy with antihypertensive medications.25 In comparison, only 48% of the patients reported an improvement in health related quality of life and 98% of the patients’ relatives/companions in the study actually believed that the quality of life of their significant other deteriorated after being placed on antihypertensive therapy.25
There are a number of possible reasons why the general public and clinicians underestimate the impact that ARMD has on HRQOL. Members of the general public may not fully understand or appreciate that ARMD causes blurring and distortion of central vision. They may not take into consideration the numerous limitations resulting from decreased visual acuity such as difficulty in reading, driving, or performing activities of daily living without assistance. Moreover, the public probably does not appreciate the cost of frequent visits to the ophthalmologist and low vision aids, the increased risk of sustaining additional injuries such as hip fractures from accidents attributed to poor vision, or the anxiety of not knowing if or when the dry form of ARMD may convert to the wet form of ARMD resulting in rapid loss of remaining vision. For the clinicians, they too may not fully appreciate the consequences of vision loss. Alternatively, this group may have confidence that in the near future there will be effective therapies to limit or prevent vision loss. However, to date there is no proved method for preventing loss of vision or restoring vision for the majority of patients with ARMD.
As with any study, there are potential inherent weaknesses in the present study. Some investigators critical of using the time-tradeoff technique to assess HRQOL have questioned whether humans are able to adequately integrate complex probability information when making decisions that involve risk.26 Despite such criticisms, the time-tradeoff method of utility assessment has been found to demonstrate validity, reliability, and reproducibility, and it serves as an appropriate tool for assessing the relative importance of various health states.7,8
A potential source of bias in the current study is the difference in demographic characteristics between respondents from the various groups. The group of clinicians includes third and fourth year medical students and house staff, who lowered the average age for this group. Moreover, individuals with known ARMD tend to be older in age as this condition is a chronic progressively debilitating disorder. A second possible source of bias is the significant difference in sex and racial/ethnic makeup among members of the three groups of respondents. Since ARMD is significantly more prevalent in white people compared to other racial groups and this condition affects females more than males, we would expect to see a greater representation of white females in the patient group compared to the other two groups of respondents.27,28 Arguably, further analyses comparing the utility scores for ARMD patients versus age, racial/ethnic, and sex matched controls should be performed to eliminate these potential confounding variables. Finally, it is important to recognise that individuals with ARMD have an increased risk for comorbid psychiatric illnesses, such as depression and anxiety disorders which could certainly affect responses to time-tradeoff questions.2
Our finding that members of the general public and clinicians considerably underestimate the HRQOL from ARMD is noteworthy. Based on the findings from this study, we contend that policy makers seeking input from the general public to help determine how to best allocate resources for medical conditions will better appreciate the severe public health problem that ARMD poses. Our findings suggest that even healthcare professionals do not fully appreciate the impact that ARMD has on HRQOL. Indeed, only the patients themselves best appreciate what it is like to suffer from ARMD.
Acknowledgments
Supported in part by the Retina Research and Development Foundation and the Volunteer Faculty Research Award, Thomas Jefferson University, Philadelphia, PA, USA; the Canadian Foundation for Innovation, Ottawa, Ontario, the Canadian Institutes for Health Research, Ottawa, Ontario, and an Ontario Ministry of Energy, Science and Technology’s Premier’s Research Excellence Award, Ottawa, Ontario, Canada.
The authors acknowledge Mrs Diana Coren and Ms Cristina Coren for their help with collecting data for this study.
References
Footnotes
Series editors: G and M Brown