Article Text

Abstract
Aim: To determine preoperative demographic, clinical, and optical coherence tomography (OCT) factors which might predict the visual and anatomical outcome at 1 year in patients undergoing vitrectomy and inner limiting membrane peel for diabetic macular oedema (DMO).
Methods: A prospective, interventional case series of 33 patients who completed 1 year follow up. Measurements were taken preoperatively and at 1 year. Outcome measures were logMAR visual acuity (VA) and OCT macular thickness. A priori explanatory variables included baseline presence of clinical and/or OCT signs suggesting macular traction, grade of diabetic maculopathy, posterior vitreous detachment, fluorescein leakage and ischaemia on angiography, presence of subretinal fluid, and peroperative indocyanine green (ICG) use.
Results: 33 patients completed 1 year follow up. On average VA deteriorated by 0.035 logMAR (p = 0.40). Macular thickness significantly improved by a mean of 139 μm (95% CI; 211 to 67, p<0.001). Patients with evidence of clinical and/or OCT macular traction significantly improved logMAR acuity (logMAR improvement = 0.08) compared with patients without traction (logMAR deterioration 0.11, p = 0.01). Presence of subretinal fluid significantly predicted worse postoperative result (p = 0.01)
Conclusion: On average, patients showed a statistically significant improvement in central macular thickness following treatment but a marginal acuity worsening. Presence of subretinal fluid on OCT is hypothesised to be exudative rather than tractional in nature. The visual benefit of vitrectomy for DMO in this study was limited to patients who exhibit signs of macular traction either clinically and/or on OCT.
- CMT, central macular thickness
- DD, disc diameter
- DMO, diabetic macular oedema
- ERM, epiretinal membrane
- FAZ, foveal avascular zone
- FFA, fluorescein angiography
- ICG, indocyanine green
- ILM, internal limiting membrane
- OCT, optical coherence tomography
- RCT, randomised controlled trial
- TTPH, taut thickened posterior hyaloid
- VA, visual acuity
- diabetic macular oedema
- vitrectomy
- diabetic retinopathy
- maculopathy
- optical coherence tomography
- CMT, central macular thickness
- DD, disc diameter
- DMO, diabetic macular oedema
- ERM, epiretinal membrane
- FAZ, foveal avascular zone
- FFA, fluorescein angiography
- ICG, indocyanine green
- ILM, internal limiting membrane
- OCT, optical coherence tomography
- RCT, randomised controlled trial
- TTPH, taut thickened posterior hyaloid
- VA, visual acuity
- diabetic macular oedema
- vitrectomy
- diabetic retinopathy
- maculopathy
- optical coherence tomography
Statistics from Altmetric.com
- CMT, central macular thickness
- DD, disc diameter
- DMO, diabetic macular oedema
- ERM, epiretinal membrane
- FAZ, foveal avascular zone
- FFA, fluorescein angiography
- ICG, indocyanine green
- ILM, internal limiting membrane
- OCT, optical coherence tomography
- RCT, randomised controlled trial
- TTPH, taut thickened posterior hyaloid
- VA, visual acuity
- diabetic macular oedema
- vitrectomy
- diabetic retinopathy
- maculopathy
- optical coherence tomography
- CMT, central macular thickness
- DD, disc diameter
- DMO, diabetic macular oedema
- ERM, epiretinal membrane
- FAZ, foveal avascular zone
- FFA, fluorescein angiography
- ICG, indocyanine green
- ILM, internal limiting membrane
- OCT, optical coherence tomography
- RCT, randomised controlled trial
- TTPH, taut thickened posterior hyaloid
- VA, visual acuity
- diabetic macular oedema
- vitrectomy
- diabetic retinopathy
- maculopathy
- optical coherence tomography
The majority of published reports1–3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35 regarding vitrectomy for diabetic macular oedema (DMO) are retrospective with varying inclusion criteria, methodology, and follow up. Most studies have suggested that the procedure is effective, particularly in those with clinically evident signs of a taut thickened posterior hyaloid (TTPH1). In the first published randomised controlled trial (RCT) on this subject we found that vitrectomy with internal limiting membrane (ILM) peeling did not improve the visual acuity (VA) of patients with a clinically attached but otherwise normal posterior hyaloid.24 To investigate whether there are subgroups within which vitrectomy is an effective intervention we have prospectively studied a cohort of patients, all with 1 year follow up, who underwent vitrectomy for chronic DMO.
PATIENTS AND METHODS
Ethics approval was obtained (EC 00/004). Patients included were over 21 years of age with diffuse or diffuse and focal DMO in an eye that had already received one or more grid laser treatments no less than 3 months previously. VA of Snellen 6/12 or worse and the ability to give informed consent was required. Exclusion criteria were acuity impairing ocular co-morbidity, active proliferative retinopathy, uncontrolled hypertension (blood pressure >140/95) or severe renal impairment. VA was measured in logMAR using a standardised methodology.24
The vitreous, macula, and vitreomacular interface were examined clinically (DAHL) for the features of a PVD, TTPH, and epiretinal membrane (ERM). PVD was defined as a Weiss ring or continuous folded layer of optically dense vitreous behind which no normal vitreous structure could be clinically defined. Preoperative colour imaging and fluorescein angiography (FFA) was performed using the standard 30 degree seven field Diabetic Retinopathy Study protocol.36
Images were graded by the Retinopathy Grading Centre, London. The presence of haemorrhages, microaneurysms, and exudates in field 2 photographs (macula) were each graded 0–5 against standardised photographs,37 with the results averaged to produce a maculopathy score (0–5). FFAs were graded for ischaemia and leakage. Ischaemia was graded from 0–4: four quadrants were marked out within a 0.5 disc diameter (DD) marker centred on the fovea. Grade 0 meant the foveal avascular zone (FAZ) remained within all the quadrants. FAZ breakout from a quadrant increased the grade by one. The percentage area of leakage was graded between 0 and 5. A central 2 DD marker was placed on the fovea. Grade 0 was no leakage, grade 1 meant up to 20% of the marker area with leakage; grade 2 meant 20–40%, and so on.
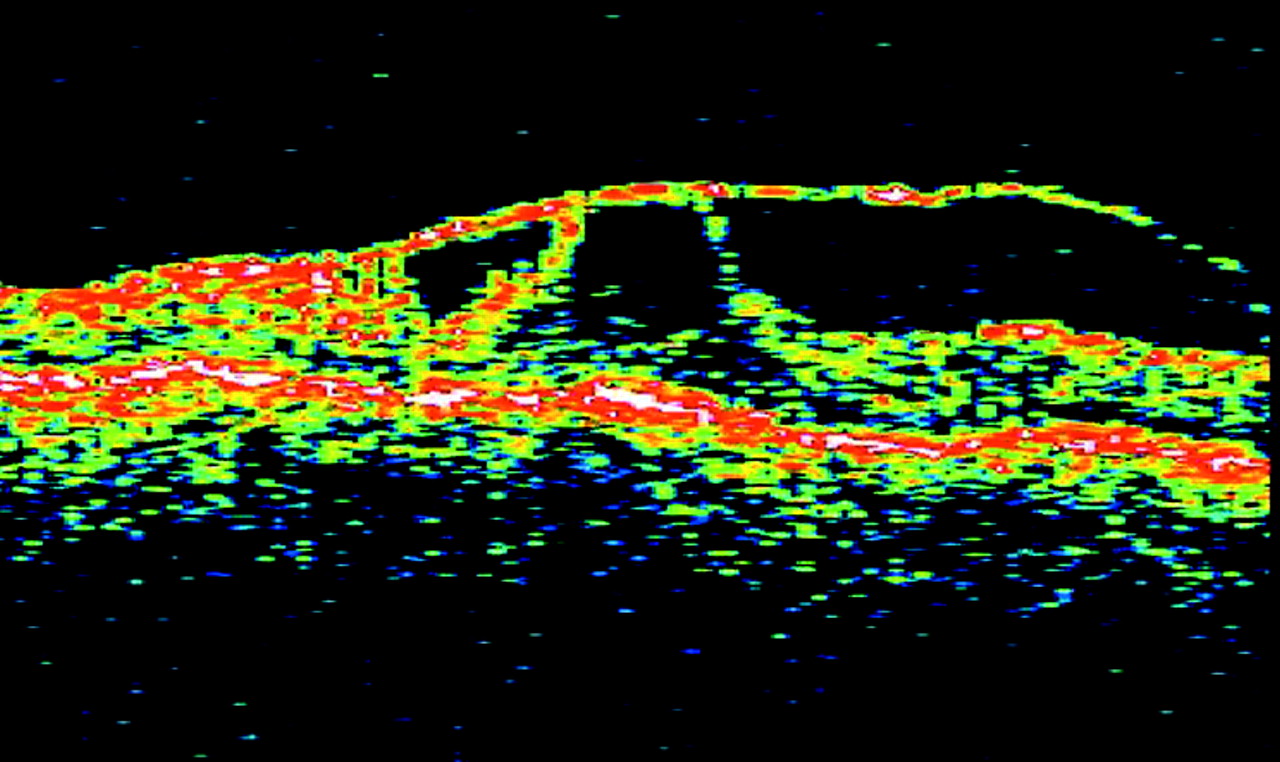
Automated OCT measurements of mean central macular thickness (CMT) based on six radial scans were employed.24 OCTs were graded (SS and DAHL) to identify signs suggesting macular traction (retinal surface peaking, epiretinal membrane, and focal or multifocal partial vitreomacular separation) and subretinal fluid (fig 1).

OCT image showing partial vitreomacular separation with multifocal traction.

{kind=link}
{kind=link}
OCT image showing presence of subretinal fluid.
The intervention consisted of a PPV with posterior hyaloid detachment if not present and ILM peeling. ICG staining was conducted on 21 patients. For this purpose aqueous ICG solution (Pulsion) diluted with Alcon BSS to 0.5 mg/ml was used. All surgery was conducted by one surgeon (DAHL).
Potential predictors examined were presence of macular traction (clinical and/or OCT signs suggesting traction), PVD, maculopathy, ischaemia and leakage grades, SRF, and ICG use.26,27 Primary outcome measures were (1) best corrected logMAR VA at 1 year, (2) CMT.
Statistical analysis
Inverse normal plots confirmed normal distribution. Paired t tests were used to compare outcome measures. Univariate and multivariate linear regression undertaken with VA (or CMT) difference as the dependent variable in each model. Pairwise pearson correlation coefficients were calculated for VA change against CMT change and for baseline VA against VA change.
RESULTS
In all, 33 patients forming the study population were followed up for 1 year postoperatively. This includes the 14 previously reported trial patients who completed 1 year follow up.24 Mean age was 65.4 years; there were 14 female patients. Quantitative OCT data were lost on three patients. One set of images was unreadable. Baseline characteristics and 1 year outcomes are shown in table 1. Included in the study were 18 patients with a clinically normal attached posterior hyaloid (of whom four had OCT signs suggestive of traction), six had a TTPH, one had an epiretinal membrane with OCT signs of epiretinal traction, seven had PVD but no clinical or OCT signs suggestive of traction, and one patient had a PVD and clinically normal macular surface but undetermined OCT appearance because of missing qualitative data.
Baseline and 1 year characteristics
Overall, there was a mean worsening of +0.035 logMAR (range +0.62 to −0.30, CI −0.05, +0.12, p = 0.40). CMT significantly improved from baseline with a reduction of −139 μm (range −497 μm to +324 μm, CI −21 to −671, p<0.001), with 17 (57%) patients having a CMT of less than 300 μm at 1 year. No significant correlation was found either between baseline acuity and change in VA (r = −0.31, p = 0.08) or VA change and CMT change (r = 0.08, p = 0.63.)
There was no difference in baseline vision (p = 0.82), CMT (p = 0.18) and presence/absence of pseudophakia (p = 0.97) between groups with and without macular traction. The six patients with a clinical TTPH improved by a mean −0.06 logMAR (range −0.26 to +0.24) and −95 μm (−194 to 109), while the five who had OCT signs of traction but did not have a clinical TTPH showed a mean improvement of −0.1 logMAR (range −0.24 to 0.0) and CMT reduction of −262 μm (range −497 μm to −69 μm). The 22 patients who had neither a clinical TTPH nor traction on OCT had a mean VA deterioration of +0.11 logMAR (range +0.62 to −0.30) but a CMT improvement of −117 μm.
The results of the multivariate regression modelling revealed that both macular traction and SRF at baseline significantly predicted visual outcome (table 2). No covariates were found to be statistically significant predictors of CMT outcome.
Changes in visual acuity with the preoperatively determined risk factors
DISCUSSION
Vitrectomy has recently been investigated as an alternative treatment to laser photocoagulation. The clinical entity of a TTPH was first described by Lewis et al,1 who suggested that the hyaloid in these circumstances exerts tangential traction on the retinal surface inducing or exacerbating oedema and that relief of this traction resulted in visual improvement. Kaiser et al later published OCT data supporting the hypothesis that TTPH is associated with signs of traction.38 The importance of OCT imaging is increasingly being recognised and has now revolutionised the clinical analysis of the vitreomacular interface.39–41 OCT features suggesting vitreoretinal traction may however occur in the absence of a clinical TTPH. This was the case in four patients included in this study. Massin et al have retrospectively reported an improvement of two lines in 70% (5/7) of patients with OCT features of traction, compared to only 12.5% (1/8) rate of two line improvement and a median doubling of the visual angle from 20/100 to 20/200 in seven patients without OCT evidence of traction.7 OCT data from prospective studies12,13,34,35 all report a reduction in CMT postoperatively; however, correlation of CMT reduction with VA improvement must be made with caution34 and we found no evidence of such a relation (p = 0.63). Reasons for this may include photoreceptor dysfunction following chronic oedema, multiple laser photocoagulation induced damage, or macular perfusion abnormalities.
Excluding our RCT, 10 other prospective studies,12,13,17,25–29,34,35 which in total include 178 eyes, have been conducted in this field. The findings suggest that vitrectomy may be beneficial; 100/178 eyes (56.2%, range 50%–78%) demonstrated an acuity improvement of two or more lines at final follow up; however, results of the RCT found no statistically or clinically significant difference in acuity or CMT between the control and vitrectomy groups.24
The results in this study show 15% (5/33) and 24% (8/33), respectively, improving or deteriorating by two or more ETDRS logMAR lines. Patients identified with macular traction had an approximately 1 logMAR line improvement in acuity compared to a one line deterioration in the 22 patients without any evidence of macular traction (regression coefficient −0.25, CI −0.05 to −0.43, p = 0.01). The presence of SRF on OCT was associated with an adverse visual outcome (mean deterioration of 0.33 logMAR, CI +0.08 to +0.62, p = 0.01). Only one of these four patients had macular traction; from this we hypothesise that in patients with DMO, SRF may have an exudative component as well as being a tractional phenomenon as suggested by Kaiser et al.38 We are not aware that SRF has previously been identified to be a potential adverse prognostic sign. No other a priori variables were found to influence the postoperative outcome.
A potential restriction to the VA improvement of patients is progression of cataract following vitreous surgery. We performed prospective Scheimpflug measurements on our RCT patients and found no statistically significant difference in progression of lens opacity in the first postoperative year.24
The findings of this study run parallel to those reported by Massin et al7 but are at odds with the other prospective data on this subject. Included in these reports are the data recently reported by Recchia et al in which only 2/11 patients had any OCT signs suggesting macular traction but mean VA improved from 20/352 to 20/119.34 Reasons for these differences are not immediately obvious but may include racial factors, disease duration and severity, extent of previous laser and macular ischaemia, a small and unconsciously biased sample on our part, and/or positive reporting bias on the part of other series.
We recognise the limited power of this study; however, our findings suggest that the benefits of vitrectomy for chronic DMO are limited to patients with clinical and/or OCT signs suggestive of traction. Macular detachment on OCT may additionally be an adverse predictive indicator.
REFERENCES
Footnotes
-
The authors have no commercial or proprietary interest in this article.
Linked Articles
- BJO at a glance