Article Text

Abstract
Aims: To determine the contrast sensitivity (CS) in 10 year old prematurely born children, previously included in a population based study on the incidence of retinopathy of prematurity (ROP), and in full term controls.
Methods: This study included 205 prematurely born children and 215 children born at term, from the same geographical area and study period. CS was assessed monocularly with the Vistech 6500 test at five spatial frequencies (1.5–18 cycles/deg).
Results: Prematurely born children had statistically significant lower CS at all frequencies, compared to full term ones. The mean differences in logarithmic CS were 0.03 (1.5 cycles/deg), 0.09 (3 cycles/deg), 0.10 (6 cycles/deg), 0.12 (12 cycles/deg), and 0.19 (18 cycles/deg). Even when the children with ROP and neurological disorders were excluded there was a difference between the two groups. Children who had been treated with cryotherapy had the lowest CS.
Conclusion: CS was lower in 10 year old prematurely born children than in full term ones of the same age. Whether this finding affects their visual function in daily life is uncertain.
- CS, contrast sensitivity
- ROP, retinopathy of prematurity
- VA, visual acuity
- VCTS, Vistech contrast sensitivity test system
- prematurity
- retinopathy of prematurity
- contrast sensitivity
- children
- CS, contrast sensitivity
- ROP, retinopathy of prematurity
- VA, visual acuity
- VCTS, Vistech contrast sensitivity test system
- prematurity
- retinopathy of prematurity
- contrast sensitivity
- children
Statistics from Altmetric.com
- CS, contrast sensitivity
- ROP, retinopathy of prematurity
- VA, visual acuity
- VCTS, Vistech contrast sensitivity test system
- prematurity
- retinopathy of prematurity
- contrast sensitivity
- children
- CS, contrast sensitivity
- ROP, retinopathy of prematurity
- VA, visual acuity
- VCTS, Vistech contrast sensitivity test system
- prematurity
- retinopathy of prematurity
- contrast sensitivity
- children
Children born prematurely are known to have high prevalences of ophthalmological and neurodevelopmental disorders.1–3 Long term follow up studies of prematurely born children are important, since minor lesions and problems may not be detected until preschool or school age. Although investigations of visual function are mainly hospital based,1,2,4,5 some have been population based.6,7,8,9,10,11 Most studies have shown that prematurely born children have poorer visual acuity (VA) than full term ones. However, VA reflects visual function at maximum contrast and does not represent the visual conditions in daily life, in which objects show varying degrees of contrast. Visual function is also dependent on the contrast sensitivity (CS). The CS function is affected by optical conditions and neural processing in the retina or the posterior visual pathways,12 all of which may be disturbed in prematurely born children.
In Stockholm county, children with a birth weight of 1500 g or less, born in 1988–90, were included in a prospective population based study on the incidence of retinopathy of prematurity (ROP).13 They were followed for 3.5 years.9,14 At 10 years of age, an ophthalmological follow up was done, which included a control group of children born at term. Their refractive outcome,15,16 visual fields,17 and visual acuity18 have been described. The aim of the present paper is to report the CS function in both of these groups at 10 years of age and to evaluate the effects of prematurity itself, ROP, and of cryotreatment.
METHODS AND MATERIALS
In a previous prospective population based study on the incidence of ROP, we included 260 prematurely born children, born between 1 September 1988 and 31 October 1990, with a birth weight of ⩽1500 g13; 40% (105) had ROP and 11% (28) had been cryotreated. The criterion for treatment was ROP stage 3 in at least four contiguous clock hours in zone II, even in the absence of plus disease. All eyes fulfilling our criterion for treatment had been cryotreated.13
A detailed description of the cohort has previously been reported.9,15,18 During the first 3.5 years, 12 children were excluded.9,14 At 10 years of age, the children were relocated and the children/caregivers were asked whether they wished to participate in an ophthalmological follow up study. Of the 248 children, 32 dropped out and the 10 year follow up therefore included 216 prematurely born children, giving a follow up rate of 87.1% (216/248).
ROP was classified as no ROP, mild ROP (stages 1 and 2), and severe ROP (stages 3–5). Severe ROP was divided into “severe untreated” and “cryotreated” ROP.
We obtained 217 children, born at term (39–41 weeks) and having normal birth weights (3000–4000 g) from the Swedish National Board of Health and Social Welfare. They were randomly selected to provide a control group and were born in the same time period and geographical area as the prematurely born ones.
All children were examined at the age of 9 years 9 months to 10 years 3 months, except one prematurely born child who was examined at 10.5 years of age.
Best corrected distance visual acuity (VA) of each eye was assessed with logMAR charts.18 “Better eye” was defined as the eye with the better VA. In 13 prematurely born and 19 full term children, the VA was the same in both eyes. In these children the right eye was chosen as the “better eye.” To exclude the effect of amblyopia and strabismus on CS,19,20 only the results of the “better eyes” are given in the present study.
Retinoscopy during cycloplegia was performed.15 The spherical equivalent was calculated and astigmatism noted. Normal refraction was defined as a spherical equivalent ⩾0D and ⩽+3D, and astigmatism <1D. The anterior segment and fundus were examined.
The presence of a neurological complication was defined as an intraventricular haemorrhage in the neonatal period and/or obvious neurological sequelae in the 3.5 year follow up.9 Thirty four (15.7%) prematurely born children had some kind of neurological complication according to this definition. No examination by a paediatrician or magnetic resonance imaging was done at the 10 year follow up.
CS was assessed monocularly with the Vistech contrast sensitivity test system (VCTS 6500).21,22 The Vistech test measures the CS at five spatial frequencies, 1.5, 3, 6, 12, and 18 cycles per degree (cycles/deg), at a viewing distance of 3 metres. The chart contains circular plates with sine wave contrast grating with nine levels of contrast for each frequency. The logarithmic values of the CS were used for the analyses. When a child could not see the plate with the lowest CS (highest contrast), but otherwise cooperated in the test, it was given a CS value, which was half of the lowest value. This was done to obviate overestimating the CS, which would have occurred if the child had been excluded. All CS tests were performed with the child’s best refractive prescription. The assessments were masked to the examiner who was one of the authors (AR), an orthoptist and experienced in examining children and in CS testing.
The study was approved by the local ethics committee at Karolinska Institutet. Informed consent was obtained by the caregivers.
Statistical methods
The results of the “better” eyes were analysed for each spatial frequency. We compared the nominal or ordinal data with an independence test of contingency tables (Fisher’s test, asymptotic or exact). A one way ANOVA (controls versus prematurely born children divided into subgroups) was used to analyse continuous data. As the sample sizes were unbalanced and the variances not homogeneous, an ANOVA model with separate variance estimates23 was used. The p values were corrected, according to the Bonferroni procedure. We used the Mann-Whitney test for continuous data to compare prematurely born children with and without neurological complications and stepwise multiple regression analyses to evaluate the effects of gestational age (GA) at birth, birth weight (BW), stage of ROP, cryotreatment, neurological complications, refraction, and VA on CS in the “better” eye.
RESULTS
In this study of CS, 205 of the 216 prematurely born children were included—that is, 83% (205/248) of the original cohort. Of the 216 children, one child was blind because of retinal detachment and 10 were unable to cooperate because of a disability or poor concentration. Of the 217 full term children, two were excluded because of poor concentration. No child had a cataract or pseudophakia. The demographics are given in table 1.
Demographic data of the prematurely born and full term children
Two of the 205 prematurely born children could participate only binocularly and their CS was included in the analyses of the “better eye.” Of the 205 and 215 cooperating children, nine prematurely born and two full term ones did not see the lowest CS (highest contrast) at 18 cycles/deg and they were given a value that was half of the lowest CS. Moreover, two of the nine premature children and one of the two full terms did not see the lowest CS at 12 cycles/deg. Exclusion of these 11 children would not have changed the results of the analyses.
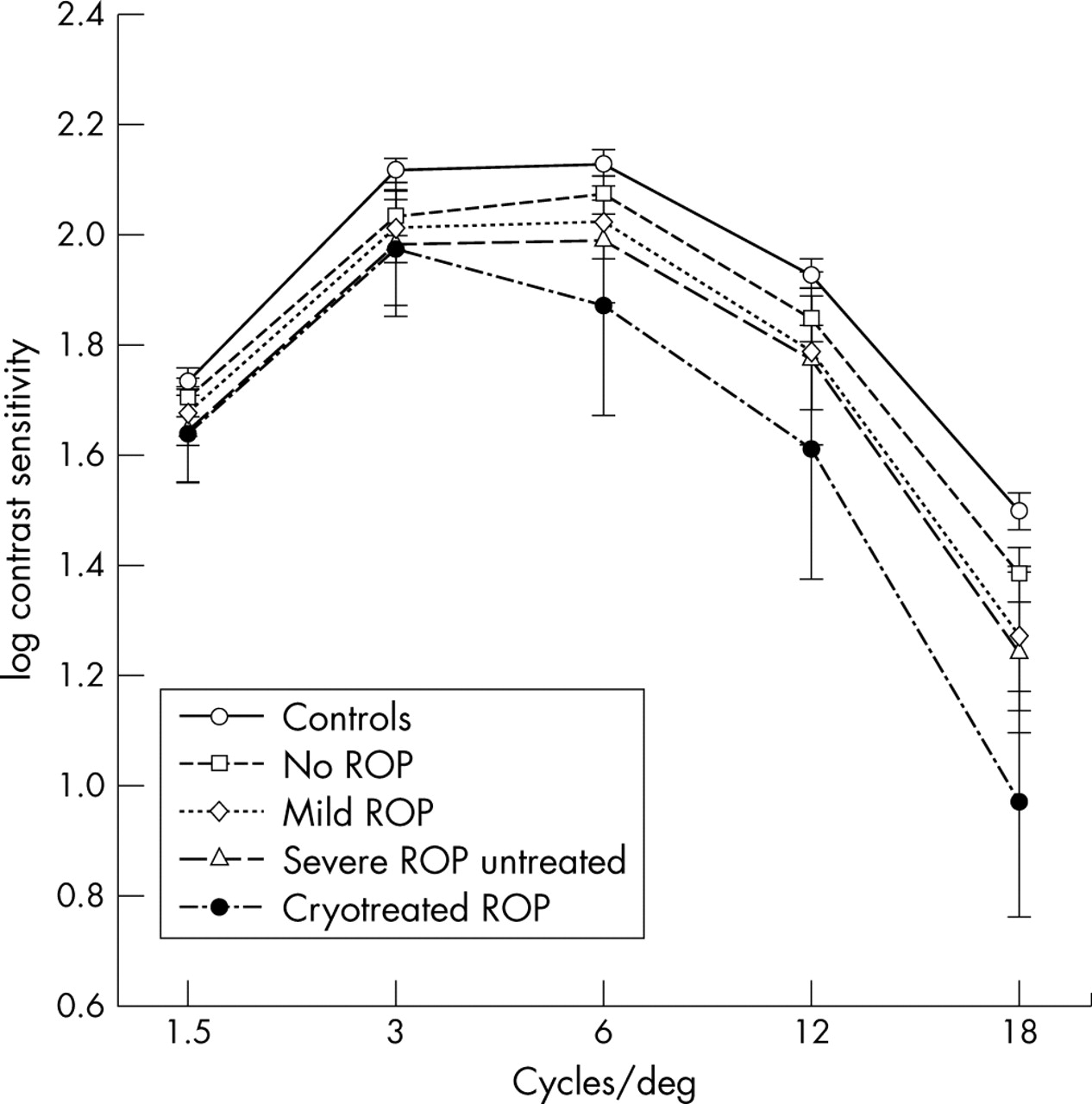
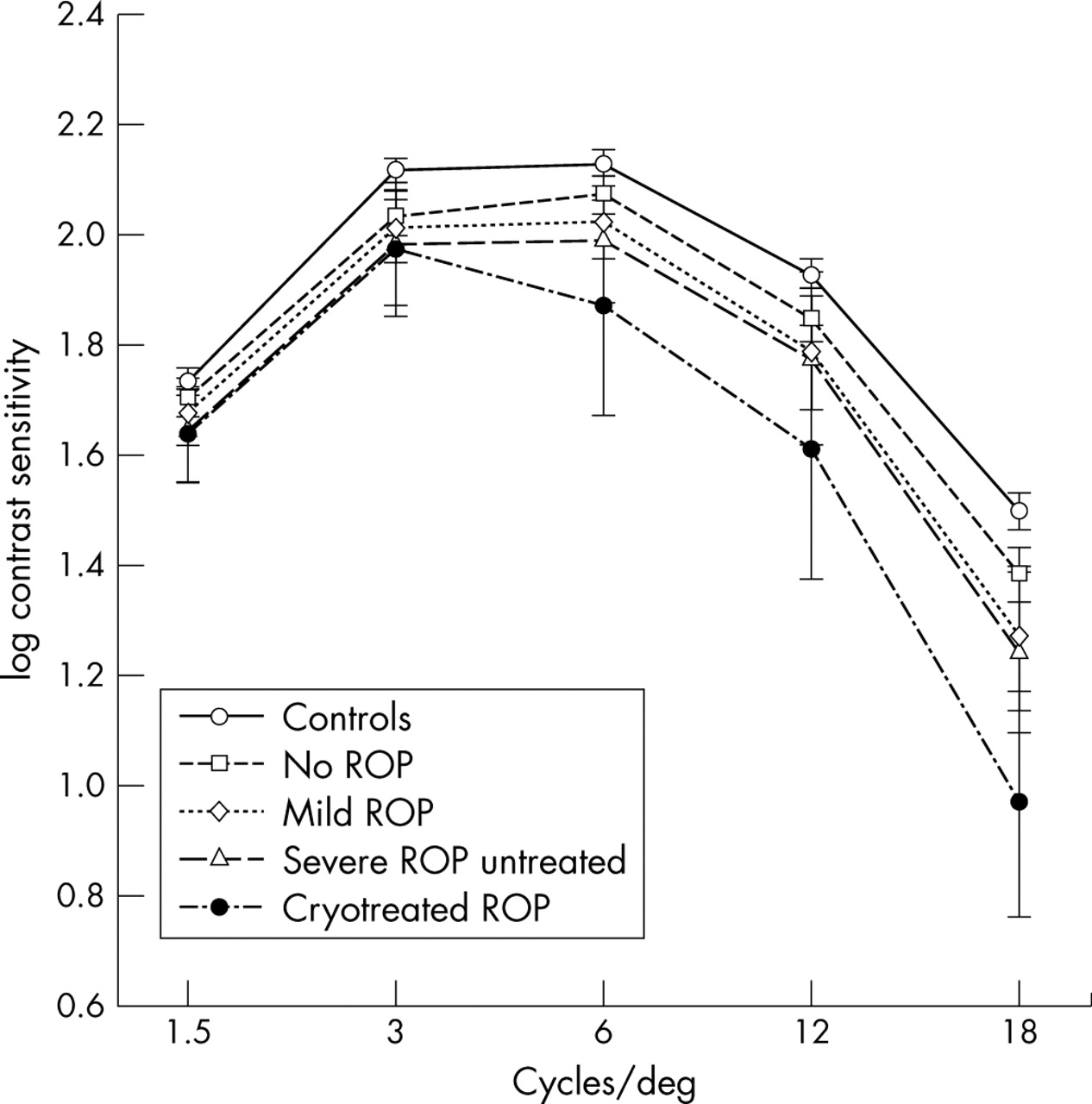
The mean logarithmic values of CS in the five spatial frequencies in the prematurely born and the full term children are given in table 2 and figure 1. We found significant differences in CS between prematurely born and full term children at all frequencies (p values see table 2), and also when children with previous ROP and neurological complications were excluded at 3 cycles/deg (p<0.001), 6 cycles/deg (p = 0.004), 12 cycles/deg (p = 0.003), and 18 cycles/deg (p<0.001).
Mean values (SD) of contrast sensitivity, assessed at five spatial frequencies, in the better eyes in prematurely born and full term children
{kind=link}
Mean values and 95% confidence intervals of contrast sensitivity function in prematurely born and full term children.
The peak of the maximum CS was at 6 cycles/deg in the full terms and in all subgroups of prematures, except in those who had been cryotreated. In the latter, the peak CS was at 3 cycles/deg, but the difference was not statistically significant (p = 0.26).
We also compared the two groups, but included only those with good VA (logMAR ⩽0) and normal refraction. Further, those with neurological complications in the premature group were excluded. The differences between the prematurely born (125) and full term (183) children were still significant at all frequencies, 1.5 cycles/deg (p = 0.02), 3 cycles/deg (p = 0.001), 6 cycles/deg (p = 0.003), 12 cycles/deg (p = 0.006), and 18 cycles/deg (p<0.001).
In the premature cohort, the children who had been cryotreated had the lowest CS at all frequencies, but the difference was statistically significant only at 18 cycles/deg (p = 0.001). However, we found no differences between the children without ROP and those with untreated ROP, or between prematurely born children with or without neurological complications at any frequency.
Multiple regression analyses were done for CS at each frequency in the prematurely born cohort, including GA at birth, BW, stage of ROP, cryotreatment, neurological complications, VA, spherical equivalent, and astigmatism as independent risk factors. At 1.5 cycles/deg, cryotreatment was of borderline significance (p = 0.06), but none of the other risk factors. At 3 cycles/deg (p = 0.01), 6 cycles/deg (p<0.001), and 12 cycles/deg (p<0.001), only VA was significant, and the correlation was greater at higher frequencies. At 18 cycles/deg, VA (p<0.001) and cryotreatment (p = 0.002) correlated with lower CS.
We also performed multiple regression analyses that included only children with good VA (logMAR ⩽0) and normal refraction. None of the risk factors was significant, although neurological complications were of borderline significance at 3 cycles/deg (p = 0.07). However, only a few (four) children who had been cryotreated were included in these analyses.
DISCUSSION
In this study of the CS in prematurely born and full term children, the former had a significantly lower CS even when we excluded those with neurological complications and previous ROP. Moreover, a difference in CS was also found between the groups when comparing only the children with good VA (logMAR ⩽0), without neurological complications and with normal refraction. In the cohort of premature children, those who had been cryotreated had the lowest CS at all frequencies. Reduced VA and cryotreated ROP correlated with a lower CS, while neurological complications did not, in the present study.
Several studies have evaluated the visual outcome in prematurely born children of similar ages.1,6,24 There are only three population based studies, apart from this one, in which 10 year old preterm children were screened prospectively for ROP in the neonatal period.7,8,11 Most authors have analysed the visual outcome at maximum contrast—that is, the VA. However, a few studies of prematurely born children describe the visual function at other levels of contrast.4,5,11,25–27 Of the three population based studies at about 10 years of age, only O’Connor et al11 report the CS findings.
In the present study, the CS was examined with the Vistech 6500 test, which measures the CS at five spatial frequencies (1.5–18 cycles/deg), but the tests used by other authors measured the CS at lower spatial frequencies.4,5,11,25–27 In the studies of prematurely born children, Dowdeswell et al,4 the American Cryo-ROP study,25 and O’Connnor et al11,27 all used the Pelli Robson test at 1 metre which assesses the CS at 1–1.6 cycles/deg.28 Jackson et al26 used a computerised technique that measures the CS at 0.22–3.5 cycles/deg and Cooke et al5 used the Cambridge test which measures it at 4 cycles/deg. The Vistech test measured the CS over a wider range of low and mid spatial frequencies and also enabled us to assess the peak of the maximum CS, normally at about 6 cycles/deg.29 The Vistech test is reliable and appropriate for children from about 5 years of age and the CS gradually increases into adulthood,30–32 although some authors claim superfluous information33 and a poor repeatability34 in the test. A wide range of normal CS has been reported, which overlaps at various ages31; however, the use of a control group born at term permitted the detection of minor differences between preterm and full term children. It is difficult to interpret whether the reduced CS itself, in the present study, was of clinical importance or just added to other differences in the visual function, such as the VA18 and the visual fields.17
O’Connor et al,11,27 Dowdeswell et al,4 and Cooke et al,5 likewise observed lower CS in prematurely born children than in those born at term, but Jackson et al26 found a similar CS in 7–13 year old preterm and full term children at frequencies from 0.22 to 3.5 cycles/deg. The differences in the results may be due to different methodology and epidemiology, such as the various tests used by the authors, measuring the CS at different spatial frequencies, and different inclusion and exclusion criteria.4,5,11,26,27
In accord with O’Connor et al,11 we observed no difference in CS between prematurely born children without ROP and those with untreated ROP. Although not statistically significant at all frequencies, the children with cryotreated ROP had the lowest mean CS and the highest prevalence of CS below normal. This was also confirmed by the multiple regression analyses, in which there was no correlation between ROP and a lower CS, whereas cryotreated ROP was a risk factor at 18 cycles/deg. In the American CRYO-ROP study,25 cryotreated eyes had better CS than those with untreated threshold ROP, which supports the view that treatment for threshold ROP has a beneficial effect.35 It is uncertain whether the reduced CS in the present study was due to the cryotreatment or to the severe ROP, since all children who fulfilled our criterion for treatment were treated.13
In this study, neurological complications according to our definition, were of no significance for a reduced CS, confirmed by the multiple regression analyses. Obvious neurological sequelae were, however, based on the 3.5 year follow up of the premature cohort.9 Since paediatric examination or magnetic resonance imaging was not performed in the 10 year follow up, minor neurological lesions could be an unrecognised reason for the reduced CS.
Certain types of losses in the CS curve may indicate differences in visual pathology.22,36,37 However, in clinical practice no diagnostic reduction in specific sensitivity has been found.38 Optical disturbances as well as retinal and neurological lesions may cause losses in CS at wide ranges of spatial frequencies.39–42 In this study, the prematurely born children had an overall reduction at all the spatial frequencies (1.5–18 cycles/deg) and we found no pattern that explained the cause of the reduction. Refractive errors played no part in the multiple regression analyses. Prematurely born children without ROP and neurological complications still had lower CS than children born at term. As in our previous studies of VA18 and visual fields17 on the same cohort, we could not determine whether the reduction in CS was caused by changes in the retina or the posterior visual pathways.
CS is regarded as the best way to measure visual function since it estimates the ability to detect daily life objects.37 Differences in visual performance in patients with the same VA may be due to differences in CS function.43 A correlation exists between VA and CS at high spatial frequencies26,38 and, in the present study, we also found this in the mid range frequencies, confirmed by the multiple regression analyses. However, although children with poor VA were excluded, the prematurely born children had significantly lower CS in the low and mid range spatial frequencies. Like studies of other ophthalmological disorders,44–47 this finding may explain visual problems despite a normal VA.
CONCLUSION
Prematurely born children with or without ROP and neurological complications had lower CS than those born at term. Children who had been cryotreated had the lowest CS, but we found no difference between those without ROP and untreated ROP. The difference in CS between premature and full term children was also noted in those with good VA (logMAR ⩽0).
Acknowledgments
We thank Elisabeth Berg, BSc, Department of Humanities, Informatics and Social Sciences, Karolinska Institutet, Stockholm, for her valuable advice about the statistical analyses and the Swedish National Board of Health and Social Welfare, for their help.
REFERENCES
Footnotes
-
The study was supported by Stiftelsen Synfrämjandets forskningsfond, Kronprinsessan Margarethas Arbetsnämnd för synskadade, Margit Thyselius fond and Stiftelsen Samariten.