Article Text

Abstract
Background: Unlike the immune privilege enjoyed by low-risk corneal grafts, high-risk corneal grafts experience rejection rates comparable to liver and kidney transplants. Systemic immunosuppression reduces the risk of rejection in high-risk corneal grafts.
Methods: Systemic tacrolimus, a specific T cell inhibitor, was used at a mean daily dose of 2.5 mg to immunosuppress 43 patients undergoing high-risk corneal transplantation. Immunosuppression was continued for a period of 18–24 months after the high-risk corneal graft.
Results: During a mean follow-up period of 33.7 months, clarity of the graft was maintained in 65% of patients. Eight patients experienced rejection episodes while on tacrolimus, and this led to graft failure in five patients.
Conclusion: Tacrolimus is relatively safe and effective in reducing rejection and prolonging graft survival in patients with high-risk keratoplasty compared with other series where similar immunosuppression was not used.
- HLA, human leucocyte antigen
- HSVK, herpes simplex virus keratitis
Statistics from Altmetric.com
Corneal transplantation is a commonly performed solid tissue transplantation procedure. Around 36 000 corneal transplants are performed annually in the US1 and around 2500 in the UK.2 Owing to its recognised immune-privileged status, topical corticosteroid treatment usually ensures survival of low-risk corneal grafts. Low-risk grafts have a good prognosis, with a rejection rate of approximately 13.5% within 2 years.3 However, in several conditions, the cornea loses its immune-privileged status, and its susceptibility to immunological rejection and failure is increased. In high-risk grafts, reported failure rates are between 60% and 90% depending on the criteria used to define high risk.4–7 Patients under high risk have been defined as having at least two quadrants of stromal vascularisation and/or a history of previous graft rejection.8 Other risk factors include herpes simplex virus keratitis (HSVK),9 chemical injury,10 large grafts11,12 and low recipient age.11
Several studies show enhanced graft survival in animal models of high-risk grafts using topical and systemic immunosuppression with ciclosporin and tacrolimus.13–18 Tacrolimus is a macrolide antibiotic isolated from the soil fungus Streptomyces tsukubaensis, with potent immunosuppressive activity. The mechanism of action of tacrolimus is similar to ciclosporin—that is, it binds to a specific cytosol protein and inhibits the T cell receptor-mediated signal transduction required for transcription of interleukin (IL)2 and other lymphokines. Tacrolimus has been used successfully in liver and renal transplantation.19 We have reported the benefit of tacrolimus in prevention of rejection in 11 patients with high-risk corneal graft.20 In that study, we compared the survival of high-risk grafts in patients treated with systemic tacrolimus with the survival of previous grafts in the same group of patients without tacrolimus and showed considerably improved graft survival with the use of tacrolimus.20 We now present our long-term results of the use of systemic tacrolimus for the prevention of rejection in 47 patients with high-risk corneal grafts.
METHODS
In all, 47 patients with 47 high-risk corneal grafts were prospectively enrolled over a period of 7 years. Any patient who had at least one previous graft failure in the same eye and/or two quadrants of stromal vascularisation was included. Patients who underwent simultaneous allolimbal transplant (n = 13) were excluded. All grafts were human leucocyte antigen (HLA) matched (no greater than a 1:1 mismatch of class I alleles). Table 1 summarises the clinical details. A system of risk scoring was devised on the basis of published risk factors for corneal rejection (table 2).20
Clinical details of patients
Preoperative risk scoring for patients undergoing high-risk corneal grafts
A total of 22 patients underwent preoperative fine needle diathermy occlusion of deep stromal vessels.21 All grafts were of 7 or 8 mm diameter except one, which was 10 mm.
TACROLIMUS TREATMENT SCHEDULE
Informed consent was obtained. Baseline evaluation included clinical history, blood pressure, full blood count, urea and electrolytes, and liver function tests. Oral tacrolimus was initiated at a dose of 2 mg/day (1 mg twice daily) on the day of surgery, and was adjusted to aim for a whole blood tacrolimus trough level between 1 and 12 μg/l determined by clinical signs. The levels were maintained at the lower end of the above range for grafts that did not show any signs of vascularisation or rejection, and at the middle of the range for those that did. Trough levels were measured 12 h after the last dose of tacrolimus and were not allowed to rise above 12 μg/l to avoid toxicity. The mean dose of tacrolimus was 2.5 mg/day per patient (range 2–8 mg/day). Additionally, topical steroids were used in all patients.
MONITORING
All patients were followed up at 1 week, 3 weeks and then every 6–8 weeks or earlier if clinically indicated. At each visit, tacrolimus trough levels and aforementioned baseline tests were monitored. Snellen visual acuity, corneal clarity, vascularisation, state of sutures and any clinical evidence of rejection were also documented.
DURATION OF TREATMENT
Systemic tacrolimus was continued for 18 months postoperatively or until suture removal, whichever came later. Patients with clear grafts in their only seeing eye were given the option of continuing tacrolimus indefinitely. In patients who experienced rejection episodes while taking tacrolimus, the drug was continued for a period of 1 year after the last rejection episode. When a graft rejected after discontinuing tacrolimus, the patients were counselled and those willing were given further treatment for 1 year. Patients who did not wish to restart tacrolimus were managed with steroids or topical ciclosporin. The time to rejection and the number of rejection episodes were documented for all relevant patients. The following were considered as end points of the study: graft failure, death, completion of follow-up and discontinuation of the drug because of side effects. The data were collected prospectively at each visit. The study was approved by the ethics committee of the Queen’s Medical Centre, Nottingham, UK, and was conducted in accordance with the tenets of the Helsinki Declaration of 1975.
RESULTS
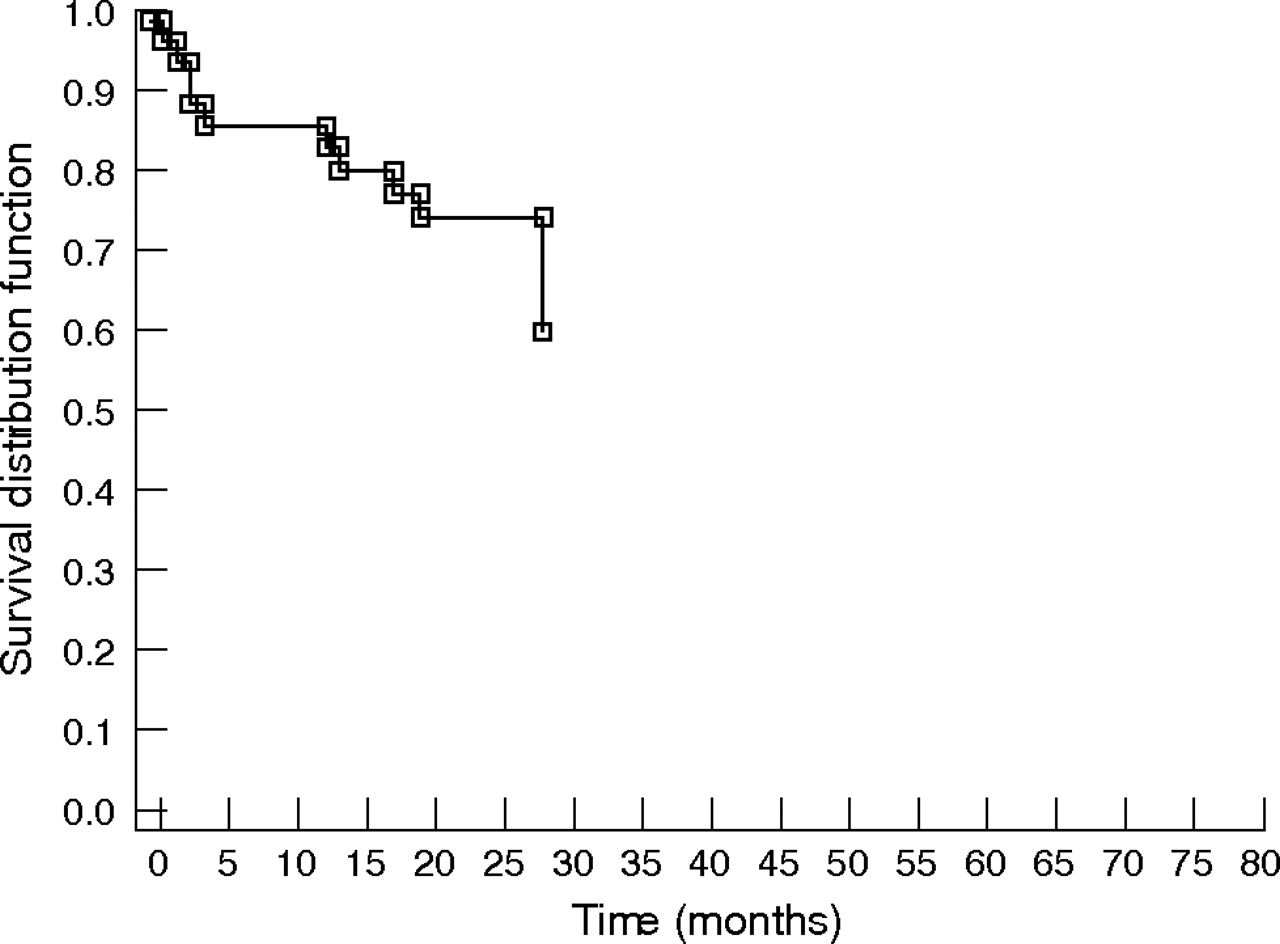
Four of the 47 high-risk patients discontinued tacrolimus within a mean of 4.2 months owing to side effects. These patients were excluded from the analysis of drug efficacy in preventing rejection. Four patients died at various stages of follow-up, with a mean time to death of 44 months. These were included in the analysis. The graft was clear in 28 of the 43 patients, till the last follow-up or death. The follow-up period ranged from 2 to 78 months (mean 33.7 months, median 30 months). The shortest follow-up was 2 months owing to failure of one of the grafts (one of the end points of the study) at 2 months (fig 1). Figure 2 shows the Kaplan–Meier survival of the grafts. Seven patients are continuing immunosuppression with tacrolimus. Four of these seven patients (including three who had high-risk grafts in their only eye) have elected to continue tacrolimus on a long-term (20–50 months) maintenance dose of 1 mg/day. The mean risk score for the entire cohort was 5, with a range 1–9.

Histogram showing duration of follow-up of 43 patients.

Kaplan–Meier curve showing survival distribution of all 43 corneal grafts irrespective of the cause of failure.
EFFICACY OF TACROLIMUS
Rejection on tacrolimus
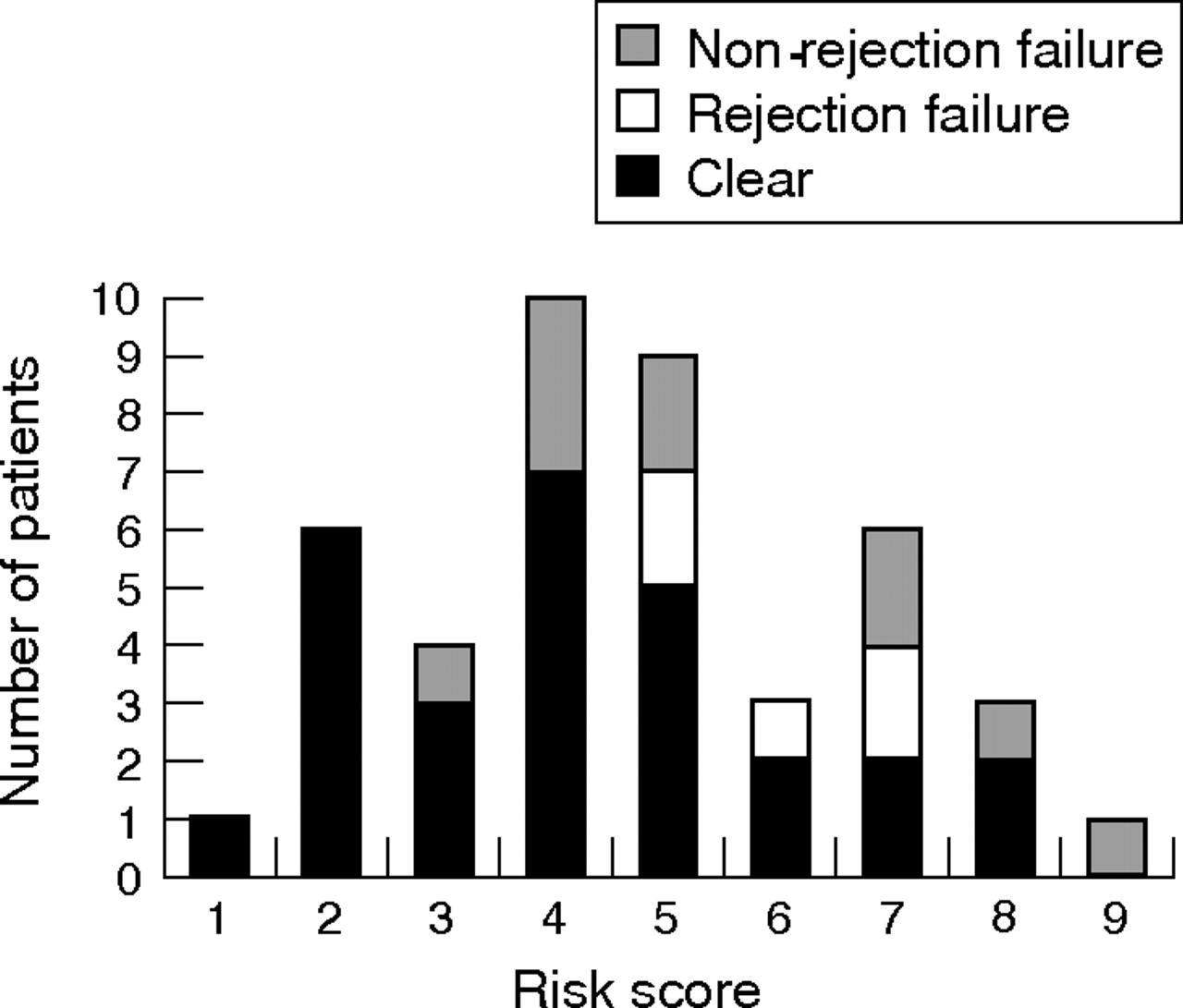
Of the 43 patients, 8 (18.6%) patients experienced episodes of rejection while taking tacrolimus, of whom three had multiple episodes. The rejection episodes were controlled with intensive topical and intravenous steroids in three of the eight patients (including two patients who had multiple rejection episodes), and the dose of tacrolimus was increased. All three patients have since successfully discontinued tacrolimus immunosuppression. The remaining five of these eight patients experienced irreversible rejection resulting in graft failure. No significant difference was seen in the trough levels between patients who showed rejection and those who did not. Figure 3 illustrates the distribution of the risk scores among the patients who experienced rejection failure (on and off tacrolimus), those who had non-rejection failure and those whose grafts remained clear. A significant correlation was observed between the risk score and rejection episodes (Pearson’s correlation coefficient, p = 0.007).
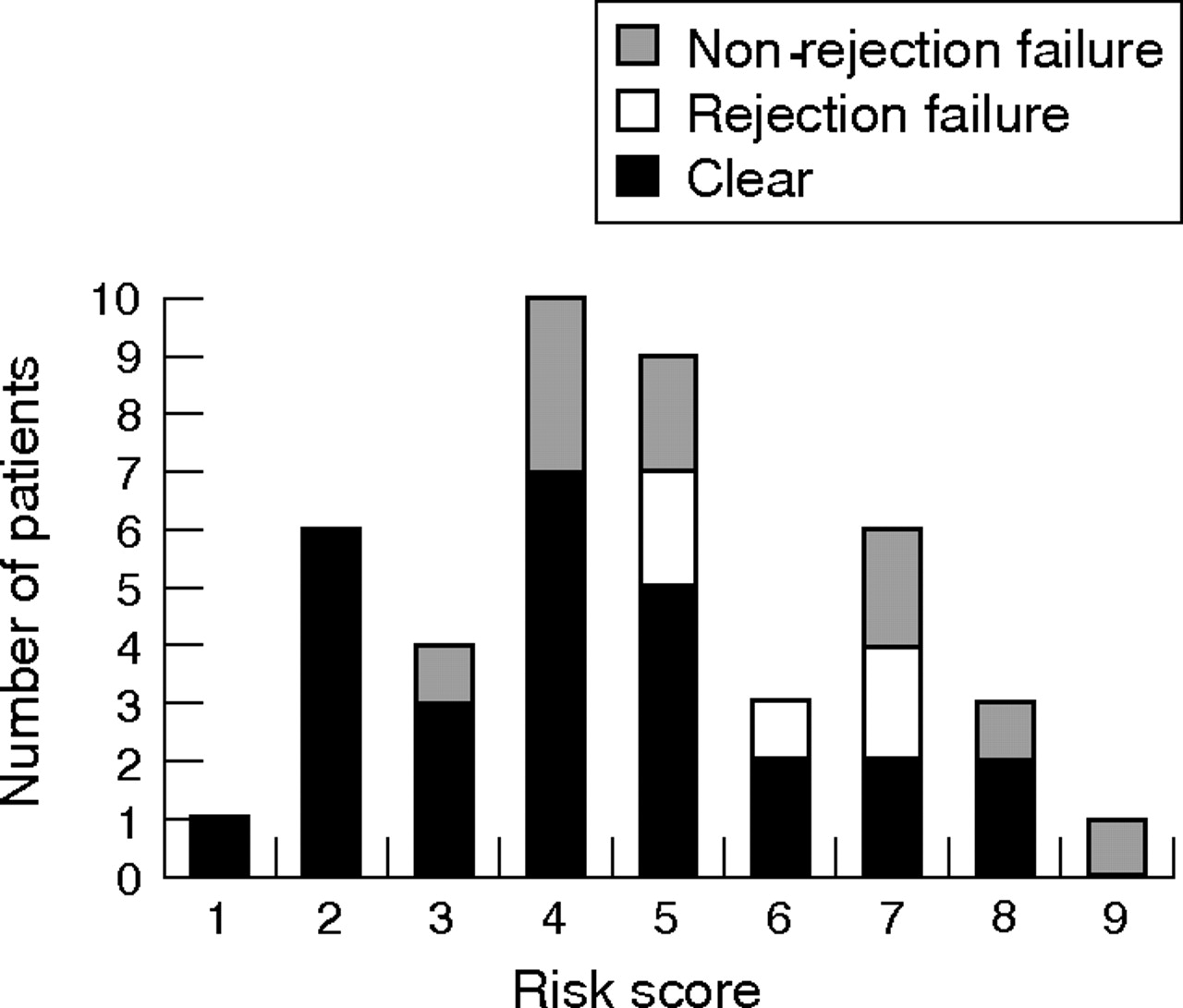
Risk score distribution in all 43 grafts.
Rejection off tacrolimus
A further 4 of the 43 (9.3%) patients experienced rejection episodes after discontinuing tacrolimus. The rejection episode was initially reversible in all four patients, of whom two elected to restart tacrolimus for 1 year. Both patients have since discontinued tacrolimus, with the graft remaining clear in one patient and a further rejection episode (5 months after discontinuing tacrolimus for the second time) resulting in graft failure in the other patient. Figure 4 shows the Kaplan–Meier curve for probability of rejection episodes.
Kaplan–Meier curve showing survival distribution to first episode of rejection excluding the non-rejection failures. No patient had graft rejection after 30 months.
Graft failure unrelated to rejection
Failure due to non-immune causes was seen in 9 of 43 (21%) patients. Raised intraocular pressure was the major factor responsible in five (11.6%) patients, stem cell failure in two (4.7%) patients and bacterial keratitis in the remaining two (4.7%) patients. The mean time to failure was 20 months (median 27.4 months).
At the end of the study, the postoperative best-corrected visual acuity in the operated eye was 6/9 or better in 17 patients, with most of the remaining patients showing visual improvement (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Preoperative and postoperative visual acuity in the 28 patients whose grafts were clear at the end of the study.
Two-year survival
Of the 43 patients, 39 were eligible to be included in the 2-year survival analysis. The grafts in the remaining four who were ineligible because of shorter follow-up period were, however, clear at the last follow-up. In all, 30 of the 39 (77%) eligible grafts were clear at 2 years; 6 (15.4%) failed grafts were not related to rejection and 3 (7.7%) failed grafts were due to rejection.
To summarise, 12 patients experienced rejection episodes during the period of the study. Clarity of the graft was maintained in 28 of 43 (65%) patients. Five patients experienced rejection-related graft failure while on tacrolimus and one had rejection-related graft failure off tacrolimus. Graft rejection correlated significantly with the preoperative risk score.
SIDE EFFECTS
The common side effect of tacrolimus was increased blood pressure or exacerbation of pre-existing hypertension in 10 patients, which was controlled with a low-dose angiotensin-converting enzyme inhibitor. Other side effects were headaches, malaise and gastrointestinal upset (n = 4 each), paraesthesia (n = 3), reversible increase in serum creatinine (n = 2), insomnia (n = 2), pancreatitis, folliculitis, diabetes, increased frequency of epileptic episodes and lymphopaenia (n = 1 each).
Four patients died in the follow-up period. The grafts were clear in three patients at the time of death. Poor compliance with glaucoma drugs owing to progressive dementia contributed to raised intraocular pressure and decompensation of the graft in the fourth patient (table 3).
Clinical details of patients who died during the study period
DISCUSSION
Primary low-risk corneal transplants have the highest success rate (>90%) and lowest rejection rate (11–18%) of all transplant surgery and do not routinely require systemic immunosuppression.22 The outcome is less satisfactory in high-risk corneal grafts, where the success rate is lower than that of first allografts of kidney, heart and liver (80–90%).23 Factors that are recognised to increase the risk of rejection in corneal transplants include vascularisation in the recipient cornea, large graft size,24 HLA-A and HLA-B incompatibility,25 previous failed corneal graft/s, decreasing age of recipient, glaucoma,24 peripheral anterior synechiae,26 chemical burn8 and HSVK.27 The risk of graft failure varies substantially even within a high-risk population.8 Our cohort of patients undergoing keratoplasty had one or more of the above risk factors. We devised a method of assigning a numerical value to each of the above risk factors to distinguish between patients at the higher and lower ends of the risk scale. This system showed a considerable correlation between risk score and rejection episodes in our study. Weisbrod et al28 reported a two-year survival rate of 63.9% for second grafts compared with 78.8% for primary grafts. The 2-year success rate in our high-risk patients was 77%. Rumelt et al29 followed up 28 re-grafts treated with oral ciclosporin for an average of 26.6 months and reported rejection-related failure in 32% and non-rejection-related failure in 36%. In comparison, rejection-related failure was seen in 7.7% and non-rejection-related failure in 15.4% of our patients at 24 months. Thus, at the 2-year point, use of systemic immunosuppression with tacrolimus confers a beneficial effect.
Corneal transplantation for HSVK is associated with increased risk of failure owing to rejection or recurrence of infection.27 HSVK was the underlying diagnosis in 13 of our patients. All 13 patients were concurrently treated with prophylactic oral aciclovir. None of these patients had a recurrence of HSVK in their graft. Preoperative glaucoma is also a strong risk factor for graft failure and can compound the risk.8,30 Every attempt was made to control the intraocular pressure both preoperatively and postoperatively. Nevertheless, raised intraocular pressure or hypotony after attempts to control the intraocular pressure was the main cause of graft failure in five patients.
Immunosuppression with topical steroids is currently the gold standard for all corneal grafts. The use of topical steroids is associated with increased intraocular pressure, cataracts or a recurrence of HSVK in susceptible patients. In high-risk grafts, topical steroids alone are not sufficient to prevent rejection and systemic immunosuppression is required.5,31,32 Other strategies to reduce the risk of rejection in high-risk grafts include HLA or ABO matching,8,33 occlusion of established corneal vessels21 and smaller graft size.
Corneal graft rejection is a T cell-mediated immune response.34,35 Several immunosuppressive drugs classed as T-cell inhibitors could be considered in the prevention and management of corneal graft rejection. All have a side effect profile that requires careful monitoring of dosage, efficacy and adverse events, for which collaboration with a clinical immunologist or rheumatologist is recommended. Over the years we have developed experience in the use of T cell inhibitors through such a collaboration.20,36,37 We have found tacrolimus to be effective and safe in the treatment of other immune-mediated diseases (uveitides) and therefore considered it an appropriate drug to use in patients with high-risk corneal transplant.
We found tacrolimus to be effective in reducing the risk of corneal graft rejection. However, eight of the 43 patients who continued to use tacrolimus experienced rejection episodes and five of these experienced rejection-related graft failure. These patients may have benefited from higher doses of tacrolimus or combination treatment with another immunosuppressive agent. The four patients who had rejection episodes after stopping tacrolimus may have required a longer duration of treatment with tacrolimus. In this study, we noted a higher risk score to be correlated with the occurrence of rejection and failure, suggesting that it is useful to risk-score patients and plan immunosuppressive strategies accordingly.
Interestingly, no patient who was followed for >30 months developed a rejection episode, suggesting that the risk of rejection in these high-risk patients is greatest in the first 30 months. This may offer some indication on the duration for which immunosuppression may be continued.
Use of systemic immunosuppression is associated with a risk of short-term and long-term side effects. The main side effect noted with tacrolimus was hypertension, which was controlled with drugs for hypertension. However, considerable side effects such as raised serum creatinine, pancreatitis and lymphopenia were also noted. Reduction of drug dose resulted in normalisation of creatinine and lymphocytes. Tacrolimus was stopped in the patient who developed acute pancreatitis. Patients who were unable to tolerate the required dose were given the option of switching to an immunosuppressive agent with a different side effect profile or using combination treatment. Topical ciclosporin was used in those patients who were unable to tolerate any systemic immunosuppression. However, the use of topical ciclosporin is limited by the local discomfort and epithelial toxicity associated with its use.38,39 Four of our patients died during the follow-up period. Three were over 88 years of age and only one patient was on tacrolimus at the time of death. Although it is impossible to be certain about the relationship between immunosuppressive treatment and cause of death in these patients, it is strong reason for exercising caution and close monitoring, use of standard protocols and multidisciplinary approach to management.
In conclusion, tacrolimus is relatively safe and effective in prolonging graft survival and may be considered in patients with high-risk keratoplasty. However, it has considerable side effects and appropriate caution should be exercised in its use. Proper patient selection and information is important before instituting treatment with tacrolimus.
REFERENCES
Footnotes
-
Published Online First 6 September 2006
-
Funding: This study was supported by Astellas Pharma, formerly known as Fujisawa Pharmaceuticals, in the form of a stipend paid to AJ during her time as clinical research fellow at the Queen’s Medical Centre, Nottingham.
-
Competing interests: None declared.