Article Text

Abstract
Purpose: To evaluate amniotic membrane (AM) tissue morphology and corneal epithelial healing in human eyes after amniotic membrane transplantation (AMT), using laser scanning in vivo confocal microscopy (IVCM).
Patients and methods: Twenty eyes of 20 patients, treated with single layer epithelial side up AMT for chemical burns in the acute stage (n = 8) and persistent corneal epithelial defect (n = 12) were studied by serial IVCM post-AMT until complete re-epithelisation. Changes in morphology of transplanted amniotic tissue and healing corneal epithelium were noted. AM and corneal epithelial cell density was calculated using image-analysis software.
Results: IVCM enabled visualisation of transplanted AM and of regenerating epithelial cells under the AM. The mean AM epithelial cell density, 1 day after transplant, was 4613 (SD 380) cells/mm2. The average AM epithelial thickness was 35 (4) μm, while the AM stromal thickness was 116 (31) μm. The amniotic stroma appeared to be composed of a superficial dense fibrous layer and a deeper loose reticular network of fibres. Amniotic epithelium was lost within 15 days of transplant, and complete re-epithelisation of the corneal surface was achieved between 1 and 4 weeks.
Conclusions: Laser scanning IVCM is a useful method for evaluating AM tissue morphology, degradation and corneal epithelial healing after AMT for different clinical indications. When the amniotic membrane acts as a patch, that is epithelial cells migrate under rather than over the membrane, the membrane disintegrates and is lost.
Statistics from Altmetric.com
The amniotic membrane (AM) has been used in the management of several ophthalmic conditions.1–3 It is composed of an avascular, hypocellular stroma and an overlying basement membrane with a single layer of epithelial cells.1 Its immunological inertness and its ability to promote epithelisation inhibit fibrosis, angiogenesis and inflammation,1 2 4–8 making it ideally suited for use in ocular surface reconstruction.9 Amniotic membrane transplantation (AMT) has been successfully used in patients with persistent corneal epithelial defects,9–12 chronic corneal ulcers11–13 and ocular surface burns.14 15 When used in the management of corneal epithelial defects in the presence of an intact limbus, complete re-epithelisation is readily achieved.16 It is thought that AMT promotes epithelisation through mechanisms such as providing a suitable substratum (basement membrane) for epithelial cell growth, preventing apoptosis and producing various growth factors capable of stimulating and supporting epithelial cells.1–3 9 When the AM is placed to cover the epithelial defect, it generally allows epithelisation to occur underneath it, thus acting as a patch and not a graft.2 The monitoring of corneal epithelial healing under the AM is difficult with slit-lamp biomicroscopy through the AM. With an AM in situ, the use of fluorescein dye17 may not be helpful, as it stains the overlying membrane and makes visualisation of underlying defects difficult. Laser scanning in vivo confocal microscopy (IVCM) affords a non-invasive option of obtaining images, not only of transparent corneal layers but also of non-transparent tissues of an ocular surface such as the limbus and conjunctiva.18 19 Recently, IVCM has been used to image the AM tissues and epithelial regeneration in rabbit corneas.20 We conducted a study to evaluate AM tissue morphology and epithelial healing in human eyes after AMT, using laser-scanning IVCM. To our knowledge, this is the first such study in humans.
PATIENTS AND METHODS
The study was an observational case series. The research adhered to the tenets of the Declaration of Helsinki, and the protocol used was approved by the Institutional Review Board. Twenty patients (20 eyes) requiring AMT (13 males and seven females aged between 41 and 70 years) who attended the Cornea and Ocular Surface Division of the Ophthalmic Clinic (University G. d’Annunzio—Chieti-Pescara, Italy) were enrolled. Each patient was informed about the nature of the study and signed an informed consent. A detailed clinical history was recorded. Eight patients (eight eyes, five left and three right) had ocular surface alkali burns presenting within 1 week of injury with corneal epithelial, limbal and conjunctival damage (Grades 3–4, Dua’s Classification),21 and 12 patients (12 eyes, six left and six right) presented with chronic persistent corneal epithelial defects (PED). Underlying causes for PED were chemical injury (3), exposure keratopathy (2), bullous keratopathy (3) and severe band keratopathy (4). PED were unresponsive to conventional treatment for at least 8 weeks before AMT (average 9.5 (SD 1.0) weeks).
Amniotic membrane transplantation
Cryopreserved amniotic membrane was obtained from either National “L’Aquila Eye Bank” or “Rome Eye Bank” (Italy). Human amniotic membrane was prepared and preserved by a previously described method with minor modifications.3 In brief, human placenta was obtained from elective cesarean deliveries, after donors were screened against HIV, hepatatis B and C viruses and syphilis. Under a lamellar flow hood, the placenta was cleared of blood clots with sterile saline solution, the AM was separated from the chorion by blunt dissection, and samples for microbiological tests to assess sterility were obtained. The amnion with epithelial side up was flattened onto a nitrocellulose paper and then stored in sterile phials containing RPMI Media (Sigma-Aldrich, St. Louis, MO) at −80°C. AMT was performed under peribulbar anaesthesia. The AM was placed as a single layer with the epithelial side up. In patients presenting in the acute stage of alkali burns surgery was performed two days and three days after injury in 5 and 3 patients, respectively. A total corneal and limbal cover with AM was achieved after 360° limbal peritomy, excision of ischaemic/necrotic conjunctiva and removal of the residual necrotic corneal epithelium. AM was secured with interrupted 8-0 Vicryl sutures with episcleral bites around the limbus. In patients with PED the loose epithelium at the edges of the defect was debrided prior to AMT. The membrane was sutured in place with interrupted or running 10-0 nylon sutures such that the edge of the surrounding intact epithelium was under the AM. At the end of surgery a therapeutic soft hydrophilic contact lens (PureVision® -balafilcon A- Bausch & Lomb, USA) was inserted. All patients received topical fluorometholone 0.1% and ofloxacin 0.3% four times daily until complete epithelialisation.
In vivo confocal microscopy
The central cornea or the area of the defect in each eye was examined with a digital corneal confocal laser-scanning microscope (HRT II Rostock Cornea Module, diode laser 670 nm, Heidelberg Engineering GmbH, Germany), on days 1, 3, 5 and 7 and on weeks 2, 3, 4, 6 and 8 post-AMT. Confocal examinations were performed in each case with bandage contact lens applied onto the cornea. The confocal laser scanning device is equipped with a water-immersion objective (Zeiss, Germany, 63×/N.A. 0,95 W) and allows for an automatic z-scan determination of depth of focus within the cornea enabling the collection and storage of high-contrast digital images 300×300 μm in size, of all corneal layers. The theoretical confocal section thickness is approximately 10 μm. This is the volume (voxel), which is imaged by the confocal microscope to form a two-dimensional pixel-based digital image. The lateral and transverse resolutions are 4 μm each.
IVCM was carried out under topical anaesthesia with 0.4% oxybuprocaine. Proper alignment and positioning of the head were maintained with the help of a dedicated movable target red fixation light for the contralateral eye. A digital camera mounted on a side arm provided a lateral view of the eye and objective lens to monitor the position of the objective lens on the surface of the eye. A drop of 0.2% polyacrylic gel served as coupling medium between the PMMA contact cap of the objective lens and cornea (contact lens).
Sequential images derived from automatic scans and manual frame acquisition throughout the area of interest were obtained with an emphasis on visualising AM and superficial corneal morphology. The “section mode” function of the instrument helped to search for AM tissues and corneal epithelium, enabling instantaneous imaging of a single area of the cornea at a desired depth.18 At least 30 images of the area of the cornea were obtained for each eye. AM and corneal epithelial cell density was calculated, at the first confocal examination at day 1 after surgery, using the analysis software of the instrument, by averaging numbers of cells from five images (randomly selected from the recorded images), counted manually within a region of interest (ROI) of standardised dimensions (250×250 μm). Cell densities are given as cells per square millimetre (cells/mm2).18
RESULTS
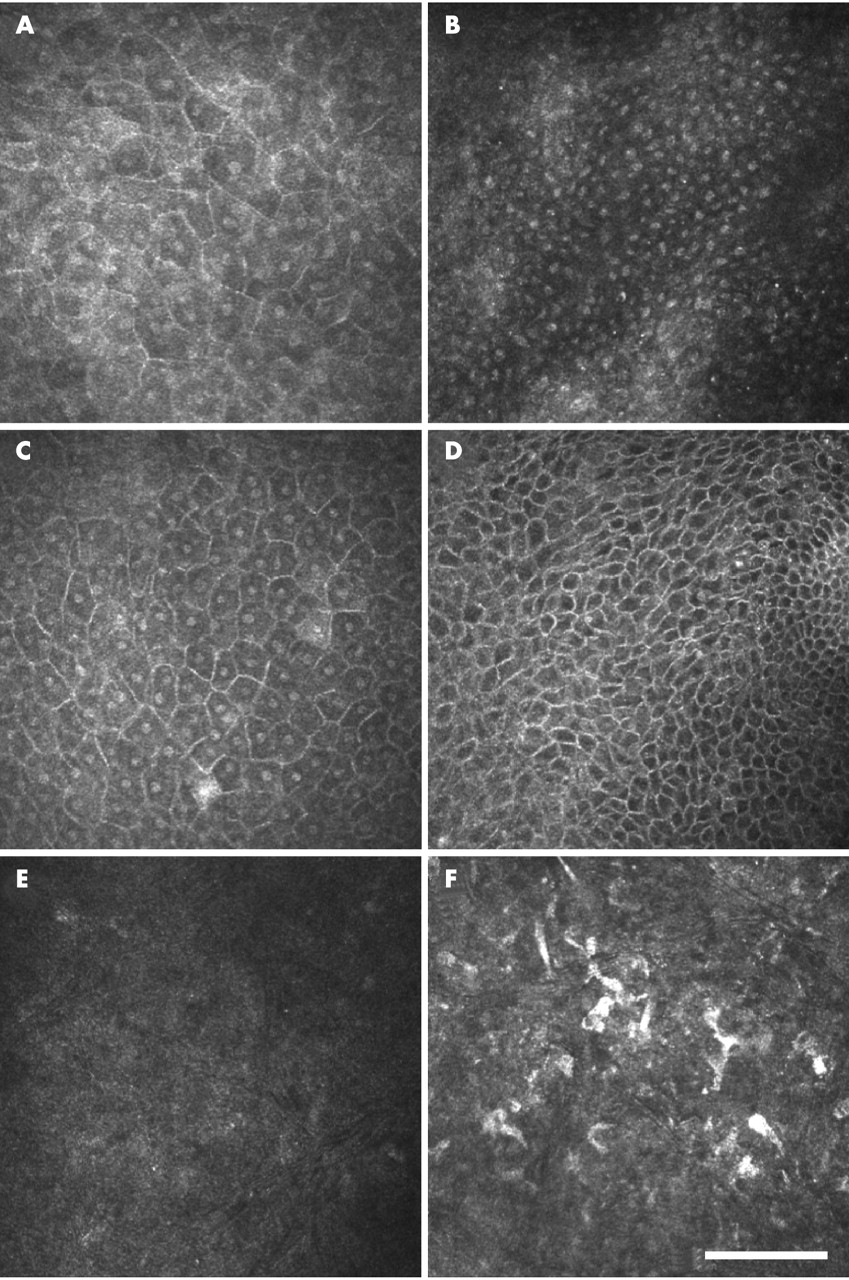
It was possible to visualise, by IVCM, AM tissue covering the corneal surface in all cases from day 1 after surgery. AM epithelium appeared as a single layer of polygonal cells with defined bright borders and a homogeneous cytoplasm that lacked nuclear details (fig 1A,B). Immediately beneath the amniotic epithelium was a thick acellular basement membrane with intermediate reflectivity and granular texture (fig 1C). Beneath the basement membrane, an almost acellular layer of intermediate to high-reflectivity was observed in all cases. This layer, representing the amniotic stroma, could be differentiated into two zones. A dense and reflective acellular superficial (fibrous layer) and a thicker and less reflective deeper layer with fibres organised in a reticular network, with rare cells interspersed, overlying the corneal stroma (fig 1D–F).

IVCM characteristics of AM and corneal epithelium are reported in table 1. The mean AM epithelial cell density was 4613 (SD 380) cells/mm2. Focal areas of missing epithelium were observed at day 1 in 75% of eyes (15/20) (fig 1B). The average AM epithelial thickness (including epithelium and basal membrane) was 35 (4) μm, while the AM stromal thickness showed a greater variability, being 116 (31) μm (range 75–155 μm). From day 3 after surgery, AM epithelium showed progressive signs of degradation (fig 2), becoming undetectable at day 15 in all eyes (table 2). AM basement membrane and stroma persisted longer (fig 3) and were microscopically visible up to 4 weeks in 60% and up to 6 weeks in the remaining 40% of the eyes studied. At 8 weeks, AM tissues were no longer detectable (table 2).


In all cases, complete corneal epithelisation was achieved within the follow-up period. Newly formed corneal epithelium under the AM tissues, in the corneal centre indicating central epithelisation (fig 4 and table 2), was observed by means of IVCM at day 7 in 15% of the eyes (3/20), at 2 weeks in 25% of the eyes (5/20), at 3 weeks in 40% of eyes (8/20) and at 1 month after surgery in the remaining 20% of eyes (4/20). No differences in epithelisation time related to the underlying diseases responsible for PED (ie, chemical injury, exposure keratopathy, bullous keratopathy and band keratopathy) were observed. The newly formed corneal epithelium was composed of large superficial flat epithelial cells and basal epithelial cells lying on a basement membrane (fig 4). At the time of epithelisation, the average central corneal epithelial thickness was 32±6 μm, the mean superficial epithelial cell density was 815 (SD 152) cells/mm2, the mean basal epithelial cell density was 2530 (288) cells/mm2, while the corresponding values increased to 55 (8) μm, 1180 (322) cells/mm2 and 4320 (412) cells/mm2, respectively, 4 weeks after completion of central epithelisation (p<0.001, Wilcoxon sign rank test), as shown in table 1.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The promotion of epithelisation is one of the main clinical benefits of AM transplantation on to the corneal surface.1–3 6–9 AM facilitates healing of the corneal epithelium not only in cases of PED where there is a chronic failure of epithelial healing but also in cases of acute epithelial defects such as in chemical burns. Chemical burn induced corneal epithelial defects with an intact or partially involved limbus respond better to amniotic membrane transplantation than those associated with total limbal deficiency.16 22 Of the different mechanisms proposed to explain the favourable action of AM, provision of an intact basement membrane substrate for the migrating cells would apply only when the membrane is used as a graft, and re-epithelisation occurs on the AM.1–3 8 9 When used as a patch, as in this study, any new epithelial sheet forming under the membrane would synthesise its own basement membrane while remaining protected by the membrane and possibly supported by its growth factors. When AM is transplanted on to the ocular surface and acts as a patch with epithelium growing beneath it, the amniotic tissues are known to undergo progressive degradation.23 When AM acts as a graft with epithelium growing on it, amnion tissues persist and integrate with the superficial corneal stroma.24 25
A previous study20 performed on rabbit eyes reported that both white-light and laser IVCM can be used to observe the structural features of AM patches (AMP) and the healing corneal epithelial under the AMP. One of the main limitations in the clinical follow-up of AMT is that the observation of corneal re-epithelisation, occurring under the AM patches, may be difficult due to the limited transparency of the AM tissues. The use of fluorescein staining has been proposed to detect corneal epithelial defects through AMP17 but fluorescein easily stains the transplanted amnion and makes delineation of any underlying corneal epithelial defect difficult. Furthermore, fluorescein staining does not permit a morphological examination of the corneal epithelium and also does not provide information on changes occurring in the different layers of the AM in situ. Laser-scanning IVCM has been shown to be a useful tool in the morphological analysis of non-transparent structures of the ocular surface such as the limbus and conjunctiva18 19 26–28 and hence was preferred over white-light confocal microscopy for the evaluation of transplanted AM tissues and corneal epithelial healing in the present study.
In our first study in humans, IVCM allowed the visualisation of the microscopic architecture of the AM tissues covering the corneal surface, showing progressive changes of AM morphology over time. The microscopically observed AM layers were: (i) epithelium, (ii) basement membrane, and (iii) stroma. These in vivo observations are in agreement with the microscopic morphology of AM previously described by ex vivo histology,1–3 and provide new insight regarding in vivo AM tissue alterations following transplantation. The amniotic epithelium appeared as a mosaic of cuboidal/polygonal single-layered cells with a high average cell density (4613 (SD 380) cells/mm2), similar to the basal layer of the corneal epithelium. The AM epithelium appeared focally damaged, with areas of missing amniotic epithelial cells in 75% of cases. It has been shown that cryopreservation significantly impairs the viability of AM epithelial cells, even though cell morphology is retained.29 The AM used in this study was cryopreserved, and AM epithelium was identified 1 day after surgery, although focal areas of loss of epithelial continuity were present in the majority of cases. Our findings confirm that in vivo, after AMT an AM epithelial layer of presumably nonviable cells is retained. IVCM showed that the AM epithelial layer underwent progressive degradation over a 2-week period after transplantation. These observations conform to the hypothesis that the favourable effects of AMT observed over time, cannot be entirely attributed to the AM epithelium,1 29 and that the amniotic basement membrane usually survives the processing and storage procedures.
The amniotic basement membrane was indeed microscopically identified in our study, and appeared as an acellular homogeneous structure of mid- to high-reflectivity, which persisted longer than AM epithelium, up to 6 weeks after grafting in the majority of cases, by which time corneal epithelisation was achieved in all patients. Similarly, the AM stroma was observed microscopically in vivo after surgery and could be differentiated in two different sublayers by morphology: a superficial layer with dense and almost continuous high reflectivity, and a deeper one, containing evident extracellular fibres interspersed in a low reflective matrix, arranged in a network pattern. Presumably, these two distinct layers identified in the AM stroma by IVCM represent the compact layer (a dense tissue devoid of cells) and the fibroblast-spongy layer (loose network of reticulum with embedded fibroblasts) respectively.1 IVCM showed that the spongy layer was in direct contact with the denuded corneal stroma and progressively degraded over the 4–6-week period during which corneal re-epithelisation occurred under the AM stroma.
Notably in this study, corneal epithelisation was achieved in all patients and was found to occur under the low reflective stromal sublayer of the AM. This observation indicates that when the AMT surgery is performed as described in this case series, with the edge of the AM patch extending beyond the area of defect, it is ensured that the regenerating epithelium will migrate under the AM which then will serve as a patch and not a graft.2 16 24 Moreover, IVCM also showed that newly formed corneal epithelial cells can synthesise their own basal membrane allowing them to anchor to the underlying stroma. The type of corneal epithelisation under the amniotic patch and the persistence for a variable period of time of the patch on the corneal surface observed in this study, even when epithelisation was achieved, corresponds to the “disintegration pattern” of the AM proposed by Resch et al25 in their recent ultrastructural observations on amniotic membrane integration patterns. The favourable effects of AMT on corneal epithelisation may also be attributed to the suppression of inflammation in the acute phase of severe ocular burns.30
This study also demonstrated that the morphological and microscopic evaluation of healing epithelium under the AM is possible by IVCM. Complete healing occurred while the AM basement membrane and stromal layers were still present on the corneal surface. This was similar to the observations described using IVCM in rabbits.20 Progressive maturation of the newly regenerated corneal epithelium as evidenced by the initial presence of a thin epithelial layer composed of superficial and basal epithelial cells with reduced cell density and increased cell size changing into a thicker epithelium with increased cell density and reduced cell size by 1 month was observed by IVCM.
Continued application and experience gained by the use of bsf/IVCM are increasingly establishing its role as a useful clinical tool in the evaluation of the ocular surface.
REFERENCES
Footnotes
Competing interests: None.
Linked Articles
- At a glance