Article Text

Abstract
Background/aims: The aim of this study was to compare the morphological and visual acuity outcomes associated with a single intravitreal injection of triamcinolone acetonide versus bevacizumab for the treatment of refractory diffuse diabetic macular oedema.
Methods: Twenty-eight patients were randomly assigned to receive a single intravitreal injection of either 4 mg/0.1 ml triamcinolone acetonide or 1.5 mg/0.06 ml bevacizumab. Comprehensive ophthalmic evaluation was performed at baseline and at weeks 1, 4, 8 (±1), 12 (±2) and 24 (±2) after treatment. Main outcome measures included central macular thickness measured with optical coherence tomography (OCT) and best corrected Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity.
Results: Twenty-six patients (26 eyes) completed all study visits (two patients missed two consecutive study visits). Central macular thickness was significantly reduced in the intravitreal triamcinolone group compared with the bevacizumab group at weeks 4, 8, 12 and 24 (p<0.05). Logarithm of the minimum angle of resolution (LogMAR) best-corrected visual acuity was significantly higher at weeks 8 (0.69; ∼20/100+1) and 12 (0.74; 20/100−2) in the intravitreal triamcinolone group compared with the bevacizumab group (weeks 8 (0.83; ∼20/125−1) and 12 (0.86; 20/160+2)) (p<0.05). Significant change from baseline in mean intraocular pressure (mmHg) was seen at week 4 (+2.25) only in the intravitreal triamcinolone group (p<0.0001). No patient had observed cataract progression during the study.
Conclusions: One single intravitreal injection of triamcinolone may offer certain advantages over bevacizumab in the short-term management of refractory diabetic macular oedema, specifically with regard to changes in central macular thickness. The actual clinical relevance of our preliminary findings, however, remains to be determined in future larger studies.
Statistics from Altmetric.com
Macular oedema is the most common cause of visual impairment in patients with diabetic retinopathy.1 Based on observations of the Early Treatment Diabetic Retinopathy Study (ETDRS) Group, diabetic macular oedema (DMO) is classified as “clinically significant” if well-defined specific clinical features (described elsewhere2) were seen associated with retinal thickening at or within 1 disc diameter of the centre of the macula or definitive hard exudates in this region. For this subgroup of patients, focal/grid laser photocoagulation is associated with a 50% reduction in moderate vision loss.2 However, the infrequently observed visual acuity improvement as well as the frequent recurrence or persistence of DMO after appropriate laser treatment, particularly in eyes presenting with angiographically diffuse macular oedema,2 3 has led investigators to seek alternative treatments for the management of DMO.
Amongst treatments currently under investigation for DMO, intravitreal injection of triamcinolone acetonide4–11 and of anti-angiogenic agents, such as bevacizumab,12 13 pegaptanib14 and ranibizumab,15 have been reported to be associated with short-term favourable anatomic and visual results in at least some patients with DMO.6–15 In the view of these promising preliminary results, we conducted a randomised, prospective study to compare the morphological and visual acuity outcomes associated with a single intravitreal injection of triamcinolone acetonide versus bevacizumab in the management of refractory diffuse DMO.
METHODS
The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the local Institutional Review Board. All participants gave written informed consent before entering into the study. All patients evaluated at the Retina Section of the Department of Ophthalmology, School of Medicine of Ribeirão Preto, Brazil, with a diagnosis of refractory DMO in at least one eye between April 2006 and September 2006 were invited to participate in the study. Throughout the study, measurements of best-corrected ETDRS visual acuity (BCVA) as well as central macular thickness (CMT) measured using third-generation optical coherence tomography (OCT) were performed prior to other study procedures by masked certified examiners. Ophthalmic evaluation, fundus photography and fluorescein angiography were performed by two retina specialists (L Paccola and M S Folgosa), who were aware of treatment assignment. Study data were collected, interpreted and analysed by two other masked investigators (R A Costa and J C Barbarosa).
Patient eligibility and baseline evaluation
Patients were included if they had: (1) refractory DMO (defined herein as the presence of “clinically significant macular oedema” (as per ETDRS criteria)2 by biomicroscopic evaluation, which had persisted despite at least one session of macular laser photocoagulation performed at least 3 months earlier) and diffuse fluorescein leakage involving the foveal centre and most of the macular area on fluorescein angiography; (2) logarithm of minimum angle of resolution (LogMAR) ETDRS BCVA (Snellen equivalent) of 0.3 (20/40) or worse; and (3) CMT greater than 300 µm on OCT. Exclusion criteria were: (1) aphakic or pseudophakic eyes; (2) glycosylated haemoglobin (HbA1c) level above 10%; (3) history of glaucoma or ocular hypertension (defined as an intraocular pressure higher than 22 mmHg); (4) an ocular condition (other than diabetes) that, in the opinion of the investigator, might affect macular oedema or alter visual acuity during the course of the study (e.g. retinal vein occlusion, uveitis or other ocular inflammatory disease, neovascular glaucoma, Irvine–Gass Syndrome, etc.); (5) systemic corticosteroid therapy; (6) history of thromboembolic event (including myocardial infarction or cerebral vascular accident); (7) major surgery within the prior 6 months or planned within the next 28 days; (8) uncontrolled hypertension (according to guidelines of the seventh report of the joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-7))16; (9) known coagulation abnormalities or current use of anticoagulative medication other than aspirin; or (10) any condition affecting follow-up or documentation.
Each patient received a detailed ophthalmologic examination including measurement of BCVA according to a standardised refraction protocol using a retroilluminated Lighthouse for the Blind distance visual acuity test chart (using modified ETDRS charts 1, 2 and R), as well as applanation tonometry, undilated and dilated slit-lamp biomicroscopic examination (including grading of lens opacity using the Lens Opacities Classification System III),17 indirect fundus examination, colour fundus photography and fluorescein angiography. Third generation OCT evaluation (Stratus Tomographer, Model 3000, Carl Zeiss Ophthalmic Systems Inc., Humphrey Division, Dublin, CA, USA) was also performed in all patients. It consisted of six linear 6.00 mm scans orientated at intervals of 30° and centred on the foveal region. In order to optimise accuracy of OCT data, automatic delineation of the inner and outer boundaries of the neurosensory retina generated by OCT built-in software was verified for each of the six scans using the “retinal thickness (single eye)” analyses protocol.18 19 For this study, CMT values (defined as the average thickness of a central macular region 1000 μm in diameter centred on the patient’s foveola) automatically generated by built-in OCT3 software using “retinal thickness (both eyes)” analysis protocol was used. The good reproducibility of these measurements using this method and the feasibility of the method for monitoring macular morphological changes in diabetic eyes have been described elsewhere.9 20 21
Twenty-eight patients with refractory diffuse DMO in at least one eye based on clinical examination and fluorescein angiography were identified. If both eyes were eligible for treatment, the eye with worse visual acuity was included. Twenty-six of the 28 patients were ultimately included in the analyses (two patients missed two consecutive study visits and were excluded from analyses).
Treatment assignment
Each patient was randomly assigned to receive one intravitreal injection of either 4 mg/0.1 ml triamcinolone acetonide or 1.5 mg/0.06 ml bevacizumab within 1 week of baseline. Patients assigned to intravitreal triamcinolone constituted the “ITA” group and those assigned to intravitreal bevacizumab constituted the “IBe” group.
For ITA, 4 mg preservative-free triamcinolone acetonide (Triancinolona 40 mg/ml; Ophthalmos, São Paulo, Brazil) was used, and for IBe 0.06 ml (1.5 mg) bevacizumab (Avastin 100 mg/4 ml; Genentech Inc., South San Francisco, CA, USA) was injected into the vitreous cavity. All treatments in both groups were performed by the same retinal specialist (R Jorge) using topical anaesthesia under appropriate sterile conditions; 0.3% ciprofloxacin four times daily was used post-injection for 1 week.
Follow-up examinations and outcome measures
Patients were scheduled for follow-up examinations at weeks 1, 4, 8 (±1), 12 (±2) and 24 (±2) after injection. At these visits, the patients’ BCVA was determined and they underwent complete ophthalmic examination using the same procedures as at baseline with the exception of fluorescein angiography, which was performed only at the final (week 24) follow-up visit.
Primary outcome measures used to compare the short-term effects of ITA with IBe were: (1) anatomical effects (that is, changes in CMT) on OCT; and (2) changes in BCVA from baseline. Secondary outcomes included the presence of local (such as changes in intraocular pressure (IOP) and cataract progression) and systemic adverse events, which were monitored throughout the study.
Statistical analysis
To study the effect of both treatments at the various study follow-up visits, an analysis of variance was employed, with a split-plot design, considering the group factor as the main effect (group ITA and group IBe), and the six study visits (including baseline) as the sub-plot factor. Tukey’s test was used for multiple comparisons at 5% level of significance (p<0.05).
RESULTS
Between April 2006 and April 2007, 26 patients completed the 24-week study period (fig 1). Twenty-one eyes (n = 10, ITA group; n = 11, IBe group) had proliferative diabetic retinopathy treated by panretinal photocoagulation at least 6 months before initial evaluation. Baseline characteristics by group are summarised in table 1. There were no significant differences between the two treatment groups with regard to patient age, sex or baseline characteristics, such as diabetic retinopathy level and number of previous laser surgeries for DMO. Ten patients had refractory diffuse DMO in both eyes: the eye with worse visual acuity was selected for the study.
Outcome measures
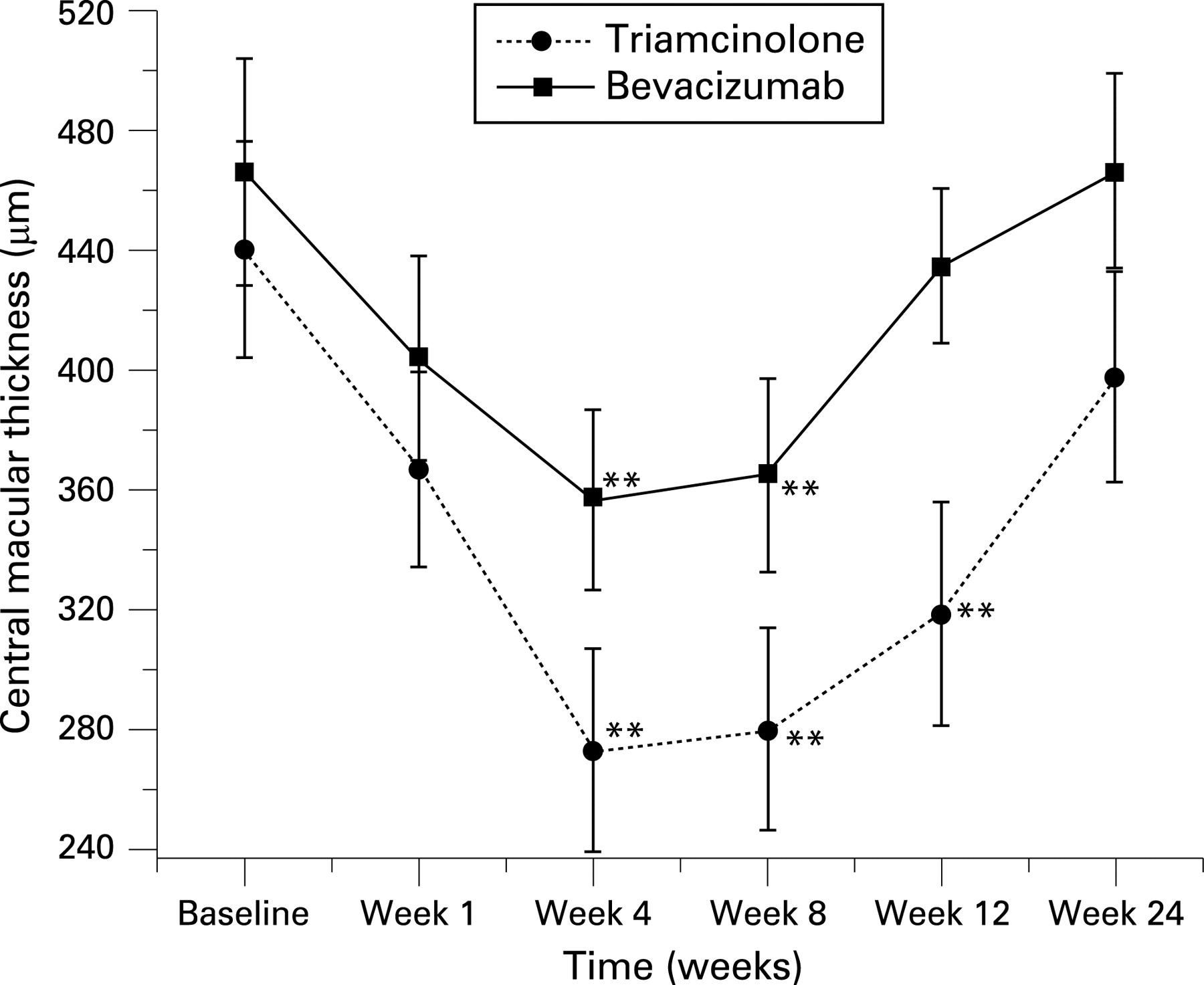
Analysis of variance showed significant interaction between groups and study visits with regard to CMT measurements (F = 2.61; p = 0.028). Figure 1 shows a significant reduction (p<0.01) in CMT in the ITA group at weeks 4 (p = 0.008), 8 (p = 0.006), 12 (p<0.0001) and 24 (p = 0.024) compared with the IBe group. Separate within-group analysis showed significant changes (reductions) in CMT values from baseline at weeks 4, 8 and 12 (p<0.0001) in the ITA group, and at weeks 4 (p<0.0001) and 8 (p = 0.0004) in the IBe group (fig 1; table 2).
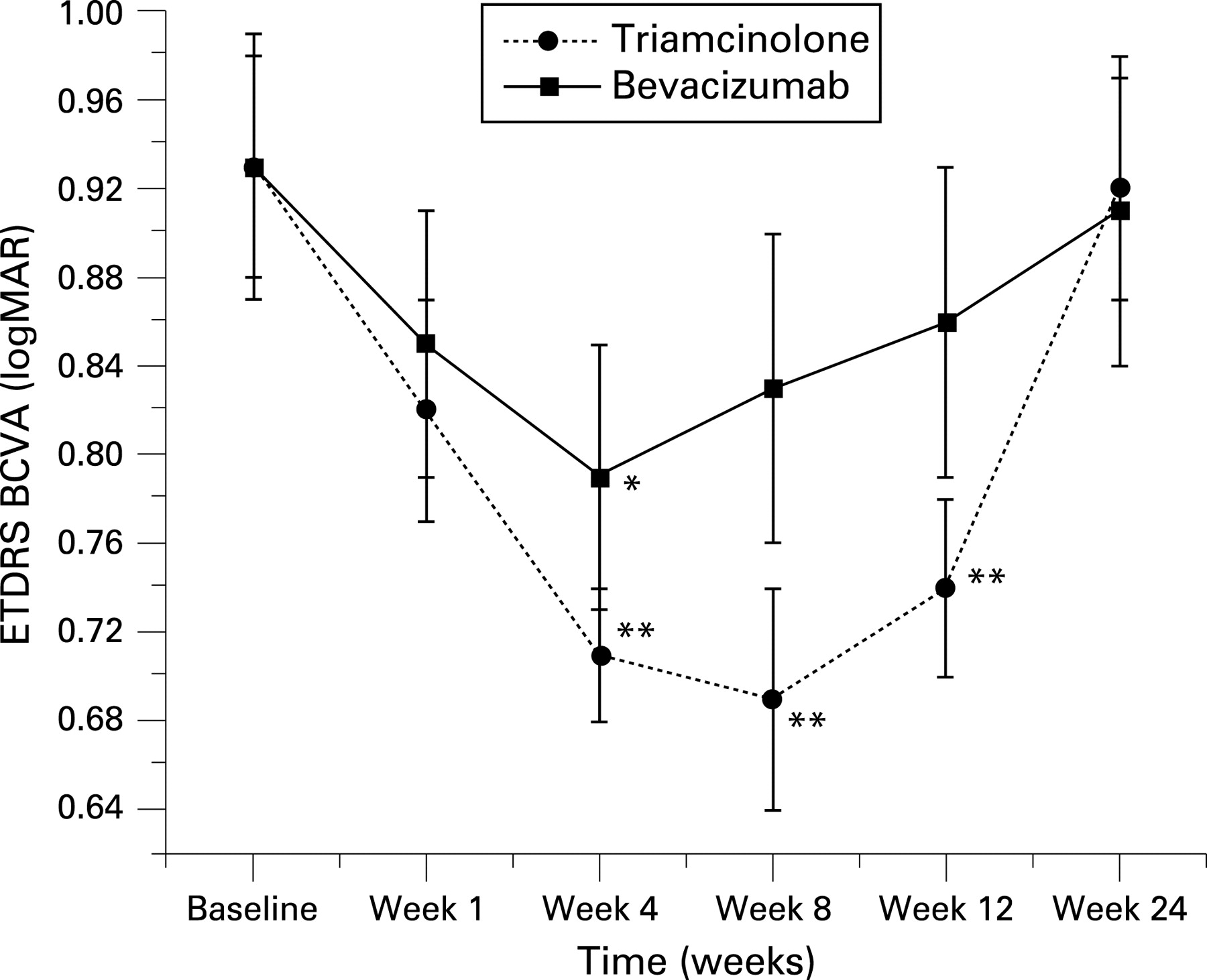
Significant interactions between groups and study visits were also observed for BCVA (F = 2.76, p = 0.022). Figure 2 shows significant improvement in BCVA in the ITA group compared with the IBe group at weeks 8 (p = 0.026) and 12 (p = 0.039). Separate within-group analysis showed significant improvement in BCVA from baseline at weeks 4, 8 and 12 (p<0.001) in the ITA group, and at week 4 (p = 0.011) in the IBe group (fig 2; table 2).
Significant interactions between groups and study visits were observed for IOP values using two-way analysis of variance (F = 3.46, p = 0.006). There was a significant increase in IOP in the ITA group compared with the IBe group at weeks 1 (p<0.0001), 4 (p<0.0001) and 12 (p = 0.043) (fig 3; table 2). Separate within-group analysis revealed a significant increase in IOP from baseline in the ITA group at week 4 (p<0.0001); in the IBe group no significant change in IOP was observed at any study visit. During the 24-week study period, no cataract progression was observed in either the ITA or IBe group. No severe adverse event was observed throughout the study. No systemic or serious drug-related adverse events were observed. Both treatment procedures were well tolerated, and no clinical evidence of inflammation, uveitis, endophthalmitis or ocular toxicity was observed.

{kind=link}
{kind=link}
{kind=link}
DISCUSSION
As far as we are aware, and based on Medline searches, this study is the first prospective, randomised trial to compare intravitreal triamcinolone with bevacizumab for the treatment of patients with refractory DMO. In this trial, a single intravitreal injection of triamcinolone acetonide was associated with a greater reduction in CMT in patients with refractory diffuse DMO compared with one intravitreal injection of bevacizumab in the short-term. Comparatively, more favourable anatomic effects were observed with intravitreal triamcinolone compared with bevacizumab as soon as 4 weeks after treatment, and persisted up to week 24. Although somewhat more favourable CMT changes were observed in patients treated with intravitreal triamcinolone than bevacizumab throughout the study period, the changes in vision were significantly different between the groups only at weeks 8 and 12. Therefore, the overall results of the current study suggest that one intravitreal injection of triamcinolone may be associated with greater beneficial effects on vision and macular remodelling than a single intravitreal injection of bevacizumab for the short-term management of refractory diffuse DMO.
Changes in CMT observed in the ITA group in the current study are consistent with those reported previously by our group in patients with refractory DMO10; mean CMT reduction of 59% (182.93 μm) at 4 weeks10 versus 38% (168 μm) in the current study, 30% (136.72 μm) at 12 weeks10 versus 27% (121.92 μm) in the current study, and 12% (55.07 μm) at 24 weeks10 versus 9.5% (42.25 μm) in the current study. Audren et al5 reported 51% (289 μm), 52% (293 μm) and 20% (115.8 μm) reductions in mean macular thickness by 1, 3 and 6 months of follow-up, respectively, after 4 mg intravitreal TA injection for refractory diffuse DMO. Using the same intravitreal dosage of triamcinolone, Massin et al8 also demonstrated short-term significant reduction in CMT. In the latter study, macular oedema recurred and retinal thickness reduction was no longer significant 24 weeks after injection, similar to the findings in the present study (fig 1).
Intravitreal bevacizumab was first reported as a treatment for macular oedema related to central retinal vein occlusion.22 Since then, there have been other reports of short-term beneficial effect of anti-vascular endothelial growth factor (VEGF) agents in reducing CMT and oedema secondary to retinal vascular disease, including diabetic retinopathy.12–15 23 24 More recently, Haritoglu et al reported significant macular thickness reduction 2 (15%), 6 (17%) and 12 weeks (25%) after repeated intravitreal bevacizumab injections.12 We observed significant improvement in CMT at 4 (23%) and 8 (21%) weeks after a single injection of 1.5 mg IBe.
Beneficial effects of intravitreal injection of TA compared with bevacizumab with regard to change in visual acuity were noted 8 and 12 weeks after injection. In the ITA group, visual acuity improvements from baseline were noted at weeks 4 (logMAR 0.22), 8 (logMAR 0.24) and 12 (logMAR 0.19). Similarly, previous reports have shown significant visual acuity improvements at the same study points after ITA injection,6 9 10 whereas Massin et al reported only a trend towards improvement in visual acuity 3 months after intravitreal injection.8 Regarding IBe injection, we verified significant improvement in mean visual acuity 4 weeks (logMAR 0.14, ∼7 EDTRS letters) after IBe compared with baseline values. Haritoglu et al12 reported a similar significant increase in visual acuity (logMAR 0.11, ∼6 EDTRS letters) 6 weeks after treatment, when 70% of the patients had received at least two injection of 1.25 mg IBe. On the other hand, a retrospective series by Arevalo et al13 showed that 55.1% of patients improved ⩾2 ETDRS lines (10 ETDRS letters) after 6 months of follow-up. However, this study did not include patients with refractory DMO and IBe was used as a primary treatment. In addition, the retrospective nature of the study and lack of standardisation regarding the number of injections and anti-VEGF drug dosage make a comparison of the 6-month results difficult.
The risk of IOP elevation associated with ITA has been reported in previous studies.6 9 In our study, there was a significant IOP increase from baseline observed at 4 weeks after the procedure in the ITA group. In addition, IOP in the ITA group was significantly elevated at weeks 4 and 8 in comparison with IBE group. Since baseline IOP values in both groups were similar (p = 0.56), it is important to point out that ITA has a higher risk of short-term elevation of IOP than IBe. Additionally, the incidence of cataract progression and glaucoma may well increase with longer follow-up and additional ITA treatments,6 and surgery for steroid-induced cataract may worse DMO and make its management more complicated.25 For this reason, IBe is an attractive treatment option for steroid-responders26 and phakic patients. For these patients, we hypothesise that repeated IBe injections using a dosage higher than that used in the current study may be a reasonable alternative therapeutic option,13 23 as it may be associated with better VA and CMT outcomes without the adverse events of glaucoma and cataract progression. Additional injection-related complications reported in other studies, such as conjunctival ulceration, retinal detachment, infectious or non-infectious endophthalmitis,14 27–29 were not observed in the current study.
In conclusion, a single intravitreal injection of 4 mg TA appears to offer certain short-term advantages over IBe for the management of patients with refractory DMO, particularly with regard to CMT as measured by OCT. However, the visual results are grossly comparable, and the well-known toxicities of TA must be considered. Moreover, limitations inherent in the study’s design, such as small sample size and limited length of follow-up, preclude extrapolation of our results. Finally, the potential benefits of TA or IBe, if any, over additional laser therapy for the management of refractory diffuse DMO remains to be determined, particularly in the long-term.
REFERENCES
Footnotes
Funding: Supported in part by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), grant no. 302940/2005-7; Fundação de Amparo è Pesquisa do Estado de São Paulo (FAPESP), grant no. 2006/55080-5.
Competing interests: None.
Linked Articles
- At a glance