Article Text

Abstract
AIM/BACKGROUND The most common choice of treatment for choroidal haemangiomas (CH) in the past has been the employment of scatter photocoagulation of the surface. This management often requires repetitive treatment or additional invasive management due to massive exudative detachment of the retina. The aim of this retrospective study was to investigate the outcome of the alternative application of low dose external beam irradiation with high energetic photons on these tumours.
METHODS A total absorbed dose of 20 Gy was applied to a total of 51 symptomatic eyes: 36 with a circumscribed CH of the posterior pole and 15 with diffuse CH as part of the Sturge–Weber syndrome. The indication for treatment was an exudative retinal detachment including or threatening the fovea. The mean follow up times in each group were 4.5 and 5.3 years, respectively. Out of a group of 33 patients from whom reliable data could be derived, 17 had symptoms lasting longer than 6 months.
RESULTS In 23 cases (63.8%) with circumscribed CH complete resolution of the subretinal fluid was achieved; the remaining 13 cases (36.2%) showed residual serous detachment distant to the fovea. The visual acuity improved by two or more lines in 14 cases (38.9%), remained stable in 14 cases (38.9%), and decreased in eight cases (22.2%). The functional success was dependent on the lag duration between onset of first subjective symptoms and treatment. The morphological results with diffuse CH were similar to those of the group of circumscribed CH. The visual acuity (VA) at last examination was improved in seven cases (46.6%); in the remaining eight cases, VA was unchanged or had deteriorated. The poor functional outcome in the latter was mainly attributable to secondary glaucoma.
CONCLUSION External beam irradiation is a useful and a low invasive therapeutic option for CH. A successful functional outcome is dependent on the time delay between first onset of symptoms and the beginning of therapy, the formation of subretinal fibrosis, and also on secondary glaucoma in the case of Sturge–Weber syndrome.
- choroidal haemangioma
- radiotherapy
- external beam irradiation
- Sturge–Weber syndrome.
Statistics from Altmetric.com
Haemangiomas of the choroid are rare vascular hamartomas that can occur in two forms: circumscribed choroidal haemangiomas (CH), which are solitary and predominantly located at the posterior pole, and diffuse CH, which are usually part of the Sturge–Weber syndrome. Histological examination of these tumours shows a vascular pattern, dominated by cavernous portions, but capillary tumours and mixed patterns are also observed.1 2
The CH is probably a congenital tumour that can eventually become symptomatic. Little is known about the natural course of these tumours. In a clinicopathological report, progressive enlargement in a case of circumscribed CH was well documented and mainly explained by venous congestion rather than by true enlargement of the tumour itself.3 In our own institution clinical observations were made on a group of 17 patients refusing treatment for circumscribed CH with a mean follow up of 7.5 years (unpublished data). None of these tumours showed any increase in tumour height on echography or significant enlargement of the base as measured by computer guided image analysis. However, 60% of these cases showed an increase of subretinal exudation.
Decrease of visual function can be caused by exudative retinal detachment, particularly when the macula is involved, and by secondary fibrous metaplasia or atrophy of the retinal pigment epithelium and by cystoid macular oedema.
In the past, the diagnosis of CH was often made after enucleation for suspicion of primary or secondary malignant tumours in the choroid or after development of a painful secondary glaucoma resistant to therapy. Since the introduction of routine diagnostic ultrasound echography and fluorescein angiography,4 CH can be diagnosed with sufficient confidence to permit specific therapy whenever possible.
Management options include photocoagulation,5-8diathermy,9 10 cryotherapy,11 external irradiation,12-15 and brachytherapy.16 Laser photocoagulation is generally considered to be the preferred therapeutic intervention for CH.17 18 The disadvantages of this form of treatment are that multiple sessions are often necessary,7 8 and the visual outcome is limited because of the close proximity of the solitary tumours to the fovea or because of the large size of diffuse haemangiomas.
By choosing external high energy photon irradiation, tumour destruction as the primary therapeutic goal has been abandoned in favour of the more limited aim of resolving subretinal fluid. First experiences were reported in 1984/85 from our institution.12 13
The present study describes the functional and anatomical results of external ocular irradiation and provides the opportunity to recommend treatment guidelines.
Patients and methods
A total of 51 eyes (48 patients, 28 male/20 female) were irradiated; 36 eyes had a circumscribed CH of the posterior pole and 15 eyes (12 patients, 7 male/5 female) exhibited a diffuse CH as part of the Sturge–Weber syndrome (Table 1). Each patient had a retinal detachment involving or threatening the fovea. Six eyes had had previous laser treatment.
Clinical characteristics of 51 irradiated eyes
The mean age of the patients with circumscribed haemangiomas was 45 years with age ranging from 22 to 66 years. The mean follow up time was 4.5 years (range 4 months to 24 years, median 4 years).
The mean age of the 12 patients (15 eyes) with diffuse haemangiomas as part of a Sturge–Weber syndrome was 18.3 years. Seven eyes of this group were functionally ‘only eyes’, and eight eyes had secondary glaucoma. The mean follow up time was 5.3 years.
The average height of the tumours measured by standardised A-scan echography was 3.9 mm in the circumscribed CH cases and 4.1 mm in the diffuse cases of Sturge–Weber syndrome; the latter showed much larger diameters, with nine of the 15 eyes exceeding the size of one quadrant.
RADIATION TECHNIQUE
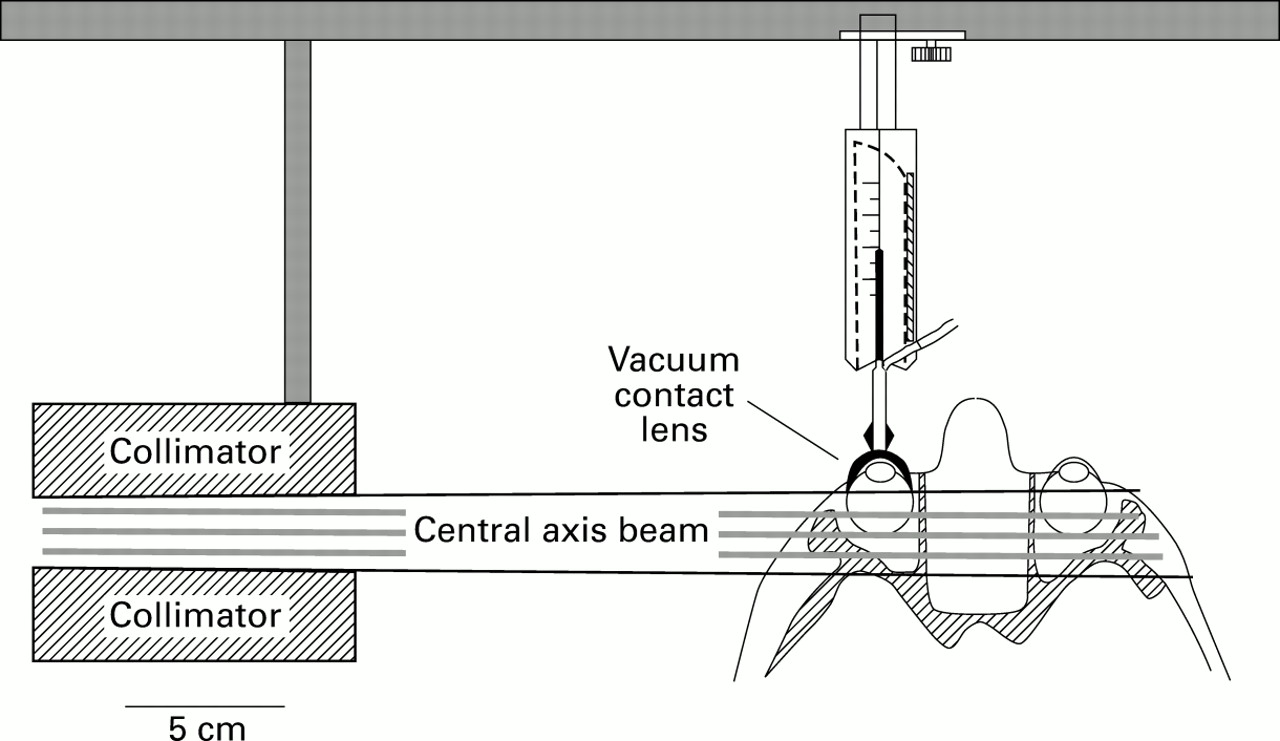
All patients received external irradiation with high energetic photons over a lateral field. As a standard treatment, a total absorbed dose of 20 Gy (2 Gy per fraction) was routinely delivered. Until 1978 two telegamma apparatus served as the radiation source for five patients (cobalt-60 in two cases and caesium-137 in three cases). Since then, linear accelerators have been used as the radiation source. According to the developmental stages of the technique, the irradiation was delivered in a lens sparing fashion. From 1984, a highly precise technique was applied, which was originally developed for the irradiation of retinoblastomas19 and was based on that described by Schipper and Tan20 (Fig 1). After instillation of a topical anaesthetic the eyes are held in position by a vacuum contact lens. Using ultrasonographic biometry the irradiation field is placed in such a way that less than 2% of the delivered dose reaches the posterior pole of the lens.21 The irradiation table is orientated in a direction so that the irradiation beam bypasses the healthy contralateral eye.

Radiation technique (modified principle of Schipper and Tan’s technique that was originally designed for irradiation of retinoblastomas20). By adjusting the collimators the beam can been focused more precisely on the location of the haemangioma.
EVALUATION OF PATIENT DATA
For each patient the following were recorded: (a)the visual acuity (VA) at time of irradiation (tested with best Landolt circles according to DIN 58220 and best optical correction); (b) the VA at the last examination after the treatment; (c) the morphology as seen by ophthalmoscopy and fluorescein angiography; (d) the tumour height determined by standardised ultrasound before and after treatment. The influence of tumour height, location, and duration of symptoms were related to the outcome. The relation to the fovea was determined as juxta-, extra-, or subfoveal according to the definitions of the Macular Photocoagulation Study Group.22 Data that reliably indicated the time of onset of the first subjective symptoms were available in 33 of the patients with circumscribed haemangiomas. No patients were lost to follow up.
For statistical analysis of correlations, the Wilcoxon test and regression analysis were applied.
Results
Circumscribed and diffuse CH of Sturge–Weber syndrome were evaluated separately in terms of the morphological and the functional outcome.
GROUP WITH CIRCUMSCRIBED CH
In all 36 cases in this group the eye could be salvaged without complications. Echographic examination showed no decrease of tumour height, the exception being the cases that received additional laser therapy.
In 23 cases (63.8%) with a collateral retinal detachment only or an additional peripheral detachment over less than one quadrant, complete resolution of the subretinal fluid was achieved. Five of these patients received additional laser therapy (argon blue) when reattachment of the retina over the tumour itself was present but further resolution of subretinal fluid in the periphery had stopped. The remaining 13 cases (36.2%) showed residual serous detachment distant to the fovea at the time of the last examination. It was evident that these cases either had a high exudative retinal detachment over more than one quadrant before therapy (11 cases) or had a follow up time shorter than 6 months (two cases).
Complete resolution of exudation was accomplished within 3 to 6 months after treatment while reattachment of the fovea occurred earlier, usually between 2 and 4 weeks after commencement of therapy (Figs 2 and3).
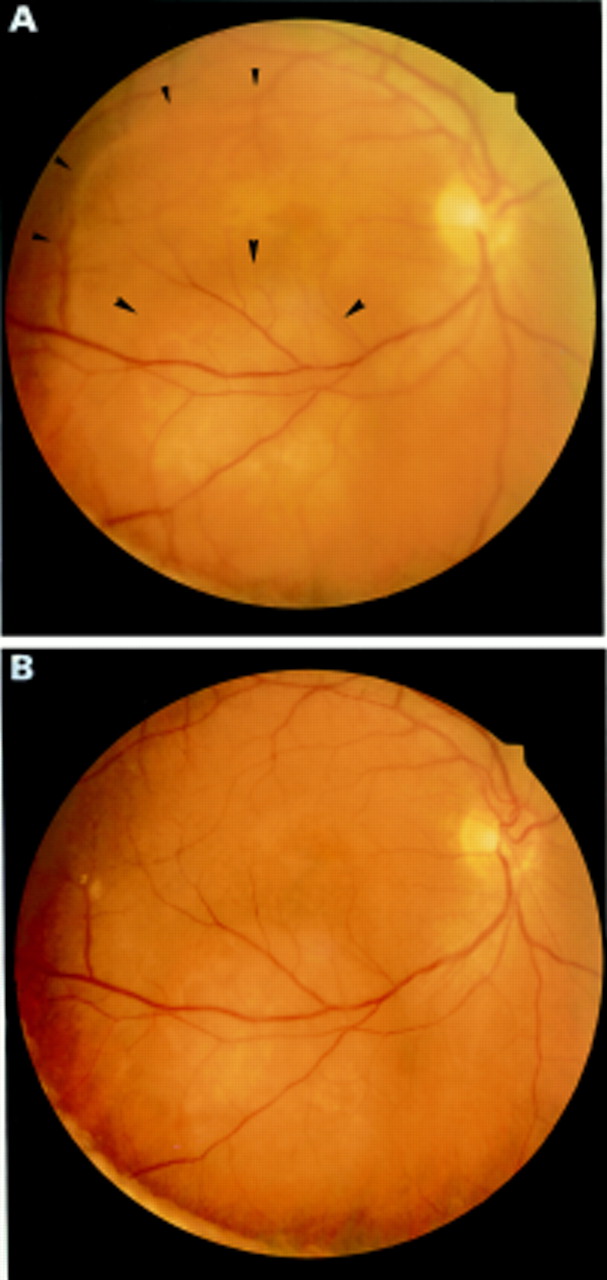
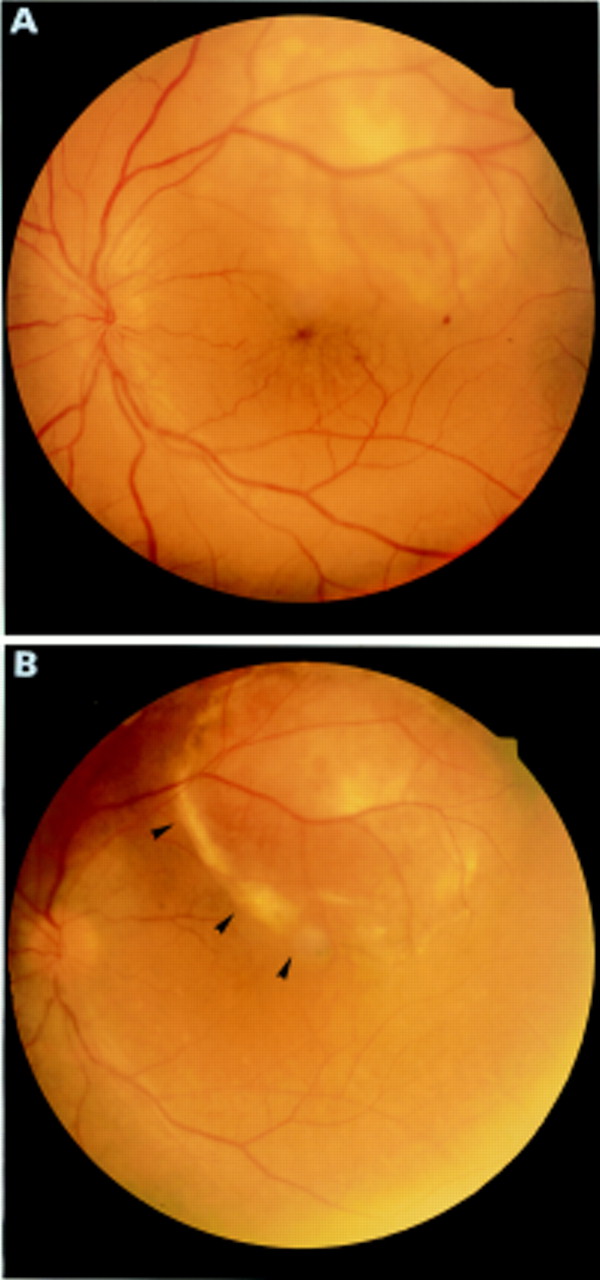
Follow up in a 42-year-old male patient with a circumscribed choroidal haemangioma of the posterior pole. (A) Situation before therapy. Note the extent of the exudative detachment that includes the fovea (small arrows) and the better visible haemangioma under the lower temporal main branch of vessels (large arrows). (B) Stable situation 1 year after therapy with completely reattached retina. The VA improved from 0.1 to 0.4.


Angiographic follow up of a circumscribed choroidal haemangioma (CH) of a 40-year-old male patient. (A) Ophthalmoscopic appearance of an extrafoveally located CH. (B) Mid phase picture of fluorescein angiography before therapy. (C) Late picture before therapy. (D) and (E) Mid phase and late picture 8 weeks after therapy.
The visual acuity improved by 2 or more lines in 14 cases (38.9%), remained stable in 14 cases (38.9%) and further decreased in eight cases (22.2%). In four of the eight cases, the VA before therapy had already been below 0.1 with significant pigment epithelial changes in the macula, which were observed at last examination. In contrast, the other four cases deteriorated considerably after an initially satisfactory improvement immediately after therapy which was attributable to an increasing formation of subretinal fibrosis that extended to the fovea (Fig 4).

Development of subretinal fibrosis after successful treatment (case 6 in Fig 8). (A) Situation before therapy with extension of the exudative retinal detachment into the foveal region. VA 0.3. (B) Situation 50 weeks after therapy with subretinal fibrosis extending into the foveal region. VA originally improved to 0.4 and dropped to 0.02 within the past 2 years.
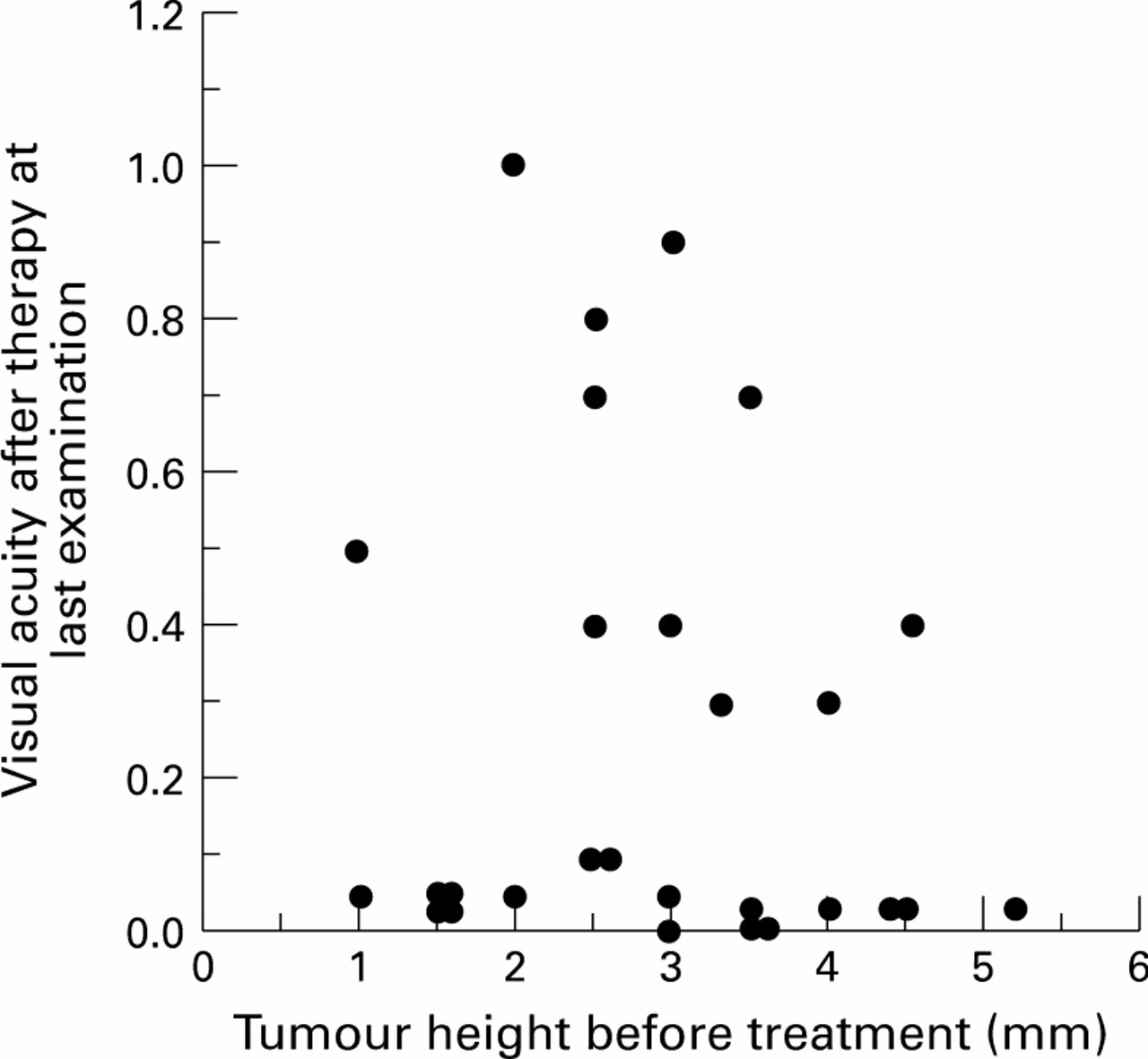
The tumour height and localisation in relation to the fovea did not have a statistically significant influence on the visual outcome (Figs5 and 6). In patients with juxtafoveal tumours (23 cases) the proportion with a VA below 0.1 after treatment was very high, but in this group the patients with low VA before treatment were most often represented. Nevertheless, one patient with an initial VA of lower than 0.1 achieved a VA of 0.9 after treatment. The functional results of extrafoveally located CH showed higher mean values, but by statistical analysis no significance could be demonstrated between location and the VA after treatment (Wilcoxon test: p<0.68).
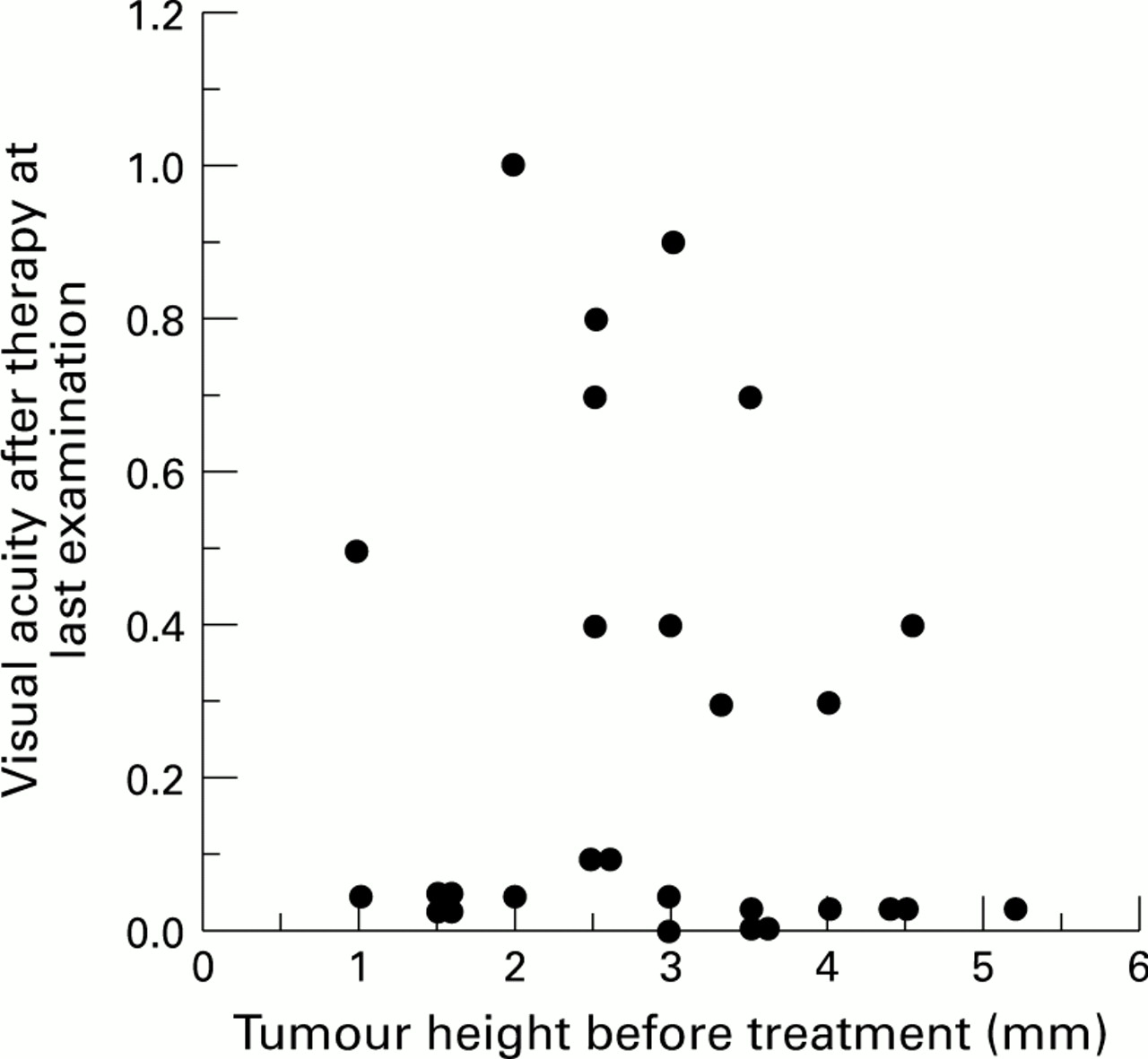
Tumour height and final visual outcome. No significant correlation in regression analysis (p <0.42).
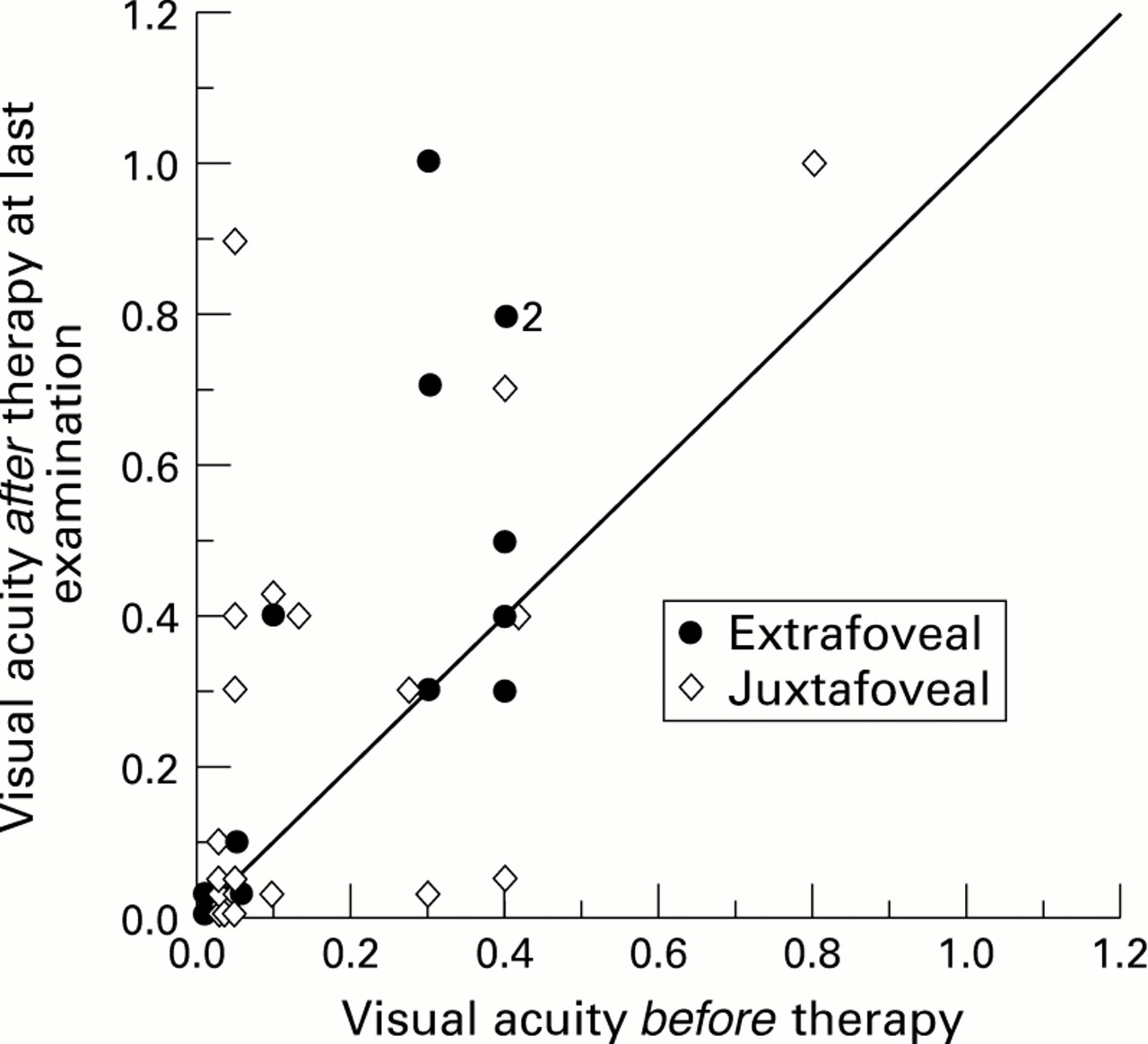
Final visual outcome and localisation of the tumour. No significant correlation (p <0.68 in Wilcoxon test).
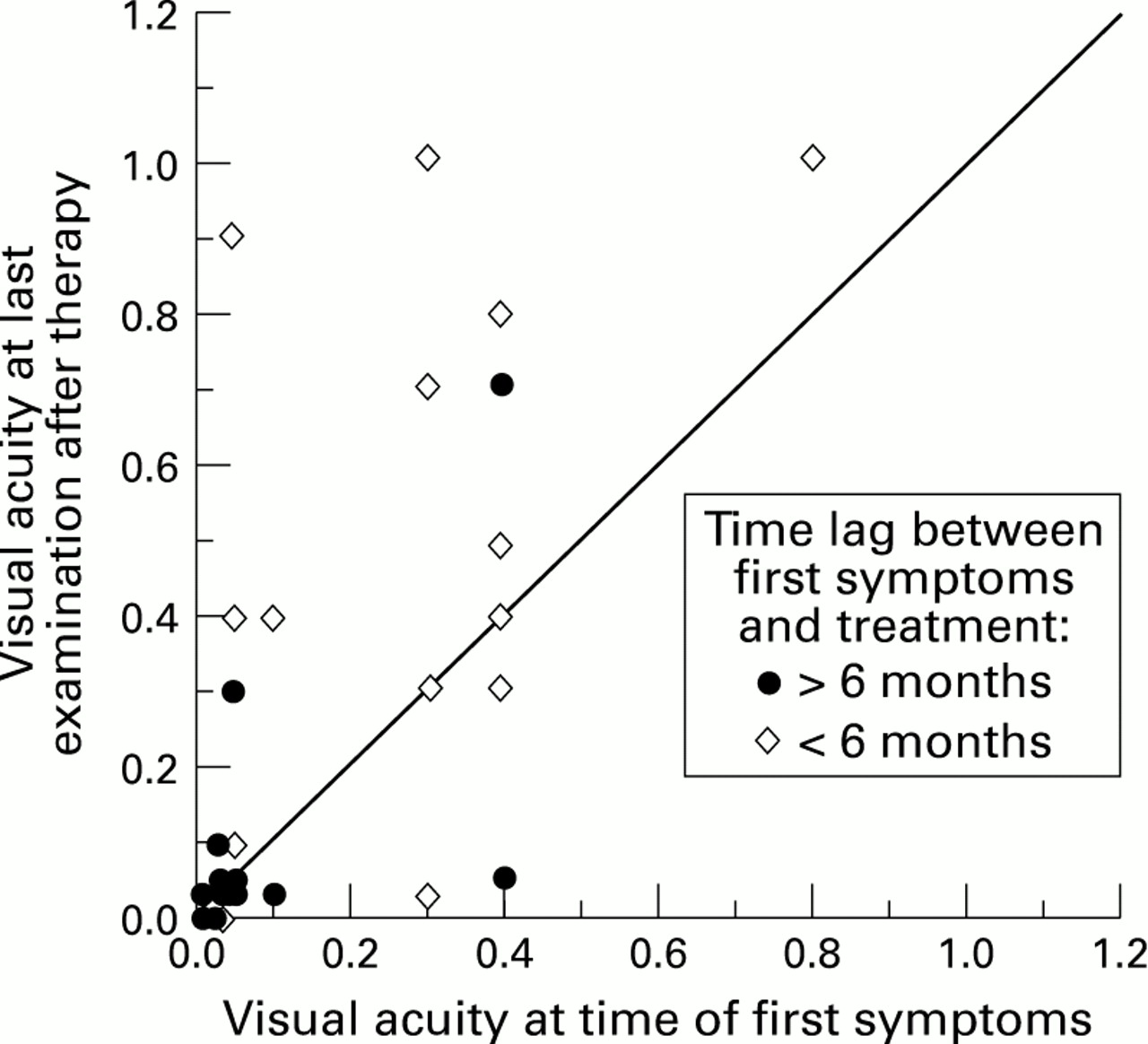
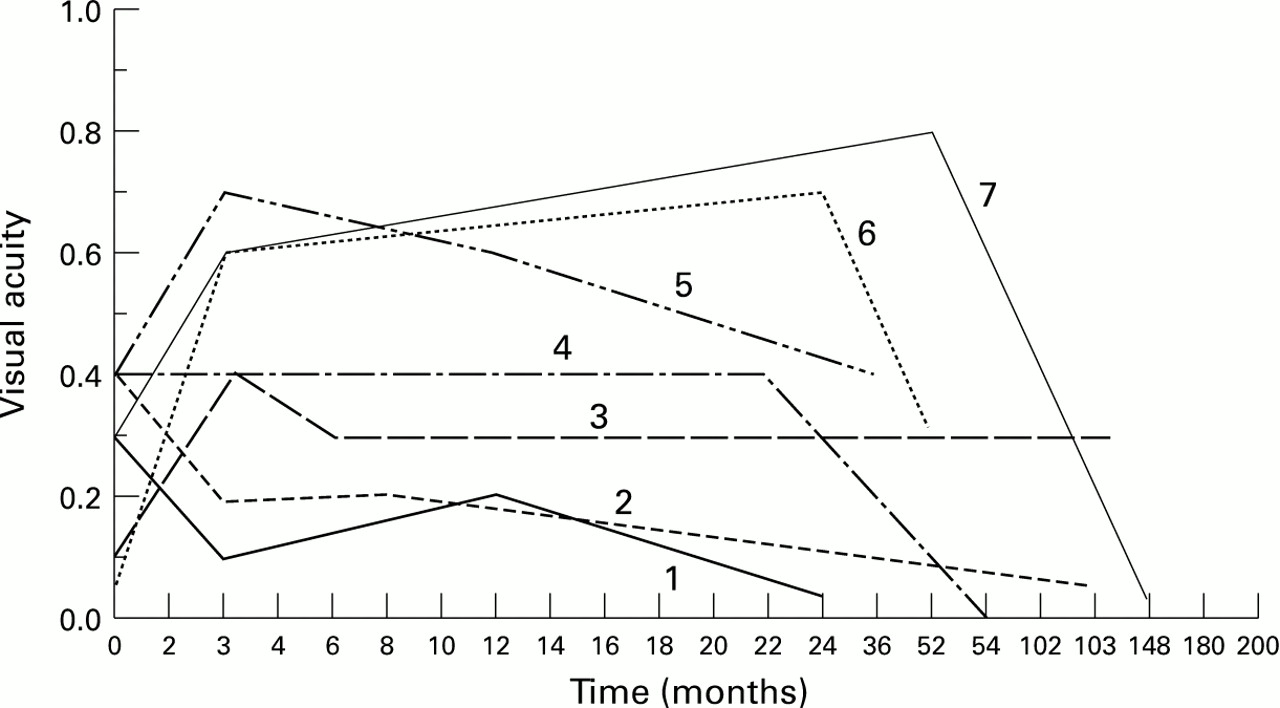
The functional success was significantly dependent on the lag duration between first onset of symptoms and treatment (Fig 7). When comparing the final VA of patients treated within 6 months after first subjective signs of visual deterioration with the final VA of patients treated later, the results of earlier treatment are considerably better (Wilcoxon test: p<0.01). In seven out of 16 patients with early treatment, follow up has shown a late deterioration of the VA after an initial improvement that was mainly attributed to the formation of subretinal fibrosis (Figs 4 and 8).
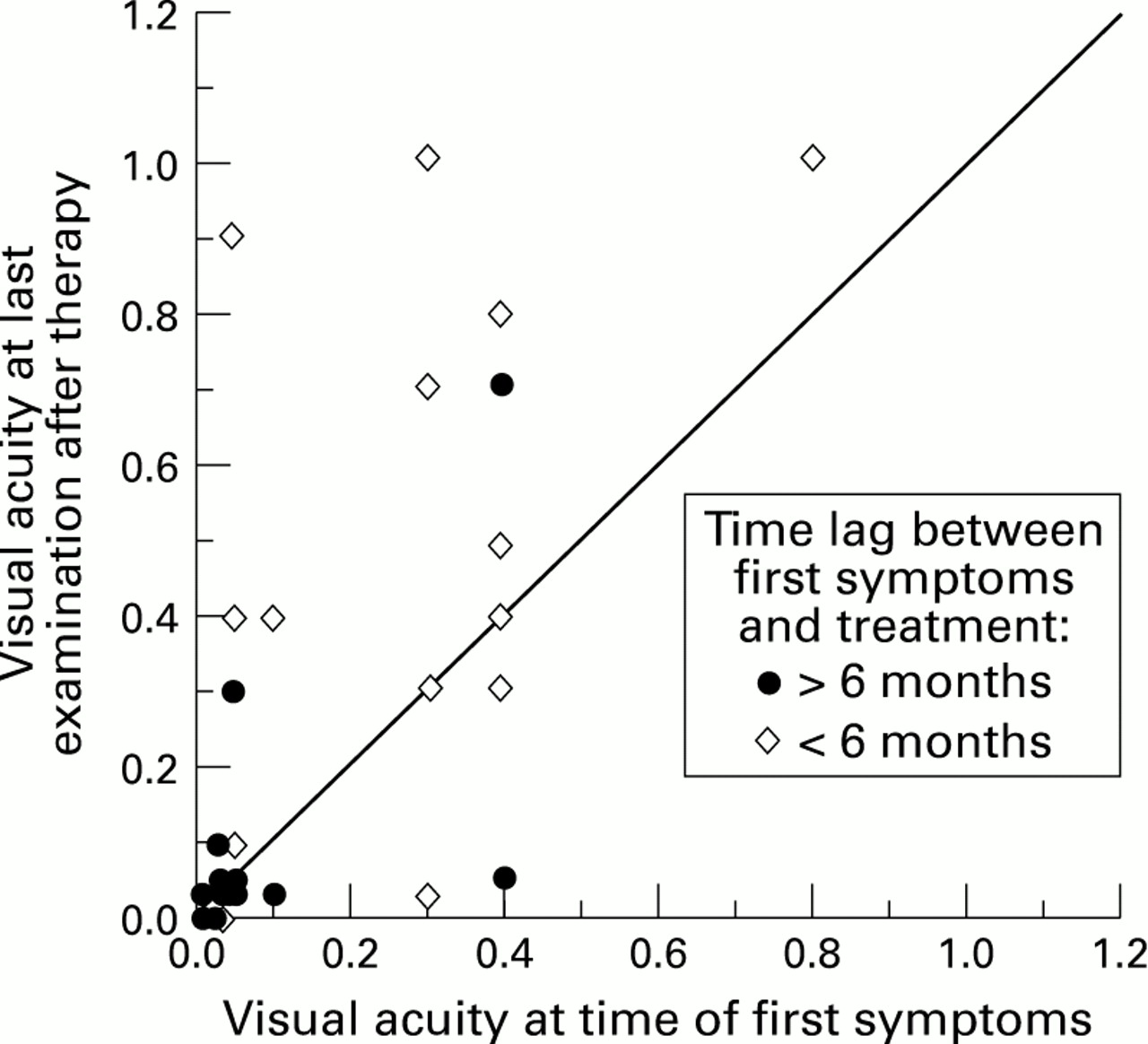
Final VA correlated with the time lag between first symptoms and treatment in 33 patients with circumscribed choroidal haemangioma. Time lag > 6 months (n = 17). Time lag < 6 months (n = 16). In the group with shorter time lag the functional results were significantly better; p < 0.01 in Wilcoxon test.

Follow up of VA of the seven cases with circumscribed haemangiomas that had a final VA equal to or lower than the VA before treatment although they had received radiotherapy early (open symbols in Fig 7). After an initial improvement following treatment the VA later deteriorated mainly due to secondary fibrous metaplasia of the retinal pigment epithelium. (Non-linear presentation on x axis).
Radiation induced side effects, such as cataract or retinopathy, were not observed.
GROUP WITH DIFFUSE CH/STURGE–WEBER SYNDROME
The results of this group were similar morphologically to the group of circumscribed CH. All eyes were preserved at least for the period of follow up. Shrinkage of the tumour mass was seen in five eyes and confirmed by standardised ultrasound echography which showed height decreases ranging from 1 to 3 mm. All these eyes had shown an original tumour height of >4 mm.
The VA at last examination improved by 2 or more lines in seven eyes (46.6%) and was unchanged or deteriorated in eight eyes (53.4%) (Fig9). Six of these eyes had uncontrolled secondary glaucoma before this treatment. In all these cases the intraocular pressure was not relieved by the treatment but was within normal range with topical antiglaucomatous therapy in four cases and ranged between 22 and 30 mm Hg in two cases at the last examination.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Functional outcome of 15 eyes with diffuse choroidal haemangiomas in Sturge–Weber syndrome.
Discussion
The results of this study demonstrate the benefit of low dose ocular irradiation for resorption of the subretinal fluid over symptomatic choroidal haemangiomas. All eyes could be salvaged without subjective symptoms and additional laser treatment was considered as necessary in only a very small number of cases.
In about two thirds of all cases complete resorption of the exudation without recurrence during the follow up time was achieved. The functional outcome was mainly dependent on the time delay between the first onset of symptoms and the beginning of therapy and on secondary glaucoma in the case of Sturge–Weber syndrome. As a result of the close proximity of most choroidal haemangiomas to the foveal region, a prompt decrease of visual acuity due to exudative retinal detachment is often an early symptom. The associated damage to the foveal photoreceptor layer is comparably small when the detachment of the retina is of short duration. As a consequence of persisting exudation, however, degenerative changes in the foveal retina, secondary fibrous metaplasia, or atrophy of the retinal pigment epithelium and cystoid macular oedema lead to irreversible functional loss.
The concept of tumour destruction of CH was first abandoned by Gass in 1974.23 24 His recommendations for laser therapy of these tumours emphasised the reduction of subretinal fluid as main therapeutical aim.
Sanborn et al 7 reported in 1982 the first large series of 59 cases of CH treated with photocoagulation. Their morphological results are similar to those of this study, although in a considerable number of cases repeated therapeutic sessions were necessary to treat multiple recurrent subretinal exudations. Sanbornet al 7 considered it disappointing that only 22.5% of their patients reached a VA of 0.5 or better, but they did not attempt to differentiate for the time interval between onset of symptoms and first treatment. In 1989, long term observations based on 64 treated patients from the same institution8 were published: stabilisation of VA was achieved in 53% of all cases, 72% of the patients had a VA lower than 0.4, and the authors estimated from their data that a significant proportion of patients would experience a further decrease of VA within 10 years despite initially successful treatment.
In a recent study by Zografos et al,16 the results of tumour destructive therapy in 41 patients by cobalt-60 brachytherapy were reported. In this series the complete resolution of subretinal fluid and formation of a flat chorioretinal scar were observed in all cases. Progress of visual acuity was measured using a four category scale of VA ranging from 20/200 or worse, to 20/20. In 31 cases with a 2 year follow up an improvement by one or even two categories was achieved. The presence of infiltration of the macula, retinal detachment of the fovea in the absence of pigment migration into the macula, subretinal fibrosis, and cystoid macular oedema were not prognostic indicators of final visual acuity. The overall outcome of this series seems to be comparable with the results from our study. Complete tumour destruction, however, has not been shown to have a significant advantage over the therapeutic options described above and that used in our study. It is our opinion that this invasive procedure should be reserved for very special indications.
Irrespective of treatment option, a stable reattachment of the fovea would probably allow the most desirable form of restoration of visual function. In our study the application of the dose of 20 Gy is not tumour destructive but results in complete resorption of the subretinal fluid in the vast majority of cases with reattachment of the fovea achieved in all cases. The exact mechanism of the radiation effect of low dose irradiation on CH is unknown, especially since there are no histological descriptions available nor are there systematic studies of the radiation effects in benign vascular tumours.25
True regression of the tumour was not seen in any of the cases with circumscribed CH and only in a minor percentage of diffuse CH cases. An explanation may be due to the higher incidence of cavernous architecture in circumscribed CH2 resulting in a different and more resistant radiation response. This observation contradicts a previous report, from our institution, of external irradiation for CH on 22 patients by Alberti,15 although the functional results were similar with improved or stable VA in 15 eyes. A possible explanation may be the different interpretation of ultrasound measurement at that time (1977–84). The patients from this period were therefore excluded from our study.
In 1991 Scott et al reported their results of a comparable technique of external irradiation on five eyes with diffuse CH and bullous serous retinal detachment as part of the Sturge–Weber syndrome.14 Their results for diffuse CH were comparable with those of our study in that complete resolution of subretinal fluid was achieved although there was no substantial improvement of VA.
A consistent finding in all larger studies of treated CH is the occurrence of subretinal fibrosis, which may be considered as a fibrous metaplasia of the retinal pigment epithelium and was seen irrespective of treatment choice. The fibrotic tissue predominantly extends to the fovea, and as a consequence, dramatic loss of VA can be a late complication; in one of our cases this pathology resulted in visual deterioration 10 years after treatment (Fig 9).
The external therapy with high energetic photons did not show any side effects in the application used in this study. The doses applied are far below the dose rate where radiation retinopathy can represent a serious complication.26 The lens sparing radiation technique was most effective against the development of any radiation induced cataract while still ensuring the prescribed dose to the CH.
It is our opinion that external beam irradiation with adjunctive photocoagulation in selected cases represents the best treatment of CH. A critical factor in a successful outcome would be the early commencement of treatment upon the first presentation of subjective signs of deterioration. Irreversible loss of function can be anticipated when symptoms are of long duration.
The following principles for treatment of CH are recommended:
- (1)
Periodic observation for incidentally detected asymptomatic CH without exudative retinal detachment threatening the fovea.
- (2)
External radiotherapy for CH with retinal detachment including or threatening the fovea, at the earliest time after onset of first subjective symptoms.
- (3)
Additional laser coagulation following the treatment guidelines by Gass24 in cases with insufficient resorption of subretinal fluid after radiotherapy.