Article Text

Abstract
BACKGROUND Squamous tumours of the ocular surface, including the lacrimal pathway, range from benign lesions to invasive carcinomas. Some of these tumours are associated with human papillomavirus (HPV) infection, with the types of HPV differing among papillomas and dysplastic or malignant lesions.
METHODS The relation between squamous tumours of the conjunctiva and lacrimal sac and HPV infection was investigated in 17 individuals with such tumours. Nine of the 17 tumours were benign, four were dysplastic lesions, and four were carcinomas.
RESULTS Eight specimens showed positive immunohistochemical staining with antibodies to HPV; four of these eight were papillomas, three were dysplastic lesions, and one was a carcinoma. Koilocytosis was detected in seven of these eight tumours. Five of the eight specimens positive for immunohistochemical staining were also positive for HPV DNA by in situ hybridisation, and all eight were positive for HPV DNA by the polymerase chain reaction (PCR) method.
CONCLUSION Approximately 50% of squamous tumours of the ocular surface and lacrimal sac were associated with HPV infection. This is the first report, to our knowledge, of the detection of HPV in the field of ophthalmology by a combination of immunohistochemistry, in situ hybridisation, and PCR.
- human papilloma virus
- immunohistochemistry
- in situ hybridisation
- polymerase chain reaction.
Statistics from Altmetric.com
Human papillomavirus (HPV) is associated with neoplasms of human squamous epithelia in regions of the cervix,1 urogenital tract,2 and larynx.3 HPV types 6 and 11 are associated with benign lesions, and types 16, 18, 31, and 33 with dysplastic lesions or carcinomas.4 5 HPV has also been detected in squamous tumours of the eye, including both benign6-10 and malignant11-14 lesions. These studies relied on only one or two methods, selected from immunohistochemistry, in situ hybridisation, and polymerase chain reaction (PCR), to detect HPV. We have now applied all three approaches to detecting HPV infection of the ocular surface and lacrimal pathway.
Materials and methods
The study subjects were 17 Japanese individuals (13 males and four females, aged 20 to 73 years), 15 of whom had squamous tumours of the conjunctiva or corneal limbus and two had squamous tumours of the lacrimal sac (Table 1).
Clinicopathological data and results of human papillomavirus (HPV) analysis
HAEMATOXYLIN AND EOSIN STAINING
Formalin fixed, paraffin embedded sections of each lesion were stained with haematoxylin and eosin and examined to confirm the diagnosis. The presence of a papillomatous growth pattern or koilocytosis was noted, and the lesions were classified on a scale ranging from benign to invasive squamous cell carcinoma.
IMMUNOHISTOCHEMICAL STAINING
Ten per cent of formalin fixed and paraffin embedded tissue from each case was used for immunohistochemical staining of HPV. Rabbit antibovine papilloma virus antibody was purchased from Dako (Carpinteria, CA, USA). This antiserum is reactive with papillomavirus genus specific (common) structural antigens regardless of host species. Immunohistochemical staining was performed by the avidin-biotin-complex method.15 The sections were deparaffinised, endogenous peroxidase was blocked by incubation of the slides for 10 minutes in 1% NaIO4, and, after being washed, the slides were incubated with primary antibodies (dilution 1:1000). The slides were then exposed to a biotinylated anti-rabbit immunoglobulin antiserum (dilution 1:500), avidin (dilution 1:1000) and biotinylated horseradish peroxidase complex, all of which had been purchased from Dako. We obtained the peroxidase reaction by incubating the slides in 0.005% H2O2 and 0.02% 3,3′ diaminobenzidine tetrahydrochloride for 10 minutes. We examined specimens of penile condyloma as a positive control, and used phosphate buffered saline instead of primary antibody as the negative control.
IN SITU HYBRIDISATION
In situ hybridisation was carried out using a method described previously.9 In brief, paraffin embedded sections were placed on silane coated slides and first examined with two broad spectrum HPV probes (a broad spectrum HPV biotinylated DNA probe purchased from Dako, which recognises HPV types 6, 11, 16, 18, 30, 31, 33, 35, 45, 51, 52, and a broad spectrum HPV digoxigenin labelled DNA probe purchased from Nichirei, Tokyo, Japan, which recognises HPV types 1, 2, 6, 11, 16, 18, 31, 33) for the detection of HPV DNA. Subsequently, all specimens were examined with biotin labelled type 6 and type 11 HPV probes, biotin, or digoxigenin labelled probes for HPV types 16, 18, 31, and 33 to confirm the type of HPV present. Briefly, paraffin sections were treated with xylene, hydrated with a graded series of ethanol solutions, treated with 0.1M HCl and proteinase K (0.1 mg/ml) at 37°C for 30 minutes, and then dehydrated. The probes were pipetted onto the slides, which were then covered with siliconised coverslips and heated on a 90°C heating block for 5 minutes to denature both tissue and probe DNA. Hybridisation was performed overnight at 37°C in a humidified chamber, to achieve high stringency, after which the specimens were washed with 2 × SCC (0.3M NaCl, 0.03M sodium citrate) twice at 37°C, dehydrated, and dried in air. The staining solution contained streptavidin labelled horseradish peroxidase or nitro blue tetrazolium. For biotin labelled probes, the sections were immersed in DAB solution for 30 minutes. Cytospin slides purchased from Nichirei and the specimens of penile condyloma were used as positive controls.
POLYMERASE CHAIN REACTION
For PCR analysis,16 ten 10 μm thick paraffin embedded sections were placed in a microtube, dewaxed twice with xylene, washed twice with ethanol, and dried. Digestion buffer containing 0.01% proteinase K and 1% sodium dodecyl sulphate was added to the tube, and the samples were incubated overnight at 48°C. DNA was routinely purified from the digested tissue by RNase I treatment, phenol-chloroform extraction, and ethanol precipitation. DNA was resuspended with 50 μl of a TRIS EDTA buffer. Amplification of HPV DNA by PCR was achieved with the sense primer pU-31B (5-TGCTAATTCGGTGC TACCTG) for HPV types 6 and 11, or pU-1M (5-TGTCAAAAACCGTTGTGTCC) for the dysplastic and malignant HPV types 16, 18, 31, and 33, and the universal antisense primer pU-2R (5′-GAGCTGTCGCTTAATTGCT C).17 Primers for amplification of the human β globin gene (5′-ACACAACTGTGTTCAC TAGC-3′ and 5′-CAACTTCATCCACGT TCACC-3′17) were used to assess the effectiveness of DNA extraction.
Amplification was performed in a thermal cycler (Perkin Elmer Cetus, Wilton, CT, USA) for 35 cycles of 94°C for 1 minute, by incubation at 52°C for 1 minute, and 72°C for 1 minute. Cycles were preceded by incubation for 5 minutes at 94°C to ensure full denaturation of the target DNA, and were followed by an extra 5 minutes at 72°C to ensure full extension of products. The PCR products (10 μl) were analysed by electrophoresis through a 4% Nusieve GTG agarose gel (FMC BioProducts, Rockland, ME, USA) and ethidium bromide staining. For identification of HPV types 6 or 11 or types 16 or 18, the PCR products (10 μl) were digested with Rsa I or Ava II, respectively, in a 15 μl reaction mixture for 1 hour at 37°C.18
Results
The clinicopathological data and the results of the immunohistochemical staining, in situ hybridisation, and PCR analyses for the 17 patients are summarised in Table 1. Histology revealed the tumours in nine individuals to be benign squamous papillomas while those in the remaining eight were dysplastic lesions or carcinomas; of the latter eight tumours, one showed moderate dysplasia, three severe dysplasia, two were identified as carcinoma in situ, and two were invasive squamous cell carcinomas (Fig 1). Although the number of males exceeded that of females, there appeared to be no relation between either sex or age and whether the lesion was benign or malignant. Distinct koilocytosis was detected in seven tumours; four benign lesions, one with moderate dysplasia, and two with severe dysplasia.
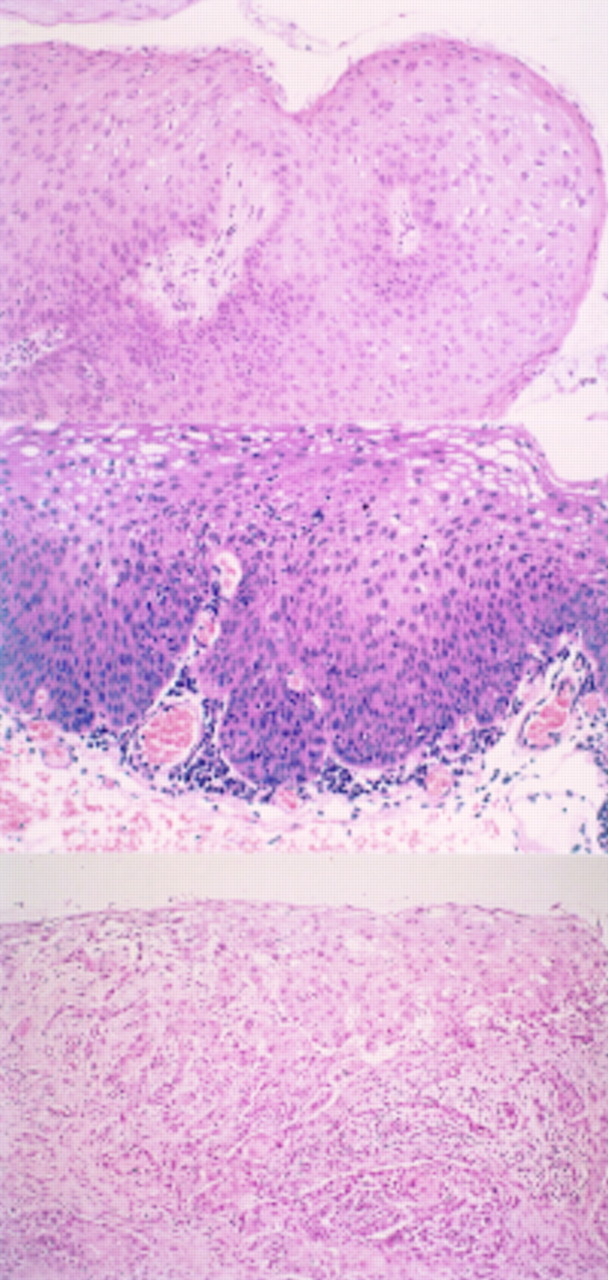
(Upper) Benign squamous papilloma of the corneal limbus (patient 6). Papillary growth of squamous epithelia and koilocytosis are apparent (haematoxylin and eosin staining, × 150). (Middle) Moderate dysplasia of the corneal limbus (patient 10). Atypical cells with hyperchromatic nuclei occupy half the thickness of the epithelium. Mitotic figures and koilocytosis are apparent (haematoxylin and eosin staining, × 150). (Lower) Invasive squamous cell carcinoma of the bulbar conjunctiva (patient 16) (haematoxylin and eosin staining, × 150).
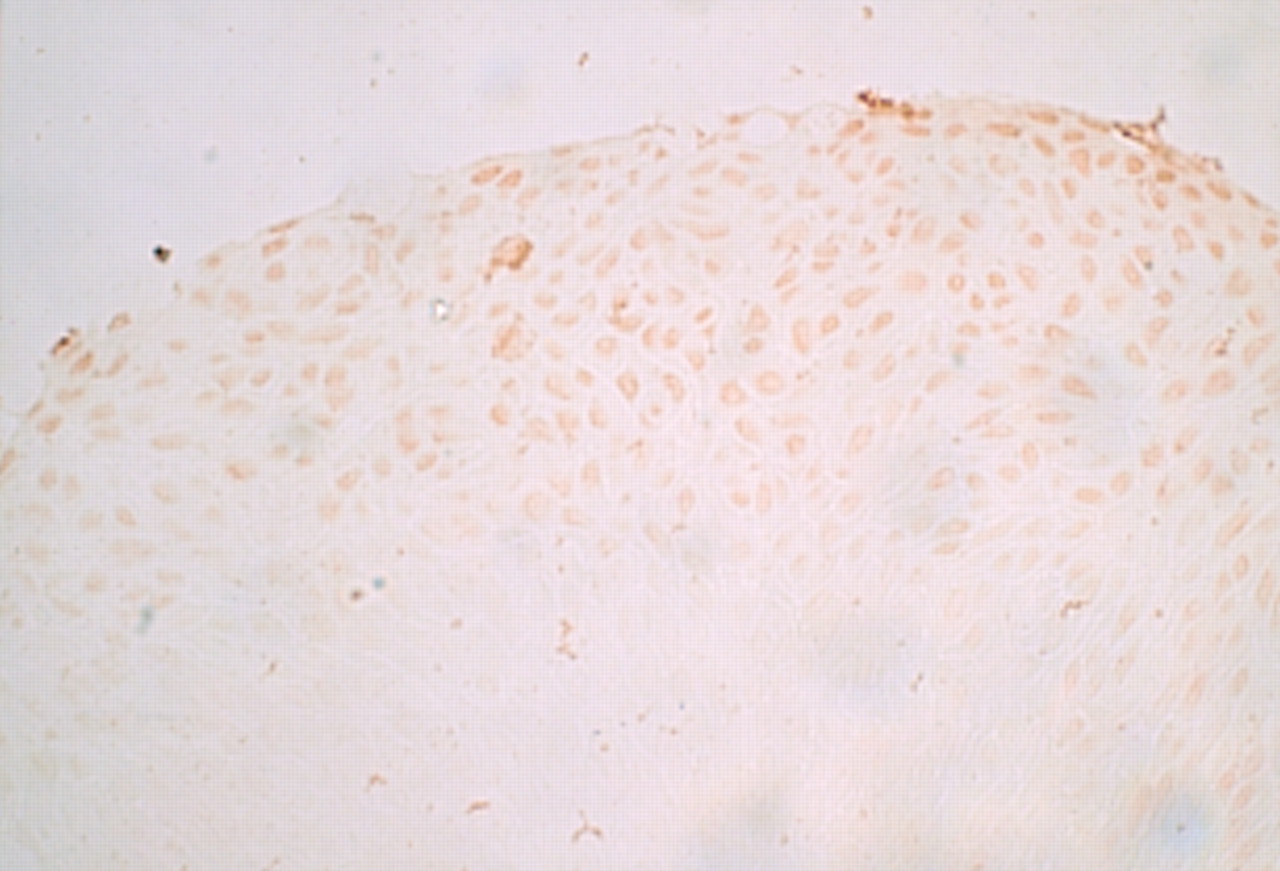
Immunohistochemical analysis showed that tumour cells, from the eight patients reacted with antibodies to bovine papilloma virus. Typically, dense brown precipitates were present in the nuclei and cytoplasm of cells in the most superficial epithelial layers. Of the eight positive tumours, four were benign lesions (Fig 2), one showed moderate and two severe dysplasia (Fig 3), and one was identified as carcinoma in situ (Fig 4). Seven of these eight tumours also showed koilocytosis by haematoxylin and eosin staining.

Immunohistochemical staining of a benign lesion (patient 4). The nuclei and cytoplasm of the tumour cells show brown staining (×160).

Immunohistochemical staining of a tumour showing severe dysplasia (patient 11). The nuclei and cytoplasm of the epithelia show positive staining with antibodies to HPV (× 160).

Immunohistochemical staining of a carcinoma in situ (patient 14). The nuclei and cytoplasm of cancer cells in the superficial epithelial layers show brown staining (× 160).
In situ hybridisation with broad spectrum probes detected HPV DNA in five tumours. Subsequently, specimens from the five positive cases (patients 1, 6, 10, 11, and 13) were subjected to hybridisation with probes specific for HPV types 6, 11, 16, 18, 31, and 33. The benign papillomas of the bilateral bulbar and palpebral conjunctiva (patient 1) and the limbus of the cornea (patient 6) reacted with the type 6 probe (Fig 5). The squamous tumour of the corneal limbus with moderate dysplasia (patient 10), although positive with the broad spectrum probe, did not react showing the specific probes. The lesion of the corneal limbus showing severe dysplasia (patient 13) was positive with the HPV type 18 probe (Fig 6). The lesion of the lacrimal sac with severe dysplasia (patient 11) was positive with the HPV type 16 probe. For all tumours positive by in situ hybridisation, the staining of tumour cell nuclei was more marked in superficial epithelial cells than in deeper cells.

In situ hybridisation results of a benign lesion (patient 6). The nuclei of the layers in the upper half of the epithelium are positive for the HPV type 6 DNA probe (× 160). Counterstaining was not performed.
In situ hybridisation results of a lesion with severe dysplasia (patient 13). The nuclei of the tumour cells near the surface are positive for the HPV type 18 DNA probe (× 160). Counterstaining was not performed.
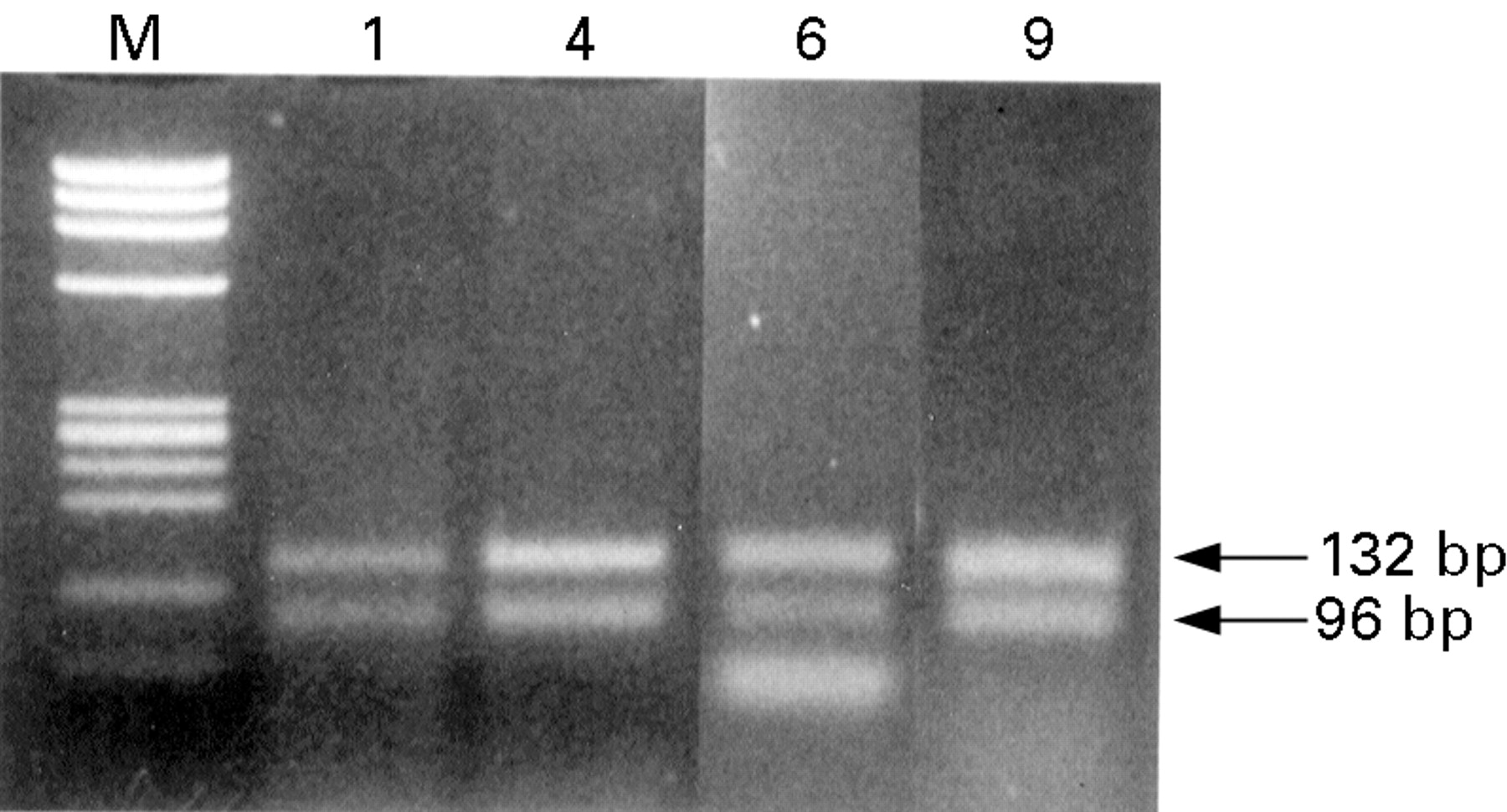
Finally, electrophoretic analysis of the products of PCR amplification and restriction enzyme digestion revealed the presence of HPV type 6 DNA in four tumours (patients 1, 4, 6, and 9) (Fig 7), HPV type 16 DNA in two tumours (patients 10 and 11), and HPV type 18 DNA in two tumours (patients 13 and 14).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Restriction enzyme (Rsa I) analysis of PCR products obtained with primer pair pU-31B/pU-2R (HPV type 6 and 11). Lane M, size marker (HaeIII digested OX174); lanes 1, 4, 6, 9, HPV type 6 DNA (132 bp and 96 bp) of patients 1, 4, 6, and 9. The extra band seen in lane 6 represents primer-dimers.
Discussion
Papillary proliferation associated with HPV infection has been documented in the larynx,19 uterine cervix,20-22 vulva,23 anus,24and penis.25 The epithelia of these lesions are squamous cells, as in papillary lesions of the ocular surface and the lacrimal pathway. In both the uterine cervix20-22 and skin,25-28 HPV types 6 and 11 are associated with benign lesions, whereas HPV types 16, 18, 31, and 33 have been linked with dysplastic lesions and carcinomas. HPV is associated with 95% of cervical dysplasia cases and 89% of cervical cancer cases.25 In the head and neck, HPV causes juvenile papillomatosis, dysplastic lesions, and carcinoma of the larynx19 29-33 as well as carcinoma of the tongue.34 In the field of ophthalmology, some previous studies have shown that papillary lesions of the conjunctiva and the lacrimal sac may be related to HPV types 6 and 118 10 14and squamous dysplasia or carcinoma to HPV types 16 and 18.11-14 These studies relied on only one or two methods, selected from among immunohistochemistry, in situ hybridisation, and PCR. However, we applied all three approaches to detecting HPV infection of the ocular surface and lacrimal pathway.
Koilocytosis associated with cytoplasmic clearing and nuclear pyknosis have been suggested to result from HPV infection.35-37These histological features have been demonstrated in papillary lesions and in regions adjacent to frank malignancies associated with HPV, especially for gynaecological and dermatological lesions.37
In seven cases, we detected koilocytosis and positive results by immunohistochemical staining. Thus, koilocytosis is also an indicator of HPV infection in the eye. We did not detect koilocytosis in the four patients with carcinoma in situ or invasive squamous carcinoma, possibly because we were not able to examine tissue adjacent to the malignancies as excision of the ocular surface and lacrimal pathway had been minimal.
The cases positive for immunohistochemical staining showed precipitates in the nuclei and cytoplasm of cells near the surface of the tumour, suggesting the presence of large amounts of HPV protein in these cells. Five of the eight specimens were also positive by in situ hybridisation with probes specific for HPV DNA. Again, the nuclei of the cells near the tumour surface were stained.
PCR analysis revealed that the eight cases were infected with HPV, in accordance with the positive results yielded by immunohistochemical staining, whereas three of the eight were negative for HPV DNA by in situ hybridisation.
Thus, of the nine benign lesions, four gave positive results with both immunohistochemical staining and PCR, as well as showing koilocytosis, whereas only two tumours showed positive in situ hybridisation results.
Immunohistochemical staining, PCR, and histological assessment of koilocytosis were therefore more reliable indicators than in situ hybridisation for the detection of HPV in benign lesions. On the other hand, of the eight dysplastic lesions and carcinomas, four yielded positive immunohistochemical staining results, and the same four tumours were shown to be infected with HPV type 16 or 18 by PCR. However, only three of these four lesions showed koilocytosis or yielded positive in situ hybridisation results. Thus, immunohistochemical staining and PCR were superior to assessment of koilocytosis and in situ hybridisation for detection of HPV infection in dysplastic lesions and carcinomas.
In the present study, HPV infection was confirmed in nearly half of the cases. HPV probably does not act alone, however, in the development of neoplasia.38 As an example, the interaction of HPV with ultraviolet light has been described in Bowen’s disease of the conjunctiva.39 However, HPV infection is considered to be one of the possible aetiologies of the proliferation of squamous tumours of the ocular surface and lacrimal sac. Thus, squamous tumours associated with HPV, whether benign or malignant, may regrow even after total resection. Ophthalmologists should therefore employ radiation and chemotherapy, in addition to surgical treatment, in the management of squamous lesions of the conjunctiva and lacrimal sac.
Acknowledgments
We thank Drs K Kigasawa, K Yago, S Gotoh, J Kamizono, H Matsuda, and M Nomura for providing specimens.