Article Text

Abstract
AIM The effect of breathing 100% oxygen on retinal and optic nerve head capillary blood flow in smokers and non-smokers was investigated using scanning laser Doppler flowmetry (SLDF) as a new non-invasive method to visualise and quantify ocular blood flow.
METHOD 10 eyes of 10 young healthy non-smoking volunteers (mean age 26 (SD 3) years) and nine eyes of nine young healthy smoking volunteers (mean age 26 (4) years) were investigated. All participants were asked not to smoke or consume caffeine containing drinks for at least 4 hours before the measurements. Blood flow measurements were performed before and after 100% oxygen was applied to the subjects through a mask over a period of 5 minutes (6 litres per minute). Juxtapapillary retinal and optic nerve head blood flow were determined in arbitrary units using SLDF representing a combination of laser Doppler flowmetry and a scanning laser system allowing visualisation and quantification of the retinal and optic nerve head blood flow. Blood flow was determined in an area of 100 μm × 100 μm. The level of carboxyhaemoglobin was determined in all subjects. A Wilcoxon matched pairs signed ranks test (non-parametric) was used for statistical evaluation.
RESULTS In the non-smoking group, retinal ‘flow’ was reduced by 33% (p = 0.005), optic nerve head ‘flow’ by 37% (p = 0.005). In the smoking group retinal flow was reduced by 10% (p = 0.01), optic nerve head flow by 13% (p <0.008). The difference in reactivity to oxygen breathing between smokers and non-smokers was highly significant (p <0.00001). Increased carboxyhaemoglobin levels were not found in either of the groups. A significant reduction of the mean arterial blood pressure of 6% (5%) (p <0.02) was observed in the non-smoking group after administration of oxygen.
CONCLUSION These results indicate that hyperoxia leads to a decrease in capillary blood flow of the retina and optic nerve head secondary to vasoconstriction, and that smokers do not respond to oxygen breathing as non-smokers do. The findings might be based on factors such as long term effects of nicotine on the sympathetic and parasympathetic nervous system.
- oxygen reactivity
- smokers/non-smokers
- retinal capillary blood flow
- scanning laser Doppler flowmetry
Statistics from Altmetric.com
It is well known that vascular tone and blood flow of the retina are significantly influenced by arterial oxygen tension. The vasoconstricting effect of oxygen on retinal vessels has been described by several authors.1 2 There have been studies examining the effect of breathing pure oxygen in normals, diabetics, smokers, and others. Morgado et al 3 have recently investigated the acute effect of oxygen breathing on the vascular regulation of retinal blood flow in smokers before and after smoking. The effects of smoking on the circulation, especially the microcirculation, are based on various mechanisms. An increased intake of carbon monoxide leads to an increased level of carboxyhaemoglobin in the blood of smokers thus reducing the affinity of the haemoglobin for oxygen—that is, the ability to bind oxygen.4 Heavy smokers are supposed to have carboxyhaemoglobin levels of up to 10% compared with 0.1% to 0.5% in non-smokers.5
Nicotine has a direct effect on the vascular system in smokers. In low concentrations nicotine causes an excitation of sympathetic and parasympathetic ganglia. The effect on sympathetic ganglia prevails. Direct stimulation of sympathetic ganglia leads to an increase of the heart rate and the total peripheral resistance due to vasoconstriction. Furthermore, it causes a stimulation of the adrenal glands: the release of noradrenaline contributes to the increase of the peripheral resistance and heart rate.6
The purpose of this study was to identify differences in the ocular vascular reactivity to oxygen between smokers and non-smokers as well as investigating the acute effect of smoking on the retinal and papillary microcirculation and its effect on oxygen reactivity.
Method and subjects
Scanning laser Doppler flowmetry (SLDF) is a combination of a scanning laser system and the well established laser Doppler flowmetry.7-9 Measuring blood flow by laser Doppler flowmetry is based on the optical Doppler effect: light is scattered by tissue and moving particles undergoing a shift in frequency (Df). Scanning laser Doppler flowmetry uses the ability of a laser scanning tomograph to measure the amount of back scattered light at different locations in an area of interest in a very short time.10 Since it is sufficient, when measuring a fluctuating signal, to take samples with a sampling rate of at least twice the highest signal frequency, numerous points of the tissue can be examined very quickly by a scanning method. In previous studies this method has produced good reliability and validity.9 11
Superficial capillary blood flow at a depth of up to 300 μm in the juxtapapillary retina and optic nerve head can be detected. The examined retinal area has a size of 2.7 × 0.7 mm. It has a resolution of 256 points × 64 lines. One sample is taken from each point on the line. Each line is scanned 128 times with a repetition rate of 4000 Hz, leading to an intensity matrix of 256 points × 64 lines × 128 times. Thus, the backscattered intensities of each scanned point are obtained as a function of the time (fluctuation-time curve). The collected intensity data of each retinal point of measurement are then analysed by a discrete fast Fourier transform thus calculating the frequency shift for each point of measurement by which the blood flow ω can be computed. From the calculated data a two dimensional colour map of the retinal/optic nerve head perfusion is created. The brightness of each point is encoded by the extent of blood flow—that is, to the Doppler frequency shift. The variables ‘volume’, ‘flow’, and ‘velocity’ are computed for each pixel. Flow (ω) is calculated by the equation
All variables are relative values and are given as arbitrary units (AU).9 11 Doppler frequencies up to 2000 Hz can be detected using a line sampling frequency of 4000 Hz. Frequencies lower than 125 Hz are excluded to minimise the influence of low frequency artefacts like breathing, cardiac action, and intensity fluctuation as a result of other effects.
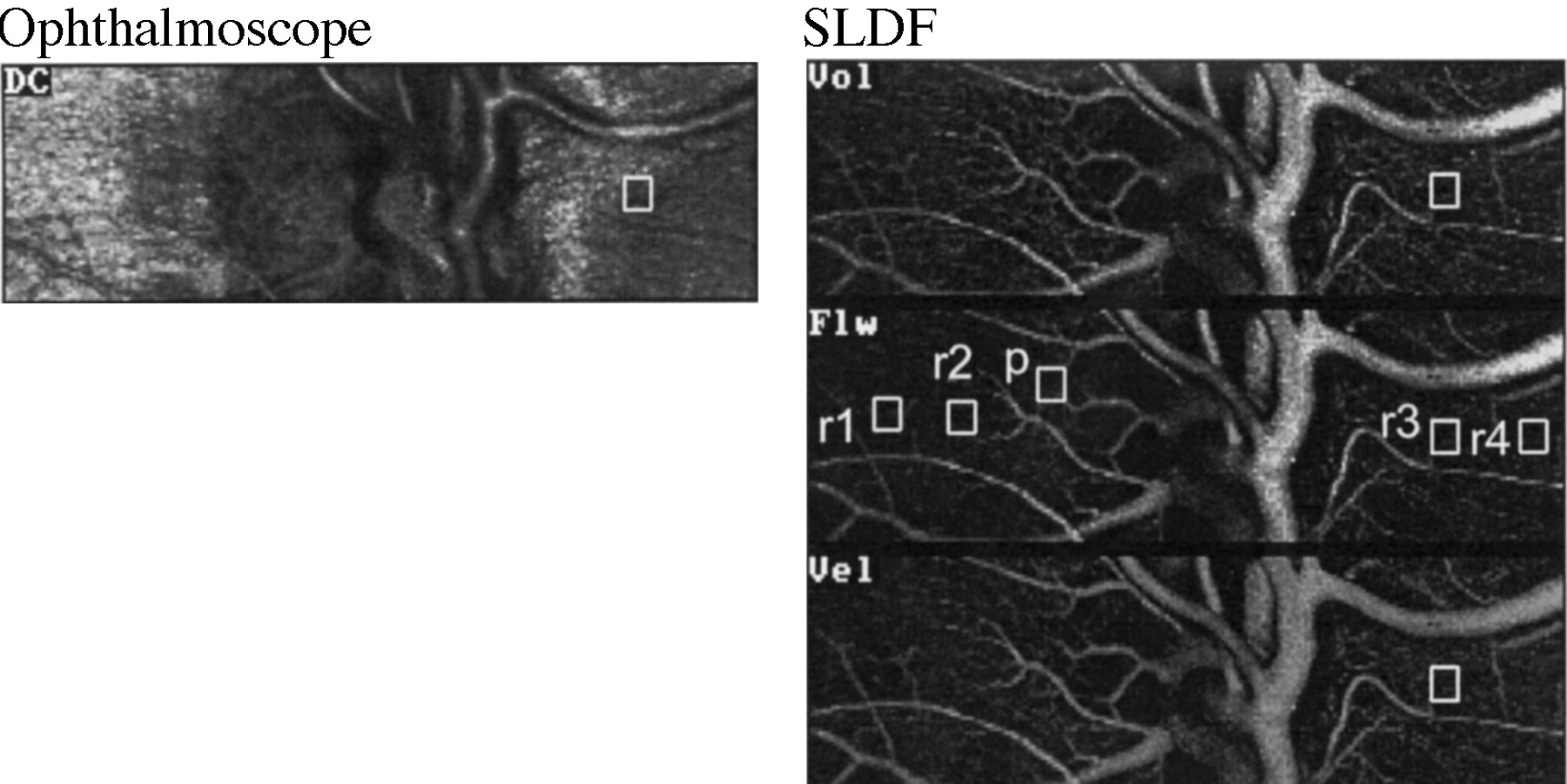
The spatial resolution of the scanning laser system is 10 mm. Our data acquisition and evaluation system is a modified laser scanning tomograph (HRF, Heidelberg Engineering, Germany). As a light source we used a 670 nm laser diode with an optical power of 100 mW. The system scans the area of interest in a 10° sector without pupil dilatation using a confocal optical system. For evaluation a square variable in size can be moved to any point in the image (see Fig 1). For our study we scanned the optic nerve head and the juxtapapillary retina and evaluated two nasal and two temporal retinal areas and one optic nerve head area (see Fig 2). These retinal areas of measurement were chosen randomly away from visible large vessels. From the four retinal values the mean was calculated. We always used a square of 10 × 10 pixels, thus a sampling area of 100 μm × 100 μm. The same retinal and optic nerve head areas were examined and evaluated before and after breathing oxygen. The same areas are found by taking anatomical structures (course of vessels) as landmarks. A coordinate system allows us to determine the exact position of the cursor (area of measurement).

Detail magnification. Above: ophthalmoscopic image (DC); right: images of volume (Vol), flow (Flw), and velocity (Vel). The brightness of pixels in these images is in accordance with the values of volume, flow, and velocity, respectively. Right centre: flow image: square, variable in size (here 10 × 10 pixels), and possible locations for quantitative evaluation (r1–r4 = retina, p = optic nerve head); once the square is positioned at a certain location this location will be the same in all images (as demonstrated in r3 and in Fig 2) leading to values of volume, flow, and velocity of one location.

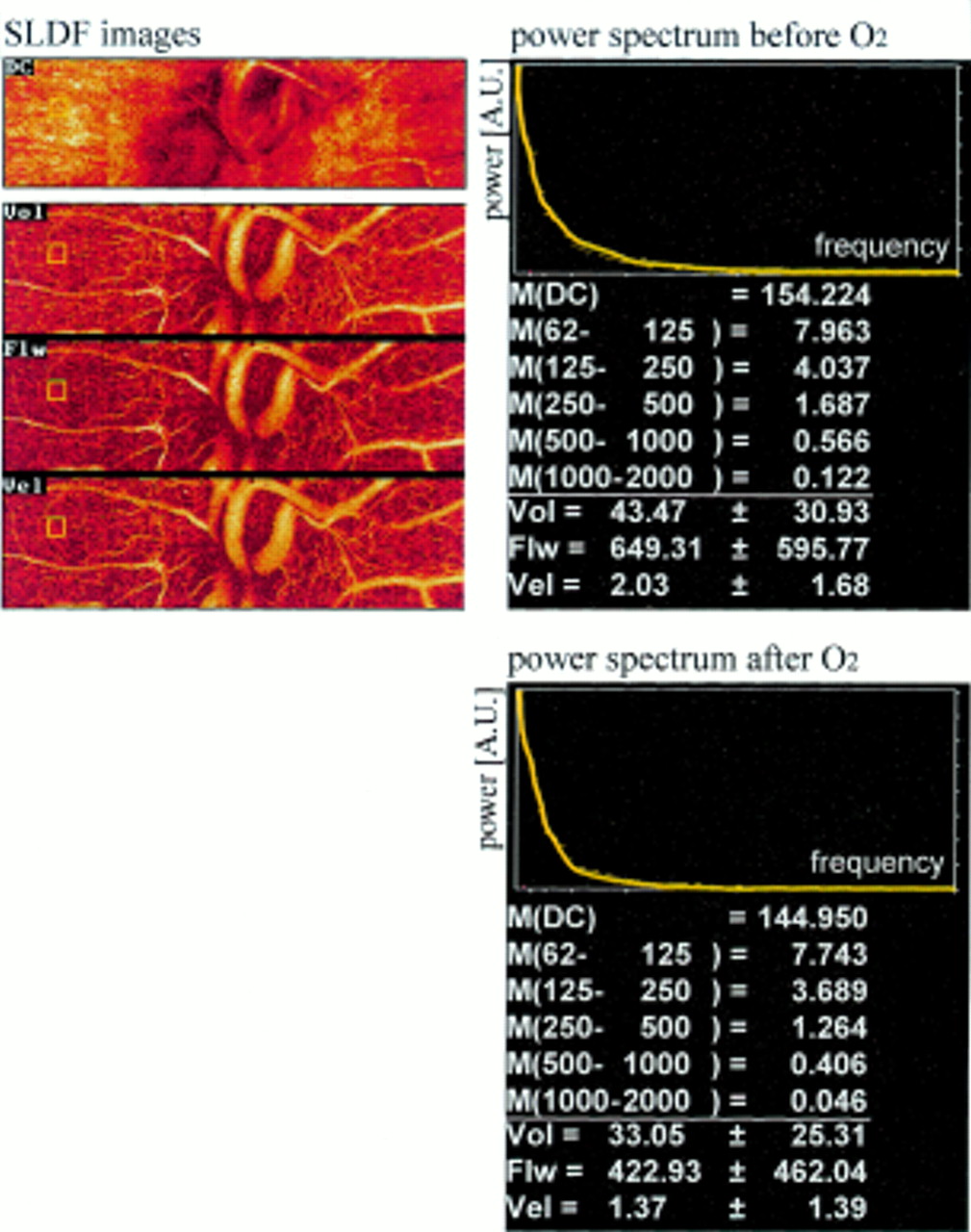
Scanning laser Doppler flowmetry images with power spectra before and after breathing oxygen. Above (from top to bottom): ophthalmoscopic image images volume (Vol), flow (Flw), velocity (Vel). Right, top: power spectra. Bottom: M(DC) = mean power of DC value (the DC value is proportional to the power of the reflected non-frequency shifted light). M(62–125) = mean power in the frequency ranges 62 Hz to 125 Hz lines below mean power in respective frequency ranges.
Ten right eyes of 10 young healthy non-smoking volunteers (mean age 26 (SD 3) years, range 23–32 years, four females, six males) and nine right eyes of nine young healthy smoking volunteers (mean age 26 (4) years, range 24–36 years, two females, seven males) were studied. None of the participating individuals suffered from ocular or systemic disease, and none of them took any medication regularly. The subjects were medical students from the local medical school or recruited from hospital staff. Informed consent was obtained from all participants according to the Helsinki declaration. All smokers had been smoking for at least 4 years (mean 8.2 (3.9) years) and smoked between 15 and 25 cigarettes per day. All participants were asked not to smoke or consume caffeine containing drinks for at least 4 hours before the measurements.
When the volunteers had arrived, brachial artery blood pressure and heart rate were determined. Then four measurements of each eye were taken. Only one measurement of the right eye was used for evaluation. The pupils of the subjects were not dilated. After application of 100% oxygen over a period of 5–6 minutes (6 litres per minute) to the sitting volunteer through a mask covering both mouth and nose the measurements were repeated in the same manner. After that blood pressure and heart rate were determined again. Each single measurement (scanning time) takes 2.048 seconds. If one considers the time needed for adjusting the camera and operating the computer (saving the acquired data), one complete single measurement takes 20 to 30 seconds. To ensure continuing influence of oxygen the mask was kept in place in front of the test person’s face during performance of the measurements.
The subjects were instructed to report any noticed effect of oxygen inhalation. One of the smoking volunteers reported headache 4 hours after the measurement, one other smoking volunteer reported dizziness right after oxygen breathing; otherwise, none of the test subjects noted any systemic reaction to the oxygen.
To assess the influence of carboxyhaemoglobin (CO-Hb) we drew venous blood from all participants and determined the CO-Hb levels.
For statistical evaluation we used a non-parametric Wilcoxon matched pairs signed ranks test.
Results
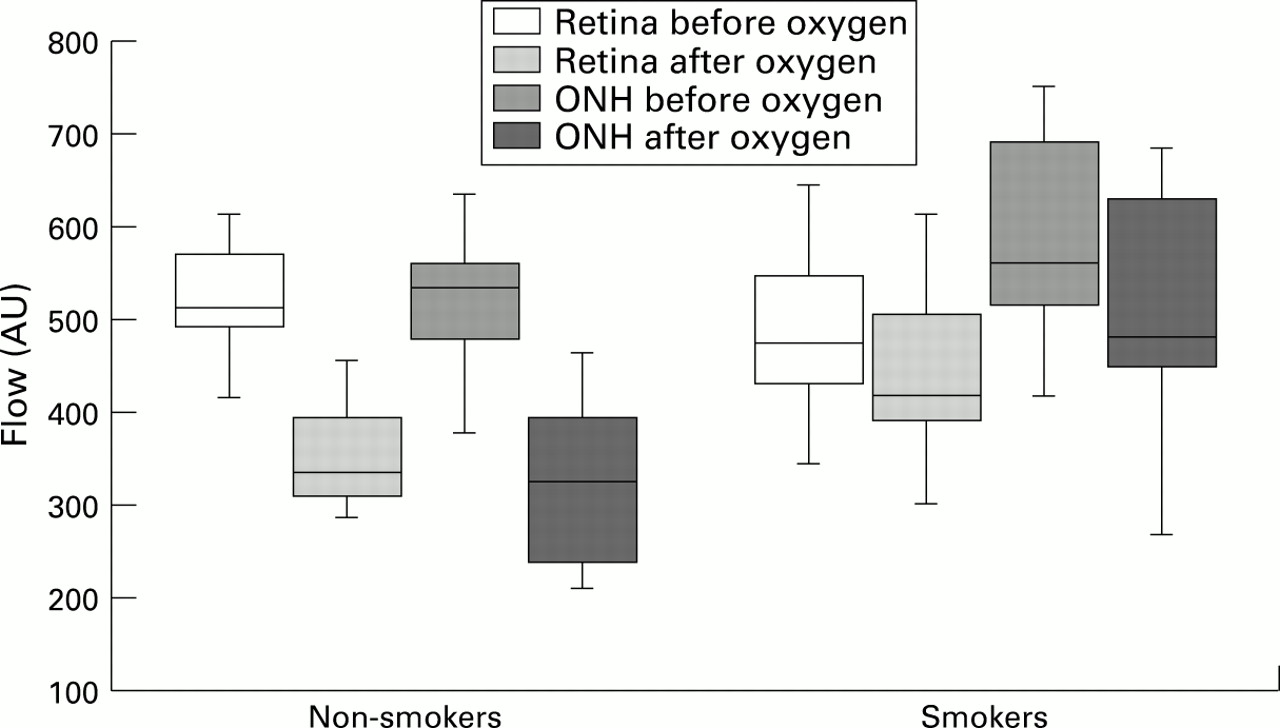
In both groups we found a significant reduction in retinal and optic nerve head volume and flow after breathing 100% oxygen. In the non-smoking group, retinal volume was reduced by 26% (p = 0.005) and flow by 33% (p = 0.005); and optic nerve head volume was reduced by 37% (p = 0.005) and flow by 37% (p = 0.005). In the smoking group retinal volume was reduced by 12% (p <0.008) and flow by 10% (p = 0.01); and optic nerve head volume was reduced by 15% (p <0.008) and flow by 13% (p <0.008) (see Table 1, see Figs 2 and 3). The difference in reactivity to oxygen breathing between smokers and non-smokers was highly significant (p <0.00001).
Changes in blood flow variables (SD) in smokers and non-smokers after breathing 100% oxygen
{kind=link}
{kind=link}
{kind=link}
Graph of reactivity changes (flow) as boxplot. Box contains 50% of the values falling between the 25th and 75th percentiles; line in the box indicates the median. Vertical lines extend from the box to the highest and lowest values (excluding outliers and extreme values). This resembles approximately two standard deviations.
In the non-smoking group the mean blood pressure was significantly decreased by 6% (5%) (p <0.02) after administration of oxygen. There was no significant change of the mean blood pressure after applying oxygen in the smoking group (p >0.1). In both groups we found a significant reduction of the systolic blood pressure under the influence of oxygen (−9% (6%), p =0.0004 in the non-smoking group, −6% (6%), p <0.002 in the smoking group; see Table 2). The diastolic blood pressure did not vary significantly in either of the two groups. However, the smoking volunteers showed an overall increased initial mean artery blood pressure (MBP) of 12% (MBP non-smokers 94.6 mm Hg, MBP smokers 108.1 mm Hg; p <0.002) before applying oxygen. The heart rate did not change significantly in either of two groups under the influence of oxygen. The initial variables, volume and flow, did not vary significantly between smokers and non-smokers (p ranging from 0.12 to 0.82). Among the smokers was one athlete (active climber) who, interestingly, showed a very good reactivity to oxygen. His retinal volume was reduced by 35% and flow by 35%. His optic nerve head volume was reduced by 49% and flow by 47%. So this reduction was above even the average of the non-smoking group.
Changes in systemic variables (SD) in smokers and non-smokers after breathing 100% oxygen
There was no correlation between the decrease in mean blood pressure and the decrease in retinal or optic nerve head blood flow in both groups (p>0.1).
In the non-smoking group none of the participants had a traceable CO-Hb level. In the smoking group two participants showed CO-Hb levels of 1.3% and 1.6%, respectively. Besides none of the smokers had a traceable CO-Hb level.
Discussion
We found that retinal and papillary blood flow is reduced under the effect of oxygen, and that this response induced by oxygen is impaired in smokers.
REACTION OF RETINAL AND PAPILLARY BLOOD FLOW TO OXYGEN IN NORMALS
Different methods have been used to investigate the effect of breathing pure oxygen on retinal vasculature—for example, laser Doppler velocimetry,2 12 fluorescein angiograms1 2 for assessment of vessel diameters, and the blue field entoptic phenomenon.13 All authors agree about the vasoconstricting effect leading to a decrease in vessel diameter and reduction of blood flow. The reductions found in retinal blood flow after breathing oxygen vary from 35% to 64%.12 In our study breathing pure oxygen led to a reduction of retinal blood flow between 26% and 33% in non-smokers. The reduction of optic nerve head blood flow was between 32% and 37% in non-smokers. There was no significant difference between the retinal and papillary reaction except for the variable volume (−26% in the retina, and −37% in the optic neve head, p = 0.02). This non-significant difference might be due to measuring only the superficial neuroretinal rim of the optic nerve, which is also supplied by the central retinal artery.
For interpretation of these data two possible reasons for the reduction of blood flow caused by hyperoxia have to be considered—the systemic responses to oxygen breathing and the local vasoconstricting effect of oxygen. In the non-smoking group we found a significant reduction of the mean arterial blood pressure (−6%, p <0.02) leading to a decreased perfusion pressure in the eye. One could presume that the decreased perfusion pressure in the non-smoker’s eyes is responsible for a decreased perfusion after breathing pure oxygen. However, a reduction in MBP of only 6% seems unlikely to produce a blood flow reduction of over 30%. According to the equation
Our results show a lower reduction of retinal and optic nerve head perfusion upon breathing oxygen than previous studies. A reason might be the application of different measuring methods and locations.
DIFFERENT REACTIONS TO OXYGEN IN SMOKERS
We found that smokers showed a significantly altered reaction of retinal and optic nerve head blood flow to breathing pure oxygen.
Previous studies3 using laser Doppler velocimetry have shown that acute smoking causes a reduction of retinal blood flow. Robinson et al, however, reported an increase in macular leucocyte velocity immediately after smoking a cigarette14using the blue field entoptic phenomenon. In these studies only the acute effect of smoking (in habitual smokers) was examined. Thus, possible long term effects of smoking on the retinal capacity of autoregulation have not been illuminated by these studies. In our study the reactivity to oxygen breathing among smokers was significantly decreased. One may presume that an increased CO-Hb level in smokers is responsible for that altered reactivity. However, other than expected none of the participating smokers showed increased CO-Hb levels. The reason might be that all smokers were asked not to smoke 4 hours before the measurements. CO-Hb is said to have a half life of approximately 3 hours in normal air (21% oxygen) and of approximately 45 minutes when breathing pure oxygen.5 CO-Hb levels were determined after the experiment, so the inhalation of oxygen might have caused a more rapid elimination of carbon monoxide. Accordingly a possible effect of CO-Hb levels cannot be definitively excluded.
Again the different systemic response in smokers and non-smokers has to be taken into consideration. As mentioned above there was no significant reduction of the mean arterial blood pressure in the smoking group. Since there was no correlation between intraindividual values of Δ blood pressure and Δ flow in either of the groups we believe this factor to be unlikely for the different response to oxygen breathing.
Nicotine causes a permanent vasoconstriction due to an excitation of sympathetic ganglia and stimulation of the adrenal gland with resulting elevated excretion of catecholamines.15However, the initial blood flow rates did not vary significantly between smokers and non-smokers. Long term effects of nicotine might also cause altered vascular regulation. So long term effects of nicotine on vascular regulatory processes are more likely to be responsible for the reduced reactivity in smokers rather than elevated CO-Hb levels. However, this cannot be clarified definitively.
SMOKING AND PATHOLOGICAL CONDITIONS IN THE EYE
Owing to the aforementioned conditions in smokers long term smoking seems to cause a change of the retinal and optic nerve head vascular regulation. In the Beaver Eye Study16 it was suggested that there is no difference between smokers and non-smokers with regard to the frequency of glaucoma. Morgado et alfound a loss of oxygen reactivity after smoking in diabetics.3 Some authors consider smoking a risk factor for the progression of diabetic retinopathy17; others regard smoking as not likely to be a risk factor for diabetic retinopathy.18 Thus it remains questionable whether long term smoking contributes to general pathological conditions of the retina and optic nerve head.
Conclusion
These results indicate that hyperoxia leads to a decrease in capillary blood flow of the retina and optic nerve head secondary to vasoconstriction, and that smokers do not respond to oxygen breathing as non-smokers do. Smokers show a reduced reactivity to oxygen compared with non-smokers. The regulatory capacity in the retinal microcirculation of smokers seems to be changed. In summary, one might conclude that the observed findings are the result of long term effects of nicotine on vascular regulation processes rather than effects of carboxyhaemoglobin.
Acknowledgments
Supported by Deutsche Forschungsgemeinschaft (DFG) Mi 320/2-2.