Article Text

Abstract
AIMS/BACKGROUND Ocular Chlamydia trachomatis infection in the west occurs as ophthalmia neonatorum, acquired from the mother, or adult paratrachoma which is also associated with current genital tract infection. Accurate rapid laboratory diagnosis facilitates management, but the relative merits of antigen detection or DNA amplification tests are unresolved.
METHODS A polymerase chain reaction (PCR) test was developed which amplified part of the plasmid shared by all the serovars of C trachomatis. Conjunctival swabs were tested using an in house immune dot-blot test (IDBT) for chlamydial lipopolysaccharide antigen, a commercial direct fluorescent antibody (DFA) test for chlamydial elementary bodies, and the PCR (DNA extracted using guanidinium lysis buffer).
RESULTS The PCR achieved a detection limit of 100 plasmid copies (10 elementary bodies). In a combined retrospective and prospective clinical evaluation, the PCR and IDBT gave identical results with 21 positive and 57 negative eye swabs. However, interpretation of the DFA test required meticulous examination of the stained smear, sometimes by two microscopists.
CONCLUSIONS The PCR is likely to play an increasing role in the diagnosis of ocular C trachomatisinfection because of its excellent sensitivity and specificity.
- Chlamydia
- diagnosis
- DNA amplification
- direct fluorescent antibody test
Statistics from Altmetric.com
Chlamydia trachomatis causes three ocular diseases: trachoma in conditions of poverty, deficient sanitation, and poor hygiene; adult inclusion conjunctivitis, also called paratrachoma, in sexually active young adults following transfer of bacteria from the genitalia to the eye; and ophthalmia neonatorum acquired from the mother.1 Only the latter two conditions are seen in developed countries such as the UK. Paratrachoma begins as follicular conjunctivitis, and if not treated persists though does not lead to blindness.1 It can, however, be confused clinically with other causes of chronic conjunctivitis. A minimum of 70% of women (and possibly all) with chlamydial conjunctivitis are estimated to have genital C trachomatis infection, mostly asymptomatic but possibly associated with diminished fertility.2-5Ophthalmia neonatorum presents as swelling of the eyelid, and progresses to purulent inflammation of the conjunctiva. If untreated, the disease can persist for up to 1 year, and, though usually self limiting, may result in blindness due to secondary bacterial infections. Infected neonates often develop pharyngitis, otitis media, and pneumonia due to chlamydia.2 Both the mother and the baby should be treated.2
Accurate rapid laboratory diagnosis is crucial to the successful management of adult and neonatal chlamydial conjunctivitis.6-13 Culture of eye swabs on cycloheximide treated McCoy cells was the ‘gold standard’ technique, though, owing to its slowness, complexity, and susceptibility to microbial overgrowth and cell toxicity, it has been largely replaced by the direct fluorescent antibody (DFA) test for elementary bodies14and/or enzyme immunoassay (EIA).15 The DFA test shows a sensitivity of 95–100% in comparison with culture in neonatal eye infections.14 None the less, laborious microscopic examination of each specimen by highly skilled and experienced personnel is recommended,16 and the assay is only suitable for the examination of small numbers of specimens. In contrast, EIAs are ideal for testing large numbers of samples, achieve sensitivities of 90% in comparison with culture, but may be less sensitive than DFA and are prone to give false positive reactions.14 15 In this laboratory we use a novel, simple, immune dot-blot test (IDBT) for detection of chlamydial lipopolysaccharide (LPS) antigen which gives a sensitivity of 92% with genital swabs17 and twice as many positive results with eye swabs18 in comparison with culture. With the advent of the polymerase chain reaction (PCR), assays for chlamydia more sensitive than culture or even DFA have been developed.19 In this study, we compare DFA, IDBT, and the PCR for the diagnosis of ocular C trachomatis infection in a combined retrospective and prospective study.
Materials and methods
CLINICAL SAMPLES
Cotton tipped conjunctival swabs for investigation of suspected chlamydial conjunctivitis were collected in 1 ml of sucrose phosphate (2SP) transport medium (8 mM KH2PO4, 12 mM K2HPO4, and 0.2 M sucrose) supplemented with antibiotics (amphotericin B 2.5 μg/ml, streptomycin 50 μl/ml, and vancomycin 100 μg/ml20). Each sample (100 μl volume) was prepared for PCR testing by 10 minutes’ incubation at room temperature with 400 μl guanidinium isothiocyanate lysis buffer (4 M guanidinium isothiocyanate, 0.5% N-lauryl Sarcosine, 1 mM dithiothreitol, 25 mM sodium citrate, 20 μg glycogen) and then precipitation with 125 μl cold 100% isopropanol. The samples were centrifuged for 10 minutes at 14 000 g at 4°C. The isopropanol was removed and the pellet washed by the addition of 250 μl 70% ethanol. The samples were centrifuged as above, the ethanol was removed and the dried pellet dissolved in 10 μl sterile double distilled water.21
CONTROL DNA SAMPLES
Crude DNA extracts from turbid suspensions of Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli, Candida albicans organisms, cycloheximide treated sonicated McCoy cells infected with C trachomatis serotype E (T181) (4 × 106 inclusion forming units/ml), and 105 cells infected with herpes simplex virus (HSV) type 1 or adenovirus type 2 were prepared by centrifugation of a 100 μl sample at 13 000g, and incubation of the resuspended pellet in proteinase K (250 μg/ml) for 3 hours at 56°C and then 95°C for 30 minutes to inactivate the enzyme. Cloned caesium chloride purified C trachomatis L2 plasmid DNA (pCtL2)22 was used as the positive control in the PCR.
IMMUNE DOT-BLOT TEST
Conjunctival swab transport medium (0.4 ml) was treated with 250 μg/ml proteinase K for 30 minutes at 56°C principally to digest staphylococcal protein A, a cause of false positive reactions in the IDBT.17 The enzyme was inactivated at 95°C for 15 minutes, and the sample added to a nitrocellulose membrane in a dot-blot manifold. The blotted antigen was detected with J12, a monoclonal antibody which reacts with a Chlamydia specific epitope on the LPS,23 radiolabelled with 125I using the method of Hunter et al. 24 Each 96 well membrane was reacted with 33 KBq of 125I labelled antibody and bound antibody detected by autoradiography. The sample was considered positive if the intensity of the darkened circle on thex ray film exceeded that formed by 100 inclusion forming units of C trachomatis serotype E.17 18 This test was performed on the open bench in our multiuser diagnostic laboratory.
POLYMERASE CHAIN REACTION
Two buffers were used successively in the PCR. Buffer 1 gave final concentrations in the reaction mixture of 67 mM TRIS-HCl, 16 mM (NH4)2SO4, 4 mM MgCl2, 1 mg/ml bovine serum albumin, 0.072% v/v 2-mercaptoethanol, 200 μM each deoxynucleoside triphosphate (dNTP), 1 unit (U) Taq DNA polymerase (Boehringer, Mannheim, Germany), and 0.2 μM each primer.26 The final concentrations achieved with buffer 2 were 10 mM TRIS-HCl, 50 mM KCl, 1.5 mM MgCl2, 200 μM each dNTP, 15 U Taq DNA polymerase and 0.1 μM each primer.17 The primers CtC (5′-AAG ATACGTGAATTCTTAAGTT-CGGTC-3′) and CtD (5′-TAATTGATCCA-AACT CTGACTTTCCTC-3′) hybridise to regions 5331–5357 and 5788–5762 on the chlamydial plasmid25 and amplify a 457 base pair fragment.26 Each 100 μl reaction mixture included 10 μl DNA extract, sterile distilled water (SDW) as a negative control, or SDW containing 1000 copies pCt L2 as a positive control. The thermal cycles were as previously described26; DNA was amplified by one cycle of 94°C for 7 minutes, 55°C for 1 minute, and 72°C for 1 minute followed by 49 cycles of 94°C for 1½ minutes, 55°C for 1 minute, and 72°C for 1½ minutes. The PCR products were analysed by electrophoresis through 1% agarose gels in parallel with a 1 kb ladder (Gibco-BRL, Paisley, Scotland).
DIRECT FLUORESCENT ANTIBODY TEST
The specimen (100 μl) was centrifuged at 13 000 gfor 5 minutes and the resultant pellet resuspended in 10–20 μl phosphate buffered saline (PBS). Five μl of the suspension were placed onto each of two wells of a multiwell glass slide, air dried, and fixed in methanol. After staining with a minimum volume of fluorescein isothiocyanate conjugated monoclonal antibody to the chlamydial major outer membrane protein (Syva, San Jose, USA) by incubation at 37°C for 30 minutes, and then washing with PBS, the smears were mounted in PBS/glycerol (50/50) and examined by ultraviolet microscopy.
Results
SENSITIVITY AND SPECIFICITY OF THE PCR
With buffer 1, the PCR detection limit was 1000 copies of C trachomatis plasmid DNA or 400 inclusion forming units ofC trachomatis. Use of buffer 2 increased the sensitivity 10-fold to 100 copies of plasmid DNA. All subsequent DNA amplifications were done using buffer 2. No CtC/CtD amplification product was generated with DNA extracted from S aureus, P aeruginosa, E coli, C albicans, HSV type 1, or adenovirus type 2.
RETROSPECTIVE EVALUATION
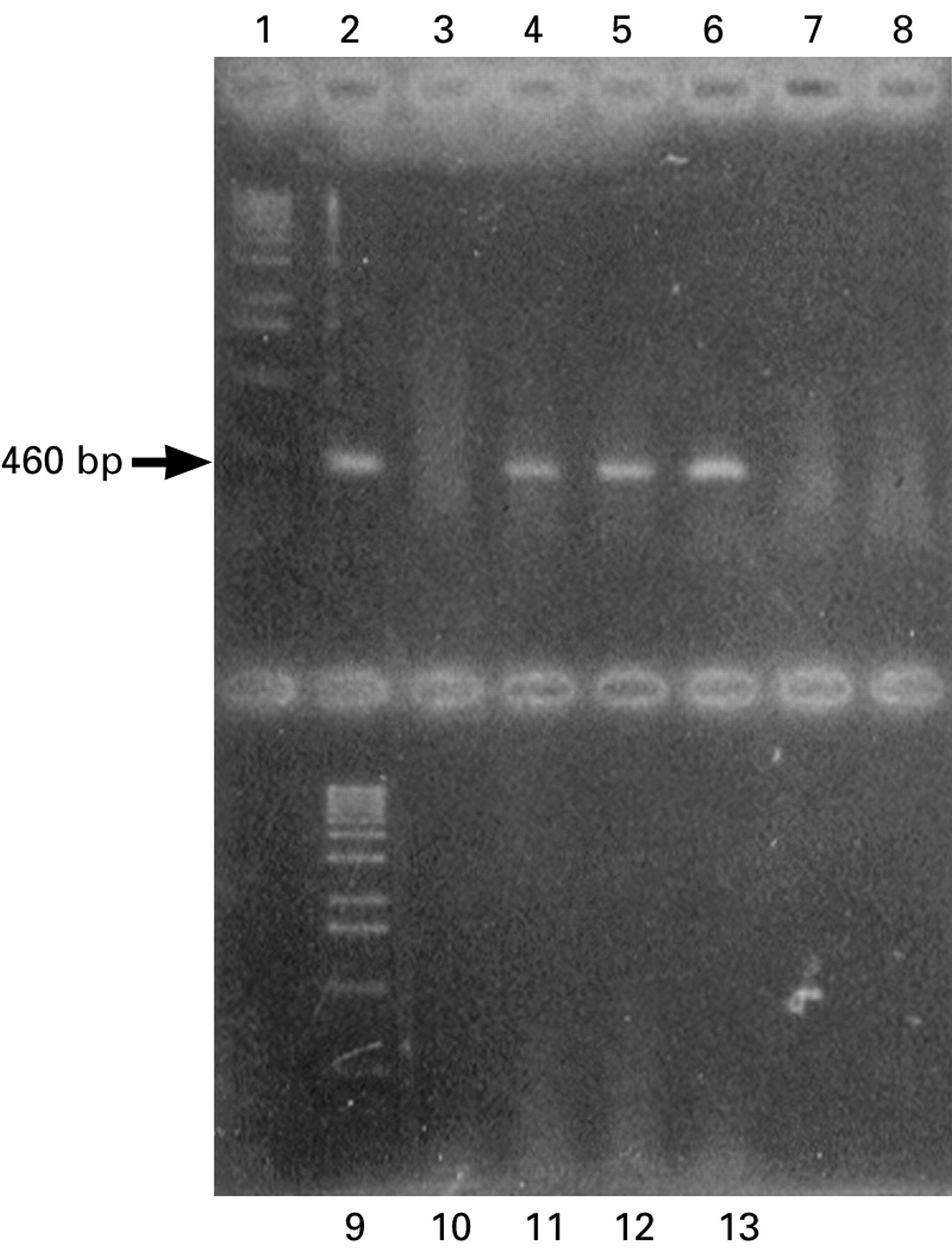
Thirty seven eye swabs in transport medium which had been stored at −70°C for up to 1 year following completion of the IDBT were examined using PCR. Thirty of these swabs were also tested by DFA test. All assays were done blind—that is, PCR testing without knowledge of IDBT results and DFA testing without knowledge of PCR or IDBT results. Sixteen samples were positive for chlamydia in both the IDBT and the PCR, and 21 specimens were negative in these two tests (for example of PCR results, see Fig 1). Identical results were obtained in the DFA assay for all 16 of the positive and 14 of the negative conjunctival swabs.

{kind=link}
Polymerase chain reaction using Chlamydia trachomatis plasmid primers CtC and CtD on conjunctival swab DNA extracts. Lanes 1 and 9, 1 kb ladder (Gibco-BRL); lane 2, positive control (1000 copies pCtL2); lane 3, negative control (sterile distilled water); lanes 4–6, immune dot-blot test (IDBT) positive eye swabs; lanes 7, 8, and 10, IDBT negative eye swabs; lanes 11–13, TRIS-EDTA, a control for cross contamination.
Interpretation of the DFA test required examination of the smears by two microscopists, both to identify correctly all IDBT positive and negative samples (four were initially misclassified as negative by one observer) and to determine the consensus result when initial screening was inconclusive (Table 1).
Results of direct fluorescent antibody (DFA) test on 30 conjunctival swabs read by two microscopists
PROSPECTIVE EVALUATION
Forty one conjunctival swabs were tested prospectively on the day of receipt by IDBT and within 1 week by PCR; five were positive and 36 negative in both assays. Combination of the data from the retrospective and prospective evaluations established that the PCR achieved a sensitivity (21/21), a specificity (57/57), a positive predictive value (21/21), and a negative predictive value (57/57) that were all 100% if the IDBT result was considered accurate.
Discussion
Our data confirmed the interpretative difficulties previously documented with the chlamydial DFA test.16 Only meticulous time consuming scrutiny of the smear, sometimes by two microscopists, guaranteed accurate results in this test.
In our laboratory, the IDBT replaced culture in cycloheximide treated McCoy cells for diagnosis of ocular C trachomatisinfection because the IBDT was more sensitive than culture with conjunctival swabs.18 The identical dot-blot, DFA, and PCR results obtained in this study proved the excellent sensitivity and specificity of our in house test for chlamydial LPS. This specificity was achieved following introduction of sample pretreatment with proteinase K, which destroyed staphylococcal protein A, a known cause of false positive results in the assay.17 Also, proteinase K treatment possibly released LPS from contaminating proteins to make the antibody binding sites more accessible and the test more sensitive. Our IDBT for adenovirus hexon protein precluded specimen pretreatment with proteinase K, and gave an unacceptably high false positive rate27 and a lower sensitivity than adenovirus PCR when testing eye swabs.28 Commercial EIAs for chlamydia give false positive readings,14 15 perhaps because proteinase K digestion of contaminating proteins cannot be included.
The difference in the detection limit of the PCR using buffer 1 forC trachomatis (400 inclusion forming units) or purified plasmid pCtL2 (1000 copies) reflected the 10 plasmid copies found in each chlamydial elementary and reticulate body.22 29 This high copy number and the presence of the plasmid in all serovars of C trachomatis 22 led us to choose plasmid rather than chromosomal DNA as the molecular target for our PCR. Amplification of chlamydial plasmid rather than major outer membrane protein gene sequences enhanced the sensitivity of detection of cultured organisms by a factor of 4.19 A possible disadvantage of chlamydial plasmid based amplification is the potential occurrence of plasmid-less strains of C trachomatis which could result in a false negative result by a PCR with a plasmid target.30 31 However, despite much speculation strains ofC trachomatis which do not contain plasmids have never been isolated and cultured and if they do exist they probably occur at a very low frequency. Switching to a simple buffer (buffer 2) increased the sensitivity to that achieved previously only with the addition of Southern blot hybridisation for the identification of PCR products.26
The PCR sensitivity achieved in this analysis (100 plasmid copies, equivalent to 10 elementary bodies) was 10-fold lower than that reported previously using different primers also targeting the chlamydial plasmid.32 Nucleic acid amplification using the latter oligonucleotides gave false positive results as a result of airborne contamination which was only eliminated following the development of a closed system for carrying out the PCR.32In contrast, our PCR gave no false positive results despite the handling of specimens on the open bench during the IDBT. Published PCRs for the chlamydial plasmid achieved higher diagnostic sensitivity for ocular infection than EIA, culture, or the DFA test.34 35The failure to document differences in performance between the latter assay, the IDBT, and our PCR for the C trachomatis plasmid probably reflected the similarity of the detection limits in the two in house tests (100 inclusion forming units or 10 elementary bodies, respectively).
In our laboratory, continued use of the IDBT for initial screening of eye swabs for C trachomatis infection was validated. In laboratories without access to the IDBT, the DFA test could be recommended only if small numbers of specimens were submitted and all were examined by skilled and experienced microscopists. Though commercial EIAs have the advantages of low cost, suitability for testing large numbers of specimens, and availability of reagents subject to external quality control, the false negative and false positive results generated are a serious disadvantage when effective treatment of chlamydial eye disease is available, and failure to treat could lead to chronic conjunctivitis in babies or infertility in adult women.2 Also, inaccurate diagnosis of C trachomatis infection in a patient being investigated for conjunctivitis and not a sexually transmitted disease could lead to litigation. The excellent performance of the chlamydial plasmid PCR none the less reinforced the potential role of DNA amplification assays for diagnosis of ocular chlamydial infection. Nucleic acid contamination of specimens during routine diagnostic testing was not detected. The commercial Roche Diagnostic Systems C trachomatis plasmid PCR, which gave similar results to the DNA amplification assay described here with oropharyngeal swabs,26 proved only marginally less sensitive than culture with conjunctival swabs,35 and includes a proprietary system designed to avoid false positive results due to contaminating amplicons from previous PCRs. Where the IDBT is not available, the arguments in favour of using the in house or commercial PCR for detection of C trachomatis in eye swabs appear to be strong. The successful use in our C trachomatis plasmid PCR of the simple buffer also employed in sensitive single target adenovirus28 and duplex adenovirus-HSV PCRs36could mean that multiplex PCRs may be feasible for the diagnosis of ocular surface infections where Chlamydia, adenovirus, and HSV are all considered possible causative agents.