Article Text

Abstract
AIMS The reliability of scanning laser ophthalmoscope (SLO) microperimetry in differentiating full thickness macular holes from macular pseudoholes and impending macular holes was evaluated.
METHODS 106 eyes with the clinical diagnosis of full thickness macular holes, macular pseudoholes, and impending (stage 1) macular holes were examined for the presence of deep or relative scotoma using SLO microperimetry. The relation between these scotomas and the clinical diagnosis was studied.
RESULTS Deep and relative scotomas were detected in all 57 eyes with clinically defined full thickness macular holes. In contrast, among 49 eyes diagnosed with macular pseudoholes or impending macular holes, no deep and only one relative scotoma was observed. The sensitivity of the presence of a deep scotoma as an indicator of the clinical diagnosis of a full thickness macular hole was 100% (57 of 57), and the specificity was 100% (49 of 49). The sensitivity of the presence of a relative scotoma was 100% (57 of 57) and the specificity was 98.0% (48 of 49).
CONCLUSION With SLO microperimetry, full thickness macular holes can be precisely and objectively distinguished from other conditions that mimic macular holes.
- macular holes
- pseudoholes
- scanning laser ophthalmoscope
- microperimetry.
Statistics from Altmetric.com
Full thickness macular holes are a common cause of visual loss in middle aged and elderly patients. They usually result in a visual acuity of between 20/80 and 20/200.1-4 The pathogenesis of this disease is hypothesised to be a result of tangential traction exerted by a thin layer of cortical vitreous. Continued traction causes the macular hole and cuff to enlarge with a progressive decrease of visual acuity in most cases.3-7
Recently, surgical techniques have been developed to release the tangential traction, and a macular hole has come to be regarded as a treatable condition. Several studies demonstrated the success of surgical treatment in this disease.8 9 Because of the increased surgical intervention for patients with full thickness macular holes, accurate diagnosis of this disease has become extremely important.
Several conditions resemble macular holes, including epimacular membranes with pseudoholes, impending macular holes, age-related macular degeneration, vitreomacular traction syndrome, and others. In particular, epimacular membrane with pseudoholes and impending (stage 1) macular holes are often misdiagnosed as full thickness macular holes on conventional examination.10-14 Since the treatment of these disorders is often quite different from that of full thickness macular holes, and ranges from conservative to invasive, a reliable means of distinguishing them from macular holes is sorely needed. We used the scanning laser ophthalmoscope (SLO), a device that has been applied to macular diseases in the past,15 to examine patients with clinical macular holes and other lesions with a similar clinical appearance. The purpose of this study was to determine if SLO microperimetry can reliably differentiate full thickness macular holes from macular pseudoholes and impending macular holes.
Patients and methods
A total of 106 eyes of 94 consecutive patients who were diagnosed with full thickness macular holes, impending macular holes, or macular pseudoholes by the five members of the retina faculty at a university teaching hospital from October 1994 to September 1995 was studied. The best corrected visual acuity was measured by ophthalmic technicians in standard fashion. All patients received detailed fundus examinations using slit-lamp biomicroscopy with a 90 dioptre lens. In most patients, other ocular examinations including fluorescein angiography, the slit-beam test (Watzke–Allen sign), Amsler grid testing, and automated static threshold perimetry using the Humphrey field analyser program 10-2 (Allergan-Humphrey Medical Instruments, Irvine, CA, USA) were also performed. The diagnosis was made based on the results of these conventional examinations. The cases diagnosed by fluorescein angiography as a choroidal neovascularisation, a cystoid macular oedema, or an idiopathic juxtafoveal telangiectasis were excluded from our study. Idiopathic macular holes were graded according to the criteria described by Gass.3 After an initial diagnosis was assigned, SLO microperimetry was performed.
We used a confocal scanning laser ophthalmoscope (Rodenstock, Germany), equipped with a static microperimetry program. Microperimetry with the SLO enables fundus controlled perimetry to be performed under direct observation of the fundus by infrared laser.15 16 Using this instrument, we could precisely stimulate retinal loci with the beam of the helium–neon laser. In this study, we used a stimulus size equivalent to a Goldmann I test spot, with a beam diameter of 27.5 μm illuminating a 0.925 degree spot on the retina.17 The duration of the stimulus was 0.1 seconds. Two stimulus intensities were used for each eye; 0 dB to detect a deep scotoma and 10 dB to detect a relative scotoma. Using these stimuli, we tried to detect scotomas on and around the macular lesion under direct observation with the infrared laser. A paracentral fixation target was chosen using four fixation targets. Patients were asked to gaze at the centre of the four crosses, which facilitated performance of microperimetry in patients with poor fixation. The intensity of background illumination was 10 cd/m2. During each examination, we stimulated over 25 points in an area of approximately 5 degrees in diameter around the fixation point. A scotoma was defined if a patient failed to detect three or more closely adjacent points during examination. If these unseen points were found using the 0 dB stimulus, it was termed a deep scotoma, and if found during testing with the 10 dB stimulus, it was termed a relative scotoma.
We divided all patients into two diagnostic groups based on the clinical diagnosis. Group 1 included patients with full thickness macular holes (idiopathic stage 2, 3, and 4 holes). Group 2 consisted of patients with diagnoses other than full thickness macular holes including impending (stage 1) holes and macular pseudoholes. The relation between these diagnostic groups and the results of SLO microperimetry were studied.
Eighty five of 106 eyes had been examined initially by ophthalmology residents or a referring ophthalmologist before examination by the members of the retina faculty. The relation between the initial clinical diagnosis and the diagnosis assigned by the retina faculty was examined in light of the results of SLO microperimetry.
In nine cases, the initial diagnosis was in question, and there were differences of opinion among members of the retina faculty. We noted these eyes to be ‘atypical’ cases. These eyes had repeated examinations for 1 year or longer and were assigned to group 1 or group 2, based on consensus of the faculty. Six of nine eyes underwent vitrectomy for a full thickness macular hole or epimacular membranes, and the final diagnoses were confirmed during surgery. We used the results of SLO microperimetry at first visit of the patients to compare with the final diagnosis. The clinical features of these atypical cases were examined.
Results
We examined 71 females (81 eyes) and 23 males (25 eyes). The mean age was 61.4 years (range 36–77 years). Of 106 eyes, there were 57 eyes with full thickness macular holes (group 1), including eight stage 2 holes, 24 stage 3 holes, and 25 stage 4 holes. The remaining 49 eyes (group 2) had other diagnoses, including 36 macular pseudoholes and 13 impending macular holes. Macular pseudoholes included 29 epimacular membranes, three lamellar macular holes, one vitreomacular traction syndrome, and others.
Table 1 shows the baseline characteristic of the two groups. The two groups were similar in age and in sex distribution. Visual acuity of patients who were diagnosed with full thickness macular hole (group 1) ranged from 20/20 to 20/800 (median 20/100). Visual acuity of patients with macular pseudoholes or impending holes (group 2) ranged from 20/15 to 20/100 (median 20/25).
Characteristics on baseline examination
Table 2 shows the diagnoses made by ophthalmology residents or referring ophthalmologists. Of the 45 eyes in group 1 (full thickness holes), six eyes were misdiagnosed as having macular pseudoholes or impending macular holes. Of the 40 eyes in group 2, 15 eyes were misdiagnosed as having full thickness macular holes. The sensitivity of the diagnoses made by these physicians was 86.7% (39 of 45) and the specificity was only 62.5% (25 of 40).
Diagnosis by residents or referring ophthalmologists versus diagnosis by retina faculty
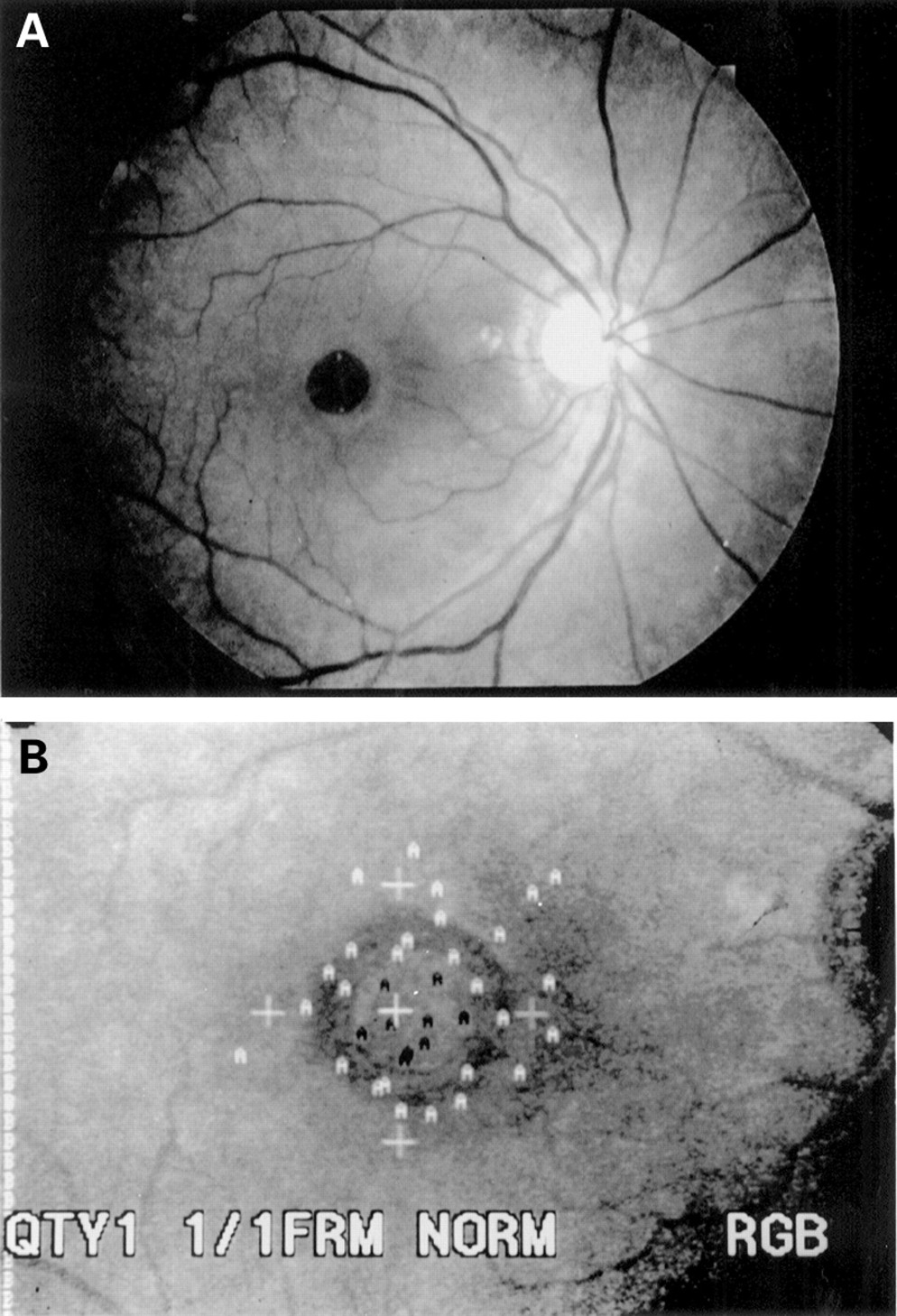
Table 3 shows the presence of scotomas in the two groups. Of the 57 eyes in group 1, all eyes showed deep (0 dB) and relative (10 dB) scotomas (Fig 1). In contrast, none of 49 eyes in group 2 had a deep scotoma by microperimetry (Fig 2). Only one eye in group 2 showed a relative scotoma.
Outcome characteristics of SLO microperimetry
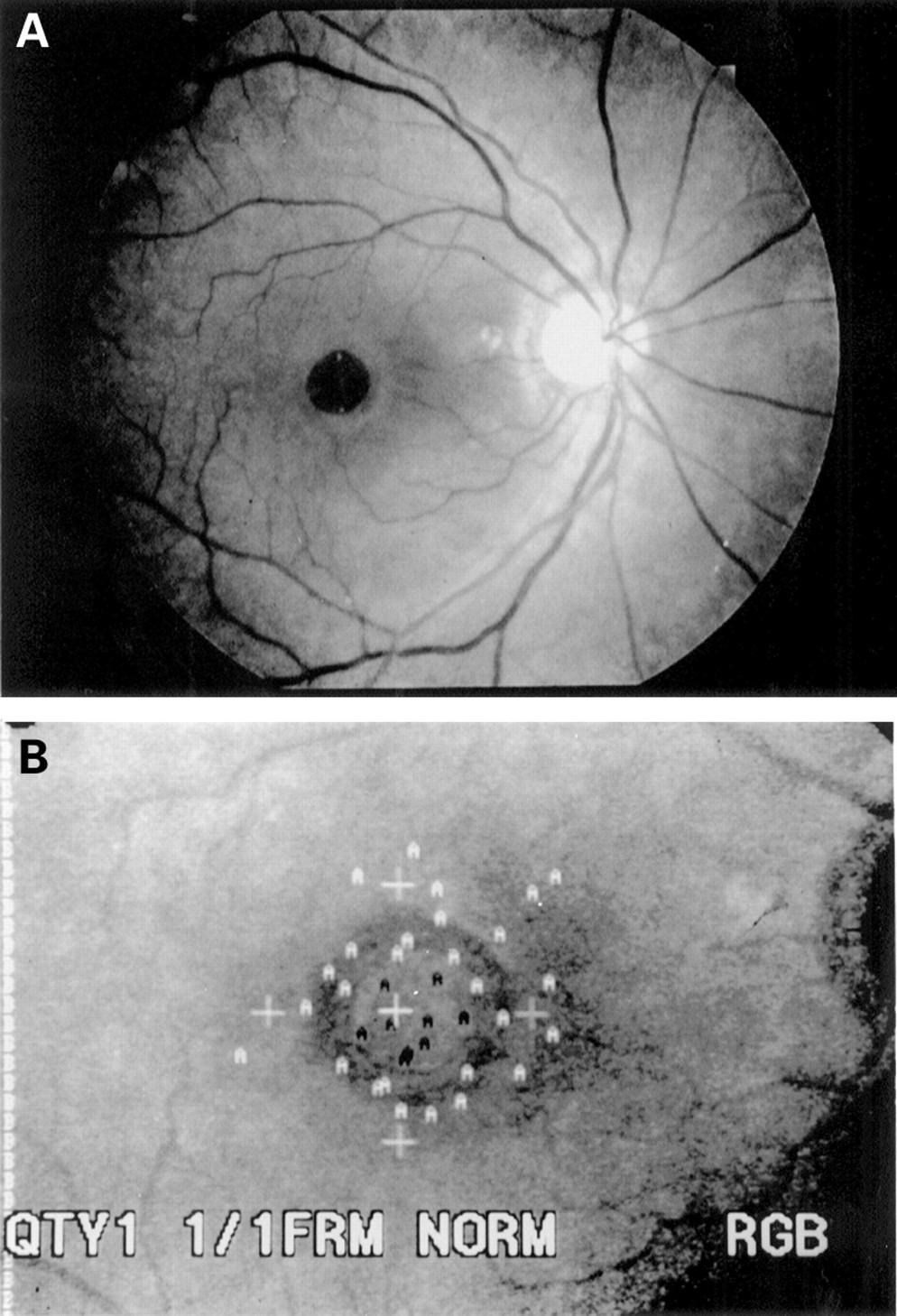
(A) Fundus photograph of a patient with a full thickness macular hole. (B) Scanning laser ophthalmoscope microperimetry with a 0 dB stimulus from the same patient. The white ‘A’s indicate points seen by the patient, and black ‘A’s correspond to points not seen (deep scotoma). Deep scotoma points were detected within the hole.

(A) Fundus photograph of a patient with a macular pseudohole. (B) Scanning laser ophthalmoscope microperimetry with a 10 dB stimulus from the same patient. A relative scotoma was not detected.
When the presence of a deep scotoma was used as the criterion for the diagnosis of a full thickness macular hole, the sensitivity of this test was 100% (57 of 57) and the specificity was 100% (49 of 49). When the presence of either a deep or relative scotoma was used for the diagnosis, the sensitivity was 100% (57 of 57) and the specificity was 98.0% (48 of 49).
ATYPICAL CASES
Table 4 summarises nine atypical cases in which the diagnosis was felt to be especially difficult. All eyes were observed for 12 months or longer. Six of nine eyes underwent pars plana vitrectomy and the diagnosis was confirmed during surgery in these eyes. The remaining three eyes had a consensus diagnosis assigned at the time of the last follow up visit. The final diagnosis in this group was full thickness macular holes in four eyes, epimacular membranes with pseudoholes in three eyes, and impending macular holes in two eyes.
Clinical features of nine atypical cases
On Amsler grid testing, none of four (0%) atypical full thickness macular holes demonstrated scotomas, whereas two of five (40%) atypical impending macular holes and macular pseudoholes demonstrated scotomas. All patients with atypical cases complained of metamorphopsia, whereas none of these patients reported a complete break in the slit-beam on Watzke–Allen testing. Central thinning of the beam was reported by three of four (75%) patients with atypical full thickness macular holes and three of five (60%) patients with atypical impending macular holes and macular pseudoholes.
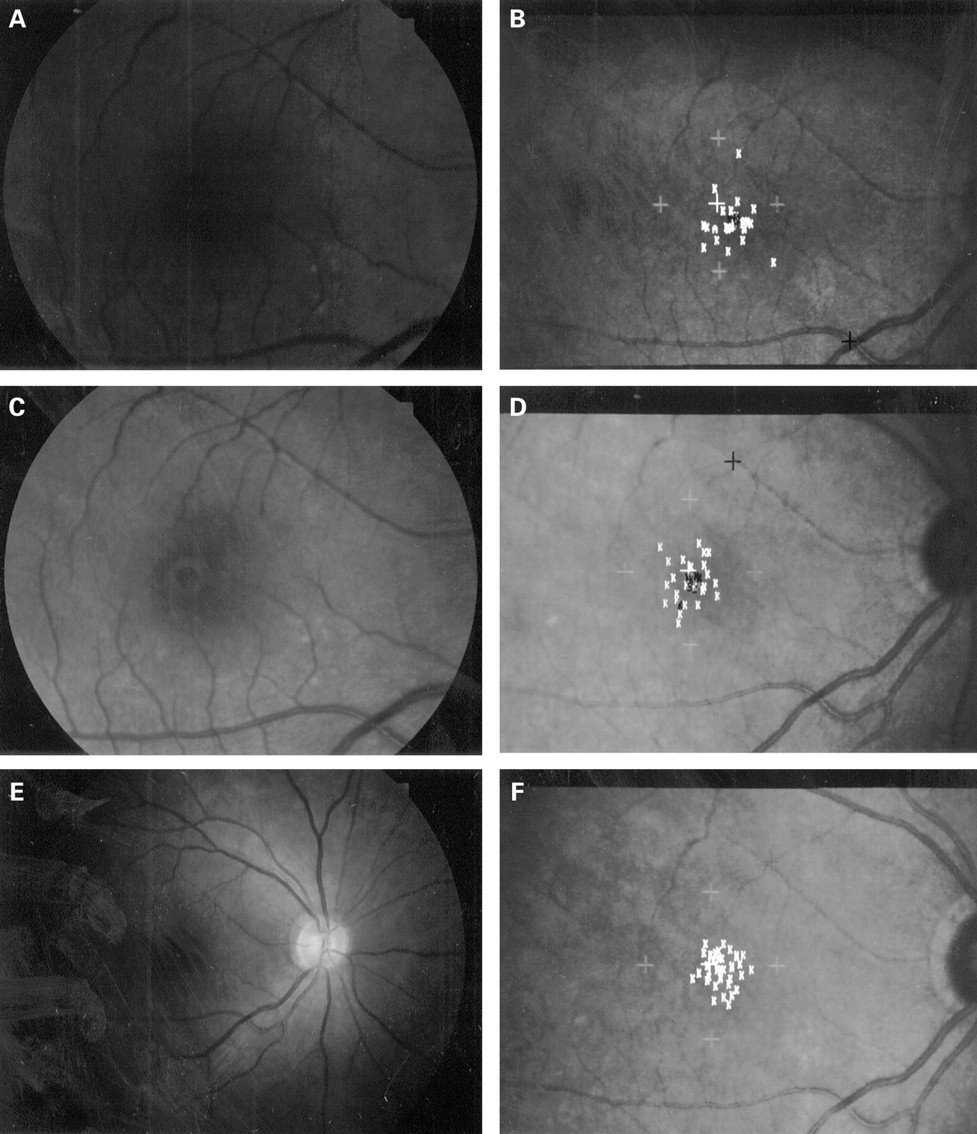
SLO microperimetry using a 0 dB stimulus allowed detection of scotomas in four of four (100%) eyes with atypical full thickness macular holes, and none of five (0%) eyes with atypical impending macular holes and macular pseudoholes. Only one eye (20%) with an impending macular hole showed a relative scotoma. In two of these atypical cases (cases 1 and 4), the size of the scotoma measured by SLO microperimetry enlarged during observation (Fig 3).

{kind=link}
{kind=link}
{kind=link}
Fundus photograph and scanning laser ophthalmoscope (SLO) microperimetry of case 1. A 50-year-old woman presented with a 5 day history of visual loss in her right eye. The initial diagnosis was an impending macular hole. (A) Fundus photograph at presentation. Her best corrected visual acuity was 20/30. (B) Scanning laser ophthalmoscope microperimetry with a 10 dB stimulus at presentation. The white ‘K’s indicate points seen by the patient, and black ‘K’s correspond to points not seen. There is a relative scotoma at the nasal border of the macular hole. (C) Fundus photograph taken 2 months later. Her best corrected visual acuity had dropped to 20/50. The hole had enlarged and the cuff of subretinal fluid surrounding the hole had increased in size. (D) SLO microperimetry performed at that time shows extension of the scotoma to the nasal side of the hole. (E) Fundus photograph of the patient taken 1 month after vitrectomy and gas injection. The hole was closed anatomically. (F) SLO microperimetry recorded 1 month postoperatively. The scotoma had disappeared.
Discussion
An impending (stage 1) macular hole is thought to be a transient condition that can lead to a full thickness macular hole.3 4 18 In approximately one half of cases, a spontaneous posterior vitreous detachment occurs and vitreous traction is released, resulting in visual improvement. In the remaining cases, however, tangential vitreous traction results in full thickness macular hole formation, usually leading to central visual loss.3Surgical intervention for impending macular holes in an attempt to prevent progression to full thickness macular holes has been reported.19 20 Although early reports had promising results, more recently the Vitrectomy for Prevention of Macular Hole Study Group found little or no benefit from surgical treatment of impending macular holes. Considering the cost and risk of vitrectomy, a conservative approach for stage 1 macular holes may be appropriate.21 Once a retinal break occurs (full thickness macular hole), vitrectomy is necessary to prevent permanent central visual loss. Therefore, differentiation of full thickness macular holes from impending macular holes has became very important.
Although macular pseudoholes are sometimes indistinguishable from full thickness macular holes by clinical examinations, including direct biomicroscopic observation, Amsler grid testing, and the slit-beam test, the two entities have quite different treatments. The features of macular pseudoholes have been studied in detail.10 13 14 22 Visual acuity is usually good but in some cases can be less than 20/60.22 In our study, the worst visual acuity seen in eyes with macular pseudoholes was 20/100, which is in the visual acuity range of full thickness macular holes. It is not satisfactory to confirm these diagnoses by visual acuity only.
The accuracy of diagnosing macular holes by conventional examinations partly depends on the ability and the experience of the examiner. Fish et al reported that the diagnosis by the initial examining physician was correct in only 43% of eyes with macular pseudoholes.13 In our study, the diagnostic accuracy of residents and referring ophthalmologists was relatively poor. In nine atypical cases, confirmation of the diagnosis was difficult even for members of the retina faculty. Amsler grid and slit-beam testing were not useful in diagnosing these nine atypical cases. These findings reflect the fact that there is no objective standard in diagnosing full thickness macular holes.
Previously, we reported the preliminary result of SLO microperimetry in diagnosing full thickness macular holes.23 Other investigators have also applied SLO microperimetry to the study of macular holes.24 25 In this study, we evaluated the ability of SLO microperimetry to differentiate full thickness macular holes from macular pseudoholes and impending macular holes. We found it possible to detect a scotoma in the macular region of all the eyes eventually diagnosed with full thickness macular holes. In contrast, all patients who were diagnosed with impending macular holes or macular pseudoholes could detect the 0 dB stimulus throughout the involved area, and only one of these patients had a scotoma on testing with the 10 dB stimulus. Thus, SLO microperimetry is very sensitive (100%) and specific (100% with the 0 dB stimulus and 98.0% with the 10 dB stimulus). Even in our atypical cases, SLO microperimetry demonstrated high accuracy in the diagnosis of macular holes. According to a recent study, 96% of stage 2 macular holes progress to stage 3 and stage 4 macular holes, and may need surgical intervention.26 An accurate diagnosis without delay is highly desirable.
This study was not specifically designed to determine the optimal SLO parameters for macular hole diagnosis. However, we did gain insight into this question. For example, in some cases of stage 2 full thickness macular holes we did not detect a scotoma with the use of the Goldmann III equivalent and Goldmann II equivalent stimulus (with a diameter of 110 and 55 mm, respectively), but did detect one using the Goldmann I equivalent stimulus. This suggests that large stimuli cannot detect small scotomas corresponding to small retinal breaks. We found the Goldmann I equivalent stimulus size to have the best sensitivity and specificity in the detection of macular scotomas. The choice of a fixation target is also an important consideration, because patients with macular holes often have poor fixation. For patients with poor visual acuity, we found a four point fixation target to lead to more steady fixation than a centrally located target. Four point fixation also has the advantage that it does not interfere with stimuli projected near the centre of the macula. The difference in the results between the 0 dB stimulus and the 10 dB stimulus was minimal.
Martinez et al reported the value of conventional examinations, including Amsler grid testing, the slit-beam test, and the laser aiming beam test in differentiating full thickness macular holes from macular pseudoholes.27 In our study, Amsler grid and slit-beam testing were not reliable in atypical cases. The laser aiming beam test may give results similar to that of SLO microperimetry. However, the smallest stimulus size available with the laser beam test is 50 mm, which is as almost twice as large as the smallest stimulus available with SLO microperimetry. According to Martinez et al, 100 mm and 200 mm laser beams were less reliable than 50 mm, indicating that the size of the stimulus is an important determinate of the ability to obtain accurate diagnostic information.27 We found that we were less able to detect a scotoma with the use of the Goldmann III equivalent or Goldmann II equivalent stimuli, which are approximately 100 and 50 mm, respectively. Therefore, SLO microperimetry with a Goldmann I equivalent stimulus appears to be more sensitive than the laser beam test. Moreover, using SLO microperimetry, we can precisely stimulate and detect responses from specific retinal loci, potentially allowing ophthalmologists to follow the development and progression of idiopathic macular holes. In our study, progression of a macular hole was observed in two cases using SLO microperimetry.
In our hands, SLO microperimetry is very useful in precisely distinguishing full thickness macular holes from similar appearing lesions. With this test, we can determine objectively the need for surgical intervention.
Acknowledgments
Supported by the grants in aid for Scientific Research (No 07557263) from the Ministry of Education, Science and Culture of Japan.
References
Linked Articles
- Editorial