Article Text

Abstract
AIMS/BACKGROUND Deep lamellar keratoplasty (DLK) was performed to restore visual acuity in 120 eyes with corneal stromal opacification. DLK is believed to be an effective treatment in eyes in which endothelial cell function had been preserved, and in which there was no epithelial or stromal oedema. The purpose of this study was to evaluate the effectiveness of this treatment.
METHODS The stroma was excised to the extent that only Descemet’s membrane remained, at least in the optical zone. Donor corneas of full, or almost full, thickness with Descemet’s membrane removed, or which had been lathed to a thickness of 0.4 mm from the endothelial side, were attached by suturing.
RESULTS In 113 eyes which were observed for 6 months or more postoperatively in which average prospective visual acuity was 0.09, average postoperative visual acuity improved to 0.6. Specular microscopy 1 month postoperatively revealed average endothelial cell counts of 2225 (SD 659)/mm2, while 24 months postoperatively this value was 1937 (642)/mm2 (cell loss 13%). Puncturing of Descemet’s membrane during surgery occurred in 47 of 120 eyes (39.2%), but after 12 months, there was no difference in visual acuity or number of endothelial cells between these eyes and those in which no puncturing had occurred.
CONCLUSIONS There was no postoperative endothelial rejection reaction with DLK, and restoration of postoperative visual acuity was quite adequate. Compared with penetrating keratoplasty, DLK allows endothelial cell counts to be maintained for a longer period. In addition, results can be expected to be more consistent over the long term with DLK.
- deep lamellar keratoplasty
- optical keratoplasty
- Descemet’s membrane
- hydrodelamination.
Statistics from Altmetric.com
Lamellar keratoplasty (LKP) is regarded mainly as a technique of therapeutic keratoplasty, as restoration of visual acuity postoperatively is often poor with this procedure. However, deep lamellar keratoplasty (DLK), in which pathological corneal stroma is completely excised as far as Descemet’s membrane, at least in the pupillary region, leads to a marked improvement in postoperative visual acuity, and compares favourably with penetrating keratoplasty (PKP). DLK is indicated for eyes in which there is stromal opacification with no epithelial or stromal oedema, and where it is thought that endothelial cell function is preserved.
Materials and methods
DLK was performed at the Sugita Eye Hospital in 120 eyes in 106 patients over the period May 1988 to April 1995. Preoperative diagnoses were corneal leucoma in 47 eyes in 40 patients, lattice corneal dystrophy in 22 eyes in 20 patients, gelatinous drop-like dystrophy in 22 eyes in 19 patients, granular corneal dystrophy in seven eyes in five patients, scarring after infections including corneal herpes in 18 eyes in 18 patients, and four eyes in four patients otherwise.
With the exception of one patient, there was no corneal epithelial or stromal oedema. In all patients preoperative ultrasound pachymetry revealed that the minimum corneal thickness was no more than 620 μm.
Ages of patients ranged from 8 to 86 years (average age 59 years). There were 50 male and 56 female patients. Donor corneas used were full thickness corneas including endothelial cells in 16 eyes, corneas in which Descemet’s membrane had been ablated with a cotton swab in 50 eyes, and corneas lathed to a thickness of about 0.4 mm from the endothelial side by using Barraque’s cryolathe in 54 eyes.
SURGICAL METHODS
Lamellar keratectomy
Firstly, the cornea is trephined through three quarters of its depth and a lamellar keratectomy performed. A trephine with a stopper may be used, but it may be difficult to cut to the desired depth. The Barron vacuum trephine cuts well and is very convenient. However because the edge of the blade is screwed down, depth may vary depending on position.
A Golf or Paufique knife is used for the lamellar keratectomy, care being taken to maintain a consistent depth as far as possible. When the fragments of stroma are lifted away, there will be an area of whiteness at the edge of the incision, which is the result of air penetrating between the collagen fibres. The cut is made with the blade moving as if stroking this area.
Deep lamellar keratectomy
(a) Hydrodelamination Stromal collagen fibres are cut across and down to produce a depression, and a saline solution injected with a blunt, 27 gauge needle at the bottom of this depression. The solution penetrates between the collagen fibres, which whiten and swell. Stroma that was not apparent will swell up and can be safely removed by further spatula delamination.
By performing hydrodelamination in this way it is also possible to tell whether or not the remaining stroma is close to normal. Thus, as illustrated in Figure 1, the solution injected spreads evenly in all directions, indicating that the normal structure of the collagen fibres is maintained. With pathological stroma, the solution does not spread evenly and there is little swelling. Because the deeper stromal fibres are coarser, the solution from a single injection will spread more widely. Where the stroma is close to normal, hydrodelamination proceeds until no more swelling can be seen, and removal of the stroma then stops. With pathological stroma, however, excision must proceed until Descemet’s membrane is exposed.
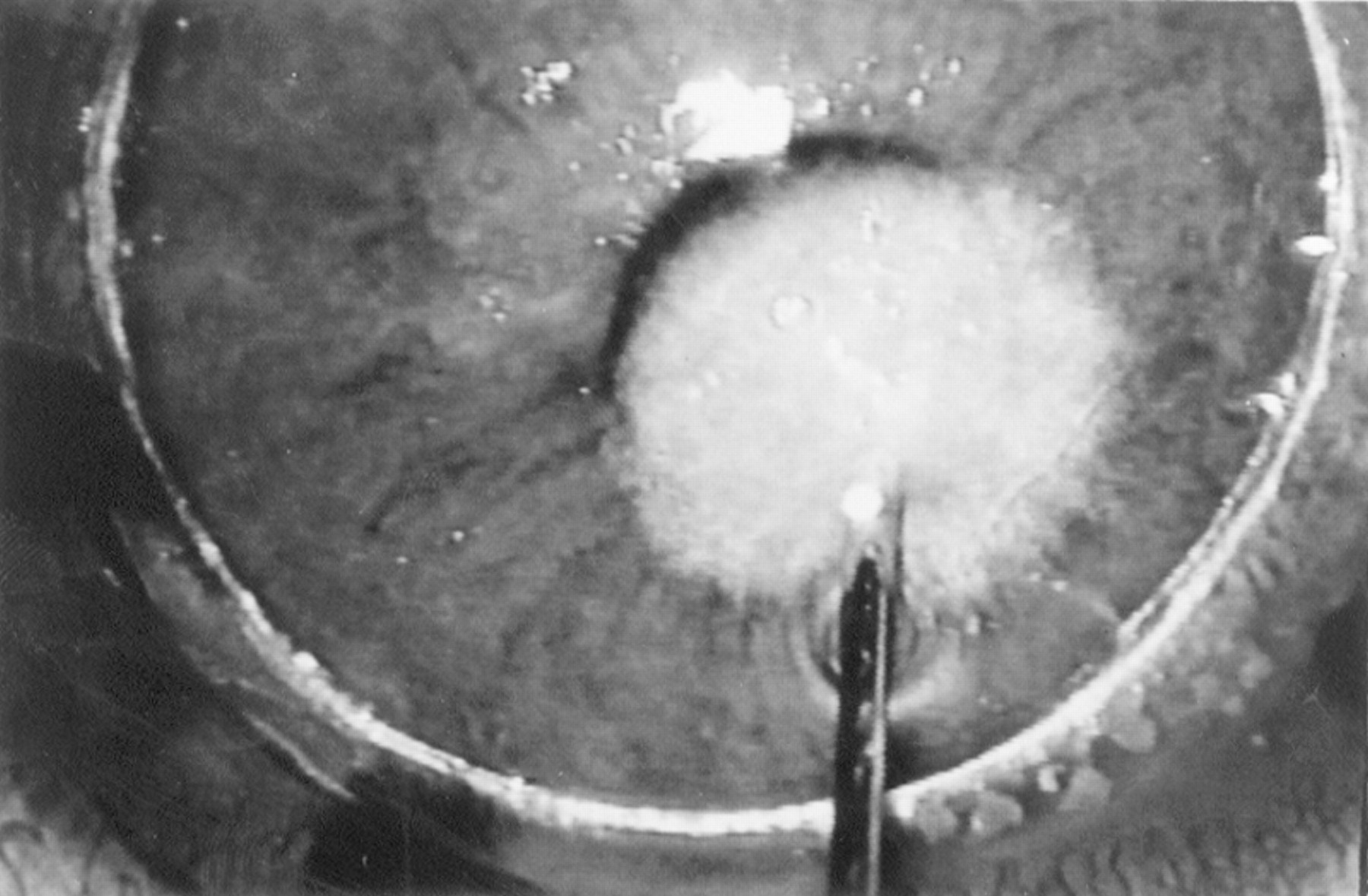
Hydrodelamination. A solution injected into the normal stroma spreads evenly in all directions and the remaining stroma whiten and swell.
(b) Spatula delamination A small cut is made in the remaining stroma with the Golf knife as if checking the depth, and from the bottom of the cut a fine spatula with a diameter of 0.25 mm (Katena K3–2310) is inserted rectilinearly into the stroma.
Once the spatula has advanced some way, it comes back and is moved again and again fan-like in different directions (Fig 2). The Paufique knife or corneal scissors is slipped into this opening and the stroma removed. It is important to excise the stroma little by little to avoid going too deep at any point.

Spatula delamination. A fine spatula inserts rectilinearly into the hydrodelaminated stroma and comes back and is moved again and again fan-like in different directions.
(c) Exposure of Descemet’s membrane In thinner sections, anterior chamber pressure will cause a little bulging of the remaining stroma when the Descemet’s membrane is close. Descemet’s membrane is quite different from the stroma with its fibrous structure. It is a smooth and glossy membrane, and the difference is apparent immediately (see Fig 3).

Descemet’s membrane is smooth and even, clearly distinguishable from the stroma.
Descemet’s membrane adheres only loosely to the stroma, so that a spatula can be moved horizontally. If the remaining stroma is lifted with suturing forceps, it can be removed with corneal scissors over an area with a diameter of about 5 mm, covering the area of the pupil. Puncture can easily occur at this stage of the procedure, and delicate work is required. In addition, Descemet’s membrane thickens with age, and can be fairly tough in the elderly. In the young, conversely, it is thin, and although elastic, is easily ruptured.
(d) Puncturing Descemet’s membrane If Descemet’s membrane is punctured during this procedure, and the hole is very small, the Descemet’s membrane can be exposed by injecting air into the anterior chamber.
If there is extensive linear tearing, and stroma has been excised to an adequate depth, then removal of the stroma can be abandoned at this point and a start made on suturing the graft.
Preparing the graft
For 54 eyes, corneas were prepared by cryolathing from the endothelial side to a thickness of about 0.4 mm, and preserved by freezing before use. In 50 eyes, virtual full thickness grafts punched from the endothelial side after removal of Descemet’s membrane with a cotton swab were used. For 16 eyes, fresh corneas with endothelial cells still attached were used.
Postoperative transparency is achieved more quickly where fresh corneas are used, but over time the results are similar with corneas that have been frozen and preserved. A cornea preserved in glycerine was used in a single eye, and this graft had become very hard, making suturing difficult and causing problems with transparency postoperatively.
Results
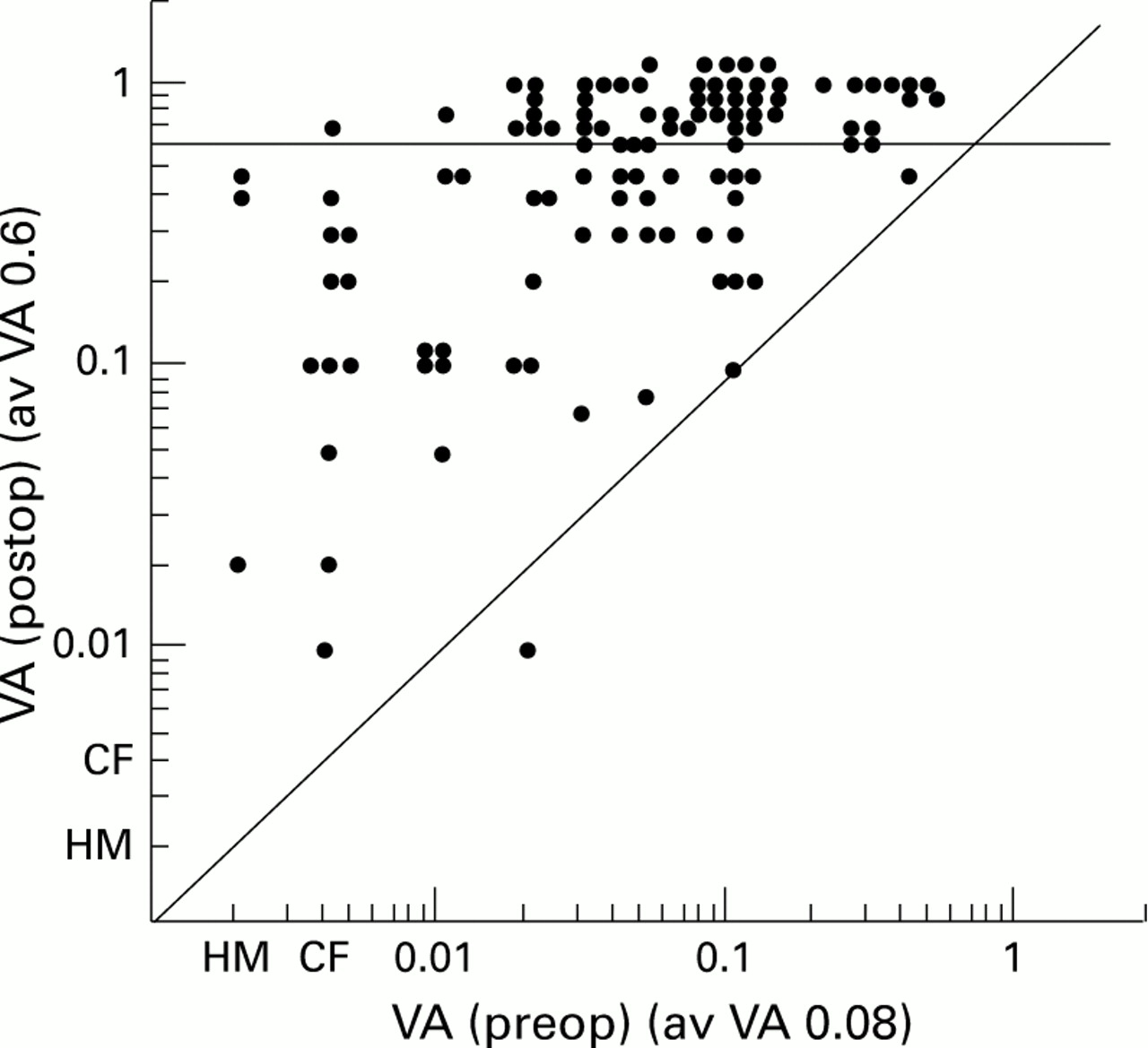
In 113 eyes observed for 6 months or more and in which average preoperative visual acuity was 0.09, average postoperative visual acuity improved to 0.6 (Fig 4). In 71 of 113 eyes (62.8%), corrected postoperative visual acuity was 0.5 or better. There were 12 eyes in which corrected visual acuity was 0.1 or worse, but in nine of these, abnormalities were seen in the macular region.

Change of preoperative and postoperative visual acuity (87 eyes were followed up for more than 6 months).
Comparisons of postoperative visual acuity in five original pathologies are shown in Table 1. Gelatinous drop-like dystrophy showed statistically significant worse visual acuity than the others (granular dystrophy and lattice dystrophy; p<0.01, corneal leucoma and scarring; p<0.05, Tukey test).
Comparison of average visual acuity in five original pathologies
Specular microscopy 1 month postoperatively revealed an average endothelial cell count of 2225 (SD 711)/mm2, while 24 months postoperatively this value was 1937 (633)/mm2 (cell loss 13%).
There were 80 eyes in which Descemet’s membrane alone constituted the optical zone. In 40 eyes, some parts of the deeper stromal lamellae were closer to normal, and hydrodelamination was abandoned at the point at which the stroma failed to swell, leaving some stroma remaining.
Table 2 compares corrected visual acuity and cell counts in these two groups at 12 months postoperatively. Both visual acuity and cell counts tended to be better where stroma remained, perhaps because the remaining stroma was close to normal and also became extremely thin, but statistically no difference was seen.
Comparison of visual acuity and cell count, at 12 months after surgery, between 80 eyes with Descemet’s membrane exposed and 40 eyes with some stroma left during operation
Table 3 compares eyes in which the donor cornea was cryolathed to a thickness of 0.4 mm from the endothelial side with eyes in which a full thickness cornea with Descemet’s membrane only removed with a cotton swab or which included the endothelium were used.
Comparison of corneal thickness, visual acuity, and cell counts at 12 months postoperatively by difference between full thickness grafts and cryolathed grafts
Preoperatively, there was no difference in corneal thickness as measured with the pachymeter between the two groups. However, 12 months postoperatively, there had been a significant decrease in corneal thickness in the cryolathed group, at 453 (90) μm, as against 592 (57) μm in the full thickness group (p = 0.000, t test).
No differences in postoperative visual acuity or in cell count were seen between the two groups at 12 months postoperatively.
Descemet’s membrane was punctured during surgery in 47 of 120 eyes (39.2%). This occurred in 37 of the first 80 eyes (45%), but fell to 10 in 40 eyes (25%) in later procedures. This was due to the fact that use of hydrodelamination became more widespread, but was not used unnecessarily where the deeper corneal stroma was close to normal, in which case some stroma was left.
Where Descemet’s membrane had been punctured, anterior chamber aqueous may collect postoperatively at the interface between the graft and the recipient cornea to form a double anterior chamber. Oedema and opacification occur as a matter of course if grafts from which endothelial cells have been removed are used. A double anterior chamber was seen in 14 of 47 eyes (30%), but an injection of air into the anterior chamber eliminated the accumulated aqueous at the interface in all eyes, and all recovered.
Among 120 eyes, Descemet’s membrane was punctured in 47 and remained intact in 73. No statistically significant difference was seen when these two groups were compared for visual acuity and cell counts 12 months postoperatively (Table 4). No statistically significant difference was seen between the 14 of 47 puncture eyes in which a double anterior chamber was seen postoperatively and the other 33 puncture eyes (Table 5).
Comparison of visual acuity and cell counts at 12 months postoperatively by presence of intraoperative puncture of Descemet’s membrane
Comparison of average visual acuity and cell counts at 12 months postoperatively by presence of double anterior chamber as the complication in 47 punctured eyes of Descemet’s membrane
Discussion
Lamellar keratoplasty has a number of advantages as a keratoplasty. No procedures are performed within the anterior chamber during surgery, so there is no postoperative intraocular complication such as anterior synechia of iris or secondary glaucoma. There is no endothelial rejection reaction and there is no need for the graft to have endothelial cells attached, so preserved corneas can be used. However, there is a decisive deficiency, which is that postoperative visual acuity is poor. LKP has, therefore, been regarded mainly as a therapeutic keratoplasty.
The cause of poor postoperative visual acuity is thought to be scarring which occurs at the interface between the donor cornea and the stroma of the recipient cornea, but this has not been established clearly in the literature.
Experiments with DLK suggested that it was possible to obtain a marked improvement in postoperative visual acuity while retaining the advantages of LKP.1 In these eyes, pathological corneal stroma was completely excised so that Descemet’s membrane was exposed at least in the region of the pupil, and donor corneas from which Descemet’s membrane has been removed were used.
Descemet’s membrane is a basement membrane of uniform structure, whose thickness is thought to increase with age. Histologically it is quite thin, at about 10–13 μm in adults,2 3 and perhaps because it is thought to be very weak, there have been no reports on techniques that expose Descemet’s membrane intentionally during surgery.
However, if the effort is made to expose Descemet’s membrane during surgery, and this exposed section is then extended, so that there is an area about 5 mm across including the area of the pupil where Descemet’s membrane only is present, it will be found that there is practically no adhesion at this point between Descemet’s membrane and the section where stroma remains.
If the endothelial side of the donor cornea is wiped with a cotton swab, Descemet’s membrane can be ablated easily, leaving a completely smooth surface on the stromal side. The result is that no scar is formed at all at the interface between the host cornea, where Descemet’s membrane only is present, and the donor cornea, from which Descemet’s membrane has been removed. This is probably the reason that there is significant improvement in visual acuity postoperatively.
As for donor corneas, no difference was seen in average visual acuity 12 months postoperatively between a group in which virtually full thickness corneas with Descemet’s membrane only removed or to which endothelial cells adhered, and a group in which corneas were cryolathed to a thickness of 0.4 mm. However, it was seen in the cryolathe group that, as might be expected, corneas were significantly thinner.
A point worthy of note is that there was no endothelial rejection among 120 eyes. The condition considered to have the best prognosis after PKP is keratoconus. Of 72 eyes treated over the past 7 years (1988–95) at the Sugita Eye Hospital, all except one were maintained optically clear. However, in 55 eyes that were followed up more than 2 years after PKP, endothelial rejection has been seen in seven eyes (12.7%). Postoperative endothelial cell counts, examined in 48 eyes treated with PKP for keratoconus, continued to fall in a straight line over 2 years. By contrast, mean cell counts in 74 eyes treated with DLK tended to fall for the first 6 months postoperatively, but then stop (Fig 5). Cell loss with DLK between the first month and 2 years postoperatively was 13%. After DLK the patient’s own cells are active; when there is no danger of an endothelial rejection reaction, the cornea is very stable after keratoplasty.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trend of decrease in postoperative endothelial cell counts, in 74 eyes that underwent deep lamellar keratoplasty(DLK) and 48 eyes that underwent penetrating keratoplasty (PKP) with keratoconus.
For corneal opacification for which surgery is indicated, examination of endothelial cell counts generally is unavailable preoperatively. Specular microscopy 6 months after DLK revealed that over 58% of the eyes had endothelial cell counts of more than 2000/mm2. Fairly rich endothelial cells could be preserved with DLK; in contrast, in PKP, endothelial cells could be totally replaced with the donor’s cells.
Gelatinous drop-like dystrophy showed significantly worse postoperative visual acuity within five original pathologies. Gelatinous drop-like dystrophy is chiefly affected corneal epithelium and Bowman’s layer and recurred in transplanted grafts. This recurrence could be protected against by using a combined procedure with keratoepithelioplasty4 or conjunctival autograft and also using a therapeutic soft contact lens thereafter.
To date, there have been few reports on DLK1 5 8especially on complete stromal excision exposing Descemet’s membrane, because surgical techniques for DLK are considered to be difficult.
The new technique uses hydrodelamination in which a saline solution is injected into the deep stroma to swell stromal collagen fibres, and spatula delamination in which a thin 0.25 mm diameter spatula is employed. Thus, complete excision of pathological stroma is possible to limit the optical zone to Descemet’s membrane only, minimising the risk of puncture of Descemet’s membrane.
A previous report described stromal excision by utilising air injected into the stroma.7 8 This method is only possible when the stroma maintains its consistency. If the stromal layer is thin, this method is not applicable. Transparency of the stroma is lost by injecting air, thus preventing visibility of collagen fibres.
With hydrodelamination, a saline solution is injected to swell the thin stroma to make it thick enough to allow further excision. The stroma is temporarily opacified by the injected solution, but it does not prevent identification of collagen fibres. Further, by observing how the solution penetrates into the stroma, one can determine the density of the stromal collagen fibres and whether the stroma is nearly normal or not. If the stroma is nearly normal, the solution spreads in all directions, and the stroma whitens and swells (Fig 1). In pathological stroma, where the structure of collagen fibres is lost and scarred, the solution cannot penetrate into the stroma and there is very little whitening and swelling. Such pathological stroma should be excised completely to leave only Descemet’s membrane. If the deep stroma is close to normal, excision should be stopped at the point where the stroma does not swell any more with hydrodelamination, leaving a small portion of the stroma unexcised.
Of 120 eyes, 80 had Descemet’s membrane exposed and 40 had some portion of the stroma left intraoperatively. Average visual acuity and endothelial cell counts were compared between these two groups 12 months postoperatively. Leaving a small amount of stroma did not produce any difference in visual acuity as long as the deeper stroma is fairly normal. Any puncture occurring during surgery puts surgeons under considerable stress; so, leaving a small amount of stroma is recommended. In this case, however, it is essential that hydrodelamination spreads the solution evenly in the stroma and that the stroma is excised deeply enough to the extent that it does not swell any more with the injected solution.
Fresh donor corneas offer earlier recovery of postoperative visual acuity. However, 3 months postoperatively and thereafter, visual acuity obtained with stored frozen corneas is comparable with that obtained with fresh corneas.
Puncture in Descemet’s membrane is an intraoperative complication. This might occur when surgeons try to limit the optical zone to only Descemet’s membrane, because any portion of pathological stroma, if unexcised, may result in poor visual outcome, which is almost inevitable with the current surgical procedure. There are two methods of dealing with this. If the hole is small, air is injected into the anterior chamber and a graft is sutured on. If the hole is large, further excision of the stroma is abandoned and a graft is sutured, then air is injected into the anterior chamber. Care should be taken if a viscoelastic material is used, because there is risk of entrapment of the viscoelastic material between Descemet’s membrane and the graft, and its absorption might be considerably delayed. As an alternative, when a puncture does occur one can switch to PKP, but all the 47 eyes in this report were treated with DLK.
Formation of a double anterior chamber was observed as a postoperative complication in 14 eyes (30%) out of 47 eyes in which Descemet’s membrane was punctured during operation. The graft, without endothelial cells, will develop oedema like primary graft failure. If the double anterior chamber does not disappear after a few days, it is necessary to inject additional air into the anterior chamber and to drain the collected aqueous humour from the space of the double anterior chamber. Because of multiple interventions, in these eyes there was a tendency towards a decrease in endothelial cell counts but statistically no difference was found between the ‘presence of double anterior chamber’ group and ‘non-presence group’ at 12 months postoperatively. Also, there was no difference in visual acuity between two groups. If the donor corneas are fresh and with endothelial cells, the grafts can survive as usual PKP even though a double anterior chamber is formed.
The success rate of PKP is rising year by year. However, endothelial cells continue to reduce at a considerable speed even 5 years after surgery9), and a long term reduction over 10 or 15 years often results in a relapse of opacification due to decompensation of endothelial cells.
Deep lamellar keratoplasty should be used more frequently because it offers satisfactory visual outcome and stability for a longer period of time, but if it is only possible to remove pathological stroma totally.
Acknowledgments
This study was supported in part from a grant by Aichi Eye Bank.