Article Text

Abstract
AIM To demonstrate the usefulness of a recently developed technique of imaging fundus autofluorescence and to compare it with the results of fluorescein angiography in the diagnosis and staging of macular holes.
METHODS The intensity and distribution of fundus autofluorescence was studied in 51 patients with idiopathic macular holes and pseudoholes using a confocal laser scanning ophthalmoscope (cLSO) and the images were compared with those obtained by fundus fluorescein angiography.
RESULTS Autofluorescence imaging demonstrated bright fluorescence of macular holes with appearance similar to that obtained by fluorescein angiography. In contrast macular pseuodoholes showed no such autofluorescence. The attached operculum in stage 2 macular holes and the preretinal operculum in stage 3 macular holes showed focal decreased autofluorescence. The associated retinal elevation and the cuff of subretinal fluid were less fluorescent compared with the background autofluorescence of the normal fellow eyes. Following successful surgical treatment the autofluorescence of the macular holes was no longer visible.
CONCLUSION Autofluorescence imaging with the cLSO makes the assessment of macular holes possible with an accuracy comparable with that of fluorescein angiography. Being non-invasive and rapid, autofluorescence imaging may become a useful alternative to fluorescein angiography in the assessment and the differential diagnosis of full thickness macular holes.
- fundus autofluorescence
- macular hole
- lipofuscin
- retinal pigment epithelium
- laser scanning ophthalmoscope
Statistics from Altmetric.com
- fundus autofluorescence
- macular hole
- lipofuscin
- retinal pigment epithelium
- laser scanning ophthalmoscope
The diagnosis of idiopathic full thickness macular holes (FTMH) is usually made by history and by biomicroscopic examination. However, at times it may be difficult to differentiate between a FTMH and a macular pseudohole even using otherwise reliable clinical tests such as the Watzke–Allen slit beam test.1 In such cases fluorescein angiography is used but this has the disadvantage of being invasive, requiring an intravenous injection of sodium fluorescein which carries a potential risk of adverse reactions.2
Recently a new technique has been developed that allows in vivo imaging of the distribution of fundus autofluorescence using a confocal laser scanning ophthalmoscope (cLSO).3 This provides high spatial resolution imaging of the distribution of fundus autofluorescence which is most likely derived from lipofuscin within the retinal pigment epithelium.3-5 It is generally accepted that lipofuscin represents the product of degradation of photoreceptor outer segments. In a normal fundus, the distribution of fundus autofluorescence is diffuse, with decreased intensity at the fovea, at the optic nerve head, and under the retinal blood vessels which appear dark.3 4 As this technique images the intrinsic fluorescence of the fundus derived from the retinal pigment epithelium,3-5 it should be possible to demonstrate a macular defect such as the FTMH similar to that seen on fluorescein angiography.
In this study we obtained images of the intrinsic autofluorescence of the fundus with a cLSO in patients with macular holes and pseudoholes and compared the images with those obtained by fluorescein angiography.
Material and methods
The technique of imaging fundus autofluorescence has been described previously.3 4 Briefly the cLSO used in this study was a prototype (SM 30-4024) donated by Zeiss (Zeiss, Oberkochen, Germany). The argon laser (wavelength 488 nm and power of 250 μW) was used for illumination, and to record autofluorescence a filter with a cut off at 521 nm was inserted in front of the detector. The cLSO images were recorded at standard video scanning rates on SVHS video tape and digitised at 256 × 256 resolution using a Wide Vision V-10 frame grabber (Wild Vision, Tyne and Wear) with an Acorn Archimedes computer (Acorn Computers, Cambridge).
A prospective study was undertaken of patients with unilateral idiopathic FTMH and with macular pseudoholes. We deliberately selected only patients with unilateral macular holes in order to compare the autofluorescence images and the fluorescein angiograms with the corresponding areas in the normal contralateral eye.
The FTMH was diagnosed on clinical examination by biomicroscopy as a full thickness neurosensory defect, by the presence of Watzke–Allen sign1 and by the demonstration of a macular transmission defect on fluorescein angiography. The holes were staged according to the classification proposed by Gass6 and Johnson and Gass.7 Briefly, stage 1 (impending) macular hole refers to a foveolar or foveal detachment without a full thickness retinal defect. Stage 2 refers to a small full thickness macular defect but no posterior vitreous separation. In stage 3 there is a partial posterior vitreous separation with a vitreous condensation (operculum) visible in front of a FTMH. In stage 4 there is complete vitreous separation and an operculum is difficult to visualise.
Before examination with the cLSO, the pupil was dilated with cyclopentolate 10% and phenylephrine 2.5% to a diameter of at least 7 mm. The 20° and 40° field of view mode and the confocal aperture 3 providing a depth resolution of less than 300 μm were used to produce reflectance images of the fundus and of the distribution of fundus autofluorescence.
Analysis of the regional variations of autofluorescence intensity in the normal control eyes showed that the difference in autofluorescence intensity measured in two adjacent boxes of 8 × 8 pixels was no greater than 5 units and that the difference in autofluorescence intensity between the two eyes in the same patient measured in similar areas is no greater than 5 units. We regarded therefore as a focal decreased autofluorescence or increased autofluorescence any variation greater than 10 units measured in boxes of 8 × 8 pixels compared with the corresponding area in the contralateral eye. The focal variation was graded as mild when the difference between the two areas was 10–15 units, medium when the difference between the two areas was 15–20 units, and intense over 20 units.
The autofluorescence and reflectance images of eyes with macular holes and pseudoholes were compared with corresponding fundus colour photographs, fluorescein angiograms obtained using a standard fundus camera, and with autofluorescence images of the normal contralateral eye. The autofluorescence intensity at the site of the macular hole was compared with the autofluorescence intensity of the corresponding area in the normal contralateral eye using the statistical package Excel Windows 5.0. The mean values and the standard deviations (mean (SD)) of the difference between the autofluorescence intensity at the site of the macular hole and the autofluorescence intensity of the corresponding area in the normal contralateral eye were calculated for each group of macular holes.
Results
We prospectively studied 46 eyes of 46 patients with unilateral idiopathic macular holes and five eyes of five patients with macular pseudoholes. There were 27 women and 19 men. Their ages ranged from 49 to 68 years (mean 54 years). The group of patients with macular holes consisted of six patients with stage 1 (impending) macular hole, eight with stage 2, 21 with stage 3, and 11 with stage 4 macular holes. In all patients with stages 2, 3, and 4 the diagnosis of FTMH was confirmed by the positive Watzke–Allen slit beam test.1Nine patients with macular holes stage 3 and 4 underwent macular hole surgery. In seven cases, a successful closure of macular hole was achieved.
STAGE 1 (IMPENDING) MACULAR HOLE
Three of the six patients with stage 1 macular holes showed no abnormal autofluorescence and the corresponding fluorescein angiograms were also considered to be normal. In the remaining three patients the foveal autofluorescence appeared slightly increased compared with the normal contralateral eye to the point of being equal to the autofluorescence of the surrounding parafoveal area (mean 7.33 (SD 6.25), p = 0.017). The corresponding fluorescein angiograms showed mild central hyperfluorescence in the mid phase of the angiogram (Fig 1).
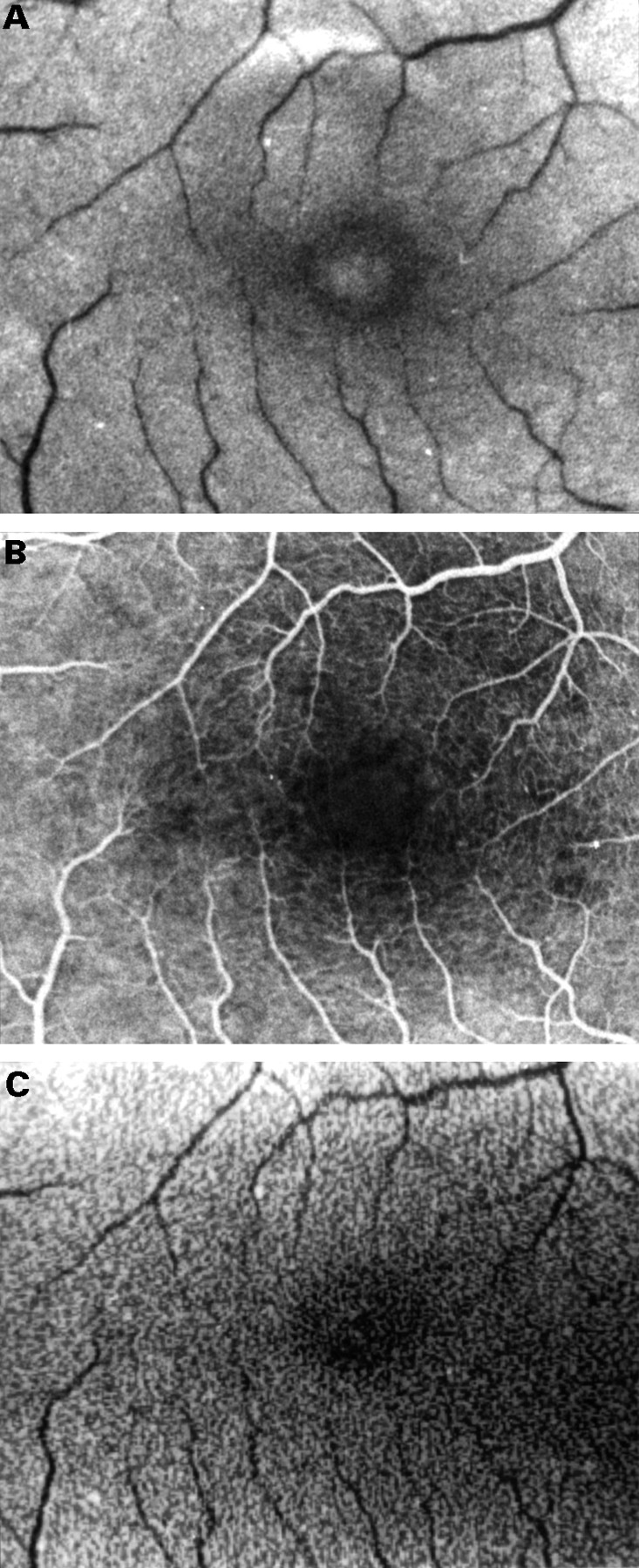
Fundus photograph of the right eye with a stage 1 full thickness macular hole (A). Note very mild hyperfluorescence in the mid phase of the fluorescein angiogram (B). Autofluorescence imaging shows an area of slightly increased fluorescence within the macular hole to the point of being equal to the autofluorescence of the surrounding parafoveal area (20° field) (C).
STAGE 2 MACULAR HOLE
All of the eight stage 2 macular holes showed intense autofluorescence at the site of the hole (mean 51.12 (SD 5.64), p < 0.001). The fluorescein angiograms of these eyes showed a transmission defect which corresponded exactly in location, size, and shape with that seen on autofluorescence imaging. In one patient the autofluorescence of FTMH was partly obscured (Fig 2). It is possible that the area of decreased autofluorescence represents the attached operculum.

Fundus photograph of the right eye with a stage 2 full thickness macular hole (A). Fluorescein angiography shows a small window defect (B). Autofluorescence imaging shows increased fluorescence centrally. The less fluorescent zone within the macular hole in the superior-nasal part may represent a partially attached operculum (20° field) (C).
STAGES 3 AND 4 MACULAR HOLES
Autofluorescence imaging of the stages 3 and 4 FTMH produced intense hyperfluorescence (mean 53.9 (SD 5.28), p < 0.001 for the stage 3 macular hole group and mean 50.64 (4.18), p < 0.001 for the stage 4 macular hole group) which was larger in size than those seen in stage 2 macular holes. This corresponded with the FTMH seen clinically and with the transmission defect seen on fluorescein angiograms (Figs 3 and 4).

Fundus photograph and fluorescein angiogram of the right eye with a stage 4 full thickness macular hole (A, B). Autofluorescence imaging shows increased autofluorescence centrally corresponding to the macular hole and a ring of decreased autofluorescence corresponding to the cuff of subretinal fluid. The shallow subretinal fluid which extends beyond the cuff is seen as an area of decreased autofluorescence surrounding the cuff of the hole (40° field) (C). The contralateral normal eye shows even autofluorescence (D).

Fundus photograph and fluorescein angiogram of the right eye of a patient with a stage 3 full thickness macular hole who subsequently underwent macular hole surgery (A, B). Preoperatively autofluorescence imaging shows increased autofluorescence centrally corresponding to the macular hole and a ring of decreased autofluorescence corresponding to the cuff of subretinal fluid and to the retinal elevation which extends beyond the cuff. The operculum appears as a dark structure on autofluorescence imaging (20° field) (C). The postoperative fundus photograph and fluorescein angiogram demonstrates the closure of the macular hole though there is a small pigment epithelial defect centrally (D, E). On autofluorescence imaging the central hyperfluorescence is no longer visible, demonstrating the closure of the macular hole. The hypofluorescence corresponding to the cuff disappeared too, suggesting flattening of the neurosensory detachment (20° field) (F).
The cuff of neurosensory retinal detachment surrounding the macular hole was visible clinically and on colour photographs in all but two eyes. The autofluorescence of the elevated retina was decreased in all these eyes (Figs 3 and 4). In contrast, on fluorescein angiography the cuff of subretinal fluid appeared hyperfluorescent in 21 out of the 32 eyes (66%) and hypofluorescent in 11 out of the 32 eyes (34%). The two eyes with no visible cuff showed no changes on autofluorescence compared with the same area in the normal contralateral eye.
The colour photographs and fluorescein angiograms were examined to determine if any retinal elevation could be detected beyond the cuff of the subretinal fluid surrounding the macular hole. Shallow retinal elevation extending beyond the cuff was seen in 18 of 32 eyes (56%). On autofluorescence imaging, this appeared hypofluorescent though less so than the cuff of subretinal fluid (Fig 3).
The presence of a preretinal operculum was demonstrated by a mobile disc-like hypofluorescence within the area of intense autofluorescence of the macular hole. We interpreted this as a shadow cast by the operculum on the retinal pigment epithelium. Focusing the cLSO in the reflectance mode on the operculum in front of the FTMH, we found that the operculum had the same shape and size and had the same movement as the hypofluorescent disc seen in front of the retina. In all the patients with stage 3 macular hole fluorescein angiography showed a window defect corresponding to the macular hole. The presence of the operculum could not be documented by fluorescein angiography (Fig 4).
CHANGES AFTER MACULAR HOLE SURGERY
In the seven eyes successfully closed after macular hole surgery the intense autofluorescence seen before surgery was absent postoperatively. The transmission defects seen preoperatively on fluorescein angiograms were no longer visible. Also the cuff of subretinal fluid was no longer visible on autofluorescence imaging and on fluorescein angiography (Fig 4).
In the two eyes with unsuccessful closure of macular hole the postoperative appearance was unchanged both on autofluorescence and on fluorescein angiography.
MACULAR PSEUDOHOLES
The fundus autofluorescence in the five eyes with macular pseudoholes was identical to that of the normal contralateral eye. The corresponding fluorescein angiograms showed no abnormal fluorescence (Fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fundus photograph of the left eye of a patient with a macular pseudohole (A). Fluorescein angiography shows no window defect (B) and autofluorescence imaging shows normal fluorescence confirming that there is no full thickness retinal defect (C).
Discussion
The management of macular holes has changed dramatically in the recent years. While surgical techniques are evolving rapidly8-13 the method of documentation of preoperative and postoperative macular appearances continues to rely mainly on fundus colour photography and fluorescein angiography. However, both these methods have certain disadvantages.14 The resolution of fundus colour photographs may be insufficient to allow for consistently reliable recognition of macular details or to demonstrate the presence of a preretinal operculum. The disadvantage of fluorescein angiography is that it is an invasive procedure which carries small but significant morbidity. In addition, it is time and labour intensive requiring the presence of a photographer, a nurse, and a doctor. The images may not be instantly available unless a digitised system is used. Other methods of imaging of macular holes have therefore been investigated, such as high resolution ultrasonography,15optical coherence tomography,16 reflectance imaging using a SLO,17 and most recently autofluorescence imaging with the help of the confocal laser scanning ophthalmoscope (cLSO).3
The fundus autofluorescence imaged using the cLSO described here derives from the lipofuscin laden retinal pigment epithelium.3-5 The latter is attenuated by the luteal pigment in the macula.5
In our study, all the patients with FTMH demonstrated hyperfluorescence at the macula on fluorescein angiography and on autofluorescence imaging. This is perhaps not surprising in that when the macular pigment which absorbs the short wavelength light of the laser in the cLSO is absent the fundus autofluorescence at that site appears more prominent.
Similarly, it could be predicted that an operculum lying in front of the macular hole would give rise to a shadow effect on the fundus on autofluorescence imaging; the luteal pigment and the neurosensory retinal tissue would attenuate the excitation light.5Confirmation of this hypothesis is also given by the alternating use of the reflectance and autofluorescence modes of the cLSO, focusing first on the operculum and then on the retina.
The cuff of subretinal fluid which surrounded the macular holes and any retinal elevation which extends beyond the cuff appeared hypofluorescent on autofluorescence imaging. This is possibly due to the presence of subretinal fluid and/or thickening of the neurosensory retina which attenuate the light that reaches the retinal pigmented epithelium. It is not clear why on fluorescein angiography some cuffs of subretinal fluid appear hyperfluorescent and some hypofluorescent though these differences are thought to be of prognostic value by some authors.18
The disappearance of autofluorescence of the macular hole after successful surgical closure suggests that the retinal pigment epithelium is again covered by retinal and/or glial tissue, as previously demonstrated histologically.19 The persistence of increased autofluorescence after unsuccessful macular hole surgery suggests that there is no bridging tissue over the defect in the neurosensory retina.
While in most cases the nature and the stage of a full thickness macular hole are obvious on clinical examination, difficulty in the diagnosis may be experienced even by experienced ophthalmologists.20 In our cases of macular pseudoholes referred for consideration of macular hole surgery, autofluorescence imaging excluded the diagnosis of a FTMH by the absence of central autofluorescence.
It is generally accepted that fluorescein angiography is an important tool in the evaluation of eyes with macular holes14 and it is particularly useful when the diagnosis of FTMH is in question.21 In this series we found that autofluorescence imaging allowed both the diagnosis and the staging of FTMH with accuracy comparable with that of fluorescein angiography. In addition, autofluorescence imaging has the advantage of being non-invasive and quite rapid, taking less than 5 minutes to perform and as such it may become an useful alternative to fluorescein angiography in the investigation of macular holes.
Acknowledgments
Dr von Rückmann was in receipt of a grant No Ru 575/1–1 from the Deutsche Forschungsgemeinschaft, Bonn, Germany and is now with the Department of Ophthalmology, Justus Liebig University, Friedrichstrasse 18, 35385 Giessen, Germany.