Article Text

Abstract
AIM The use of eye care services by people with and without diabetes was investigated in the Melbourne Visual Impairment Project (VIP), a population based study of eye disease in a representative sample of Melbourne residents 40 years of age and older.
METHODS A comprehensive interview was employed to elicit information on history of diabetes, medication use, most recent visit to an ophthalmologist and optometrist, and basic demographic details. Presence and extent of diabetic retinopathy was determined by dilated fundus examination.
RESULTS The Melbourne VIP comprised 3271 people who ranged in age from 40 to 98 years; 46.2% of them were male. Of 3189 people who had the fundus examination and knew their diabetes status, 162 (5.1%) reported having been previously diagnosed with diabetes and, of these, 37 (22.2%) were found to have diabetic retinopathy. Seven people (4.3%) had developed diabetes before age 30. The mean duration of diabetes was 9.2 years. People with diabetes were significantly more likely to have visited an ophthalmologist ever or in the past 2 years than people without diabetes. However, 31.8% of people with diabetes had never visited an ophthalmologist. The proportion of people who had never seen an ophthalmologist was 47.1% for people without diabetes, 34.2% for people with diabetes but without diabetic retinopathy, and 25% for people with diabetic retinopathy. Sixty one per cent of people with diabetic retinopathy had seen an ophthalmologist in the past year and a further 3% within the past 2 years. People with diabetes were not significantly more likely to have visited an optometrist than people without diabetes (p=0.51). Overall, 37.7% of people with diabetes and 32.9% of people without diabetes had visited an optometrist within the past year (χ2=2.25, 1 df, p=0.13). Information concerning retinal examinations was available for 135 individuals (83.3% of people with diabetes). Only 74 (54.8%) could recall ever having a dilated fundus examination; 10 (14%) by an optometrist, 62 (86%) by an ophthalmologist, and five (7%) by a general practitioner. Of those 68 people who had seen an ophthalmologist in the past 2 years, 48 (71%) reported a dilated fundus examination during that time. This compares with 28 (43%) reported dilated fundus examinations in the 65 people who had seen an optometrist in the past 2 years. This finding is statistically significant (χ2=10.2, 1 df, p<0.005).
CONCLUSION These results indicate that nearly half of people with diabetes in Melbourne are not receiving adequate screening or follow up for diabetic retinopathy, despite universal health care.
- diabetes
- diabetic retinopathy
- screening guidelines
Statistics from Altmetric.com
Vision loss associated with diabetes is largely preventable with timely detection and treatment of diabetic retinopathy. Despite this, diabetic retinopathy remains a leading cause of blindness in Australians. There are about 350 000 people known to have diabetes in Australia and possibly another 350 000 who have not been diagnosed.1
Nearly all people with diabetes develop diabetic retinopathy within 20 years after diagnosis and approximately 10% of people with type II diabetes may have retinopathy at the time of diagnosis.2 3 There is a high rate of vision loss due to diabetic retinopathy when diabetes has been present for more than 30 years, with approximately two thirds of people having lost vision after 35 years of diabetes.4
Current treatments, if appropriately timed and rigorously applied, may be effective in preventing up to 98% of severe visual loss and blindness due to diabetic retinopathy.5-8 This emphasises the need to ensure that individuals with diabetes receive adequate screening and are offered timely treatment. Recommendations in Australia are for people with diabetes to have a dilated pupil examination at least every 2 years. People with signs of diabetic retinopathy, if not already seeing an ophthalmologist, should be referred to an ophthalmologist for further management.9
Prompt and effective delivery of ophthalmic care to people with diabetes not only reduces personal suffering caused by blindness but also yields substantial cost savings. Previous studies have shown that the costs of providing preventative eye care are much less than the costs involved with providing support for a subsequent disability.10-12
Studies from the United States have shown that current recommendations for periodic screening for diabetic retinopathy are not well adhered to.13-15 However, little research has been done in Australia to determine whether people with diabetes receive regular eye examinations in accordance with recommendations. Our recent study showed that most general practitioners do not examine the fundus of their patients with diabetes, but usually refer them to an ophthalmologist.16
The purpose of this study was to assess the use of eye care services in a representative sample of the Melbourne population aged 40 and over, comprising people with and without diabetes. Compliance with current guidelines for ophthalmic examination among the participants diagnosed with diabetes was evaluated.
Methods
THE MELBOURNE VISUAL IMPAIRMENT PROJECT
The assessment of eye care service utilisation in Melbourne and the relation of this to diabetic status was investigated as part of the Melbourne Visual Impairment Project (Melbourne VIP). Details of the methods have been reported previously and only a summary will be included here.17 The Melbourne VIP is a large population based epidemiological study designed to determine the distribution and determinants of eye disease, to investigate the impact of visual impairment on an individual and their activities of daily living and to examine the use of and barriers to current eye healthcare services including the need for and accessibility of these services. Nine metropolitan suburbs of Melbourne, each consisting of two adjacent census collector districts were randomly selected for the Melbourne VIP. Eligible residents were identified by private household census and those permanent household members aged 40 or older were classed as eligible. The Royal Victorian Eye and Ear Hospital human research ethics committee approved the study and informed consent was obtained from all participants.
A screening questionnaire was initially administered to identify households with eligible residents. Repeated visits were made to the home when respondents were not available. Eligible residents were asked some basic demographic details and were invited to attend an eye examination at a local temporary test site for a more comprehensive interview and ophthalmic examination. If residents were unable to attend the test site owing to some physical condition, a modified home visit was offered to obtain as much information as possible. Trained interviewers conducted the personal household interviews.
HISTORY OF USE OF EYE CARE SERVICES PROVIDED
Basic demographic and health service utilisation data were collected during the initial private household interview including details on the use of eye care services. Respondents were initially asked if they had noticed a change in their vision in the past 10 years. If they had, they were then asked if they had seen someone about it and, if so, who they had visited. If an optometrist or ophthalmologist was not included in their response, and for those who had not noticed a change in their vision, they were then asked specifically if they had ever seen an optometrist or an ophthalmologist. The year of the last visit to an optometrist and/or ophthalmologist was recorded. An explanation of the terms optometrist and ophthalmologist was given to participants where necessary. In Australia an ophthalmologist is medically qualified and is specifically trained to diagnose or treat eye disease whereas optometrists are specialists in the area of refraction and cannot diagnose or treat eye conditions such as cataract, age related macular degeneration, or glaucoma.
For the last four test sites, people who reported a previous diagnosis of diabetes were asked if they had ever had the back of their eye examined and if so who performed the examination and when it was last performed. People with diabetes who had been examined at the first five test sites were subsequently contacted by telephone and asked the same question.
HISTORY OF DIABETES
A comprehensive interview was performed at the test site to elicit information that included past medical history and medication use.17 One component of this interview elicited a previous diagnosis of diabetes. If a previous diagnosis of diabetes was reported, details were obtained on the year of diagnosis and on any medication either currently or previously taken for more than 12 months. For each medication taken, the type and number of years of use were recorded. The questions relating to diabetes and diabetic retinopathy have been validated and employed by Welborn et al.18 19
FUNDUS EXAMINATION
The clinical examinations were performed by one of the co-authors (YLS). Pupils were dilated with one drop of tropicamide (0.5%) and one drop of phenylephrine hydrochloride (10%).17 Ophthalmic examination of the fundus was performed with a slit lamp and 90 dioptre convex lens and supplemented by indirect ophthalmoscopy if peripheral abnormalities were revealed or suspected. Presence or absence of diabetic retinopathy was recorded. If diabetic retinopathy was detected, the eyes were clinically classified as having non-proliferative or pre-proliferative retinopathy, macular oedema, or proliferative retinopathy based on a shortened version of the classification system adopted by the American Academy of Ophthalmology20 (Table1).
Diabetic retinopathy classification
VISION ASSESSMENT
Presenting and best corrected distance visual acuity were measured using the ETDRS (Early Treatment of Diabetic Retinopathy) letter chart.17
ANALYSIS
Knowledge of diabetes status and clinical fundus examination were required for inclusion in subsequent analyses. The worse of the two eyes was used for classification of diabetic retinopathy status.
For the analyses, participants were divided into the following mutually exclusive groups: (1) people with diabetic retinopathy, (2) people with diabetes and no diabetic retinopathy, and (3) people without diabetes. They were also categorised as having seen or not seen an optometrist, an ophthalmologist, or both. Within these categories they were grouped by the number of years since they had last seen an optometrist or ophthalmologist.
Paradox Version 4.0 (Borland International, Scotts Valley, CA, USA) was used for storage and processing of subject records. Statistical analyses were performed with sas Version 6.09. The statistical procedures used in this research are documented inSAS/STAT user’s guide.21 A p value <0.05 was considered to be statistically significant.
Results
PARTICIPANT CHARACTERISTICS
A total of 3946 people were determined to be eligible. Of these, 3271 (83%) attended the test site or were examined at home because of limited mobility. The non-participants were significantly more likely to speak a language other than English in their own home, but did not differ significantly in any other respects.22
In all, 3189 (97.5%) people completed the full assessment required (knowledge of diabetes status and clinical fundus examination). Of the 82 with incomplete assessment, 10 people either did not participate in the interview or did not know if they had diabetes, six with diabetes did not have a fundus examination, and 66 without diabetes did not have a fundus examination. The reasons for no fundus examination were uncooperative behaviour, small pupils, or opaque ocular media. Of the 3189 people included in the analyses, 1482 (46.5%) were males. The age of the participants ranged from 40 to 98 years, with a mean of 58.6 (SD 11.3).
A total of 162 (5.07%) reported a previous diagnosis of diabetes. Only seven (4.3%) were diagnosed with diabetes at or before the age of 30. The mean duration of diabetes since diagnosis was 9.15 years (range 0–57 years, SD 9.26); 119 (73.5%) people with diabetes reported current medical treatment for their diabetes. For those 116 who could remember their treatment, 23 (19.8%) reported using insulin and 93 (80.2%) reported using oral hypoglycaemic agents. Diabetic retinopathy was detected in 37 (22.8%) people with diabetes (Table 2). Everyone identified with diabetic retinopathy had a previous diagnosis of diabetes.
Diabetic retinopathy prevalence in people with diabetes
USE OF EYE SERVICES
People with diabetes were significantly more likely to have visited an ophthalmologist ever or in the past 2 years than people without diabetes (Table 3). However, almost one third of people with diabetes had never visited an ophthalmologist. The proportion of people who had never seen an ophthalmologist was 47.1% for those without diabetes, 34.2% for those with diabetes but without diabetic retinopathy, and 25% for those with diabetic retinopathy (Fig 1). Sixty one per cent of people with diabetic retinopathy had seen an ophthalmologist in the past year and a further 3% within the past 2 years. This distribution of attendance at an ophthalmologist varied significantly by diabetes and diabetic retinopathy status (χ2 75.8, 6 df, p=0.001).
Ophthalmic and optometric examination by diabetes status
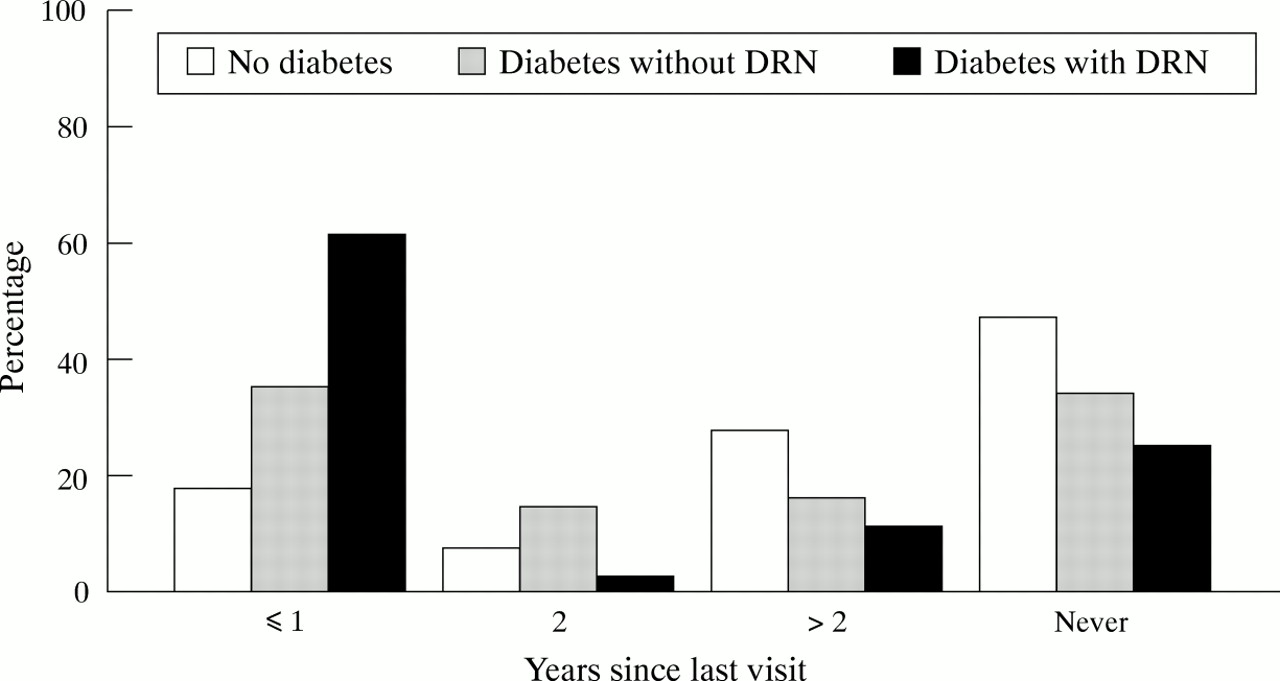
Years since last visit to an ophthalmologist by diabetes/diabetic retinopathy (DRN) status.
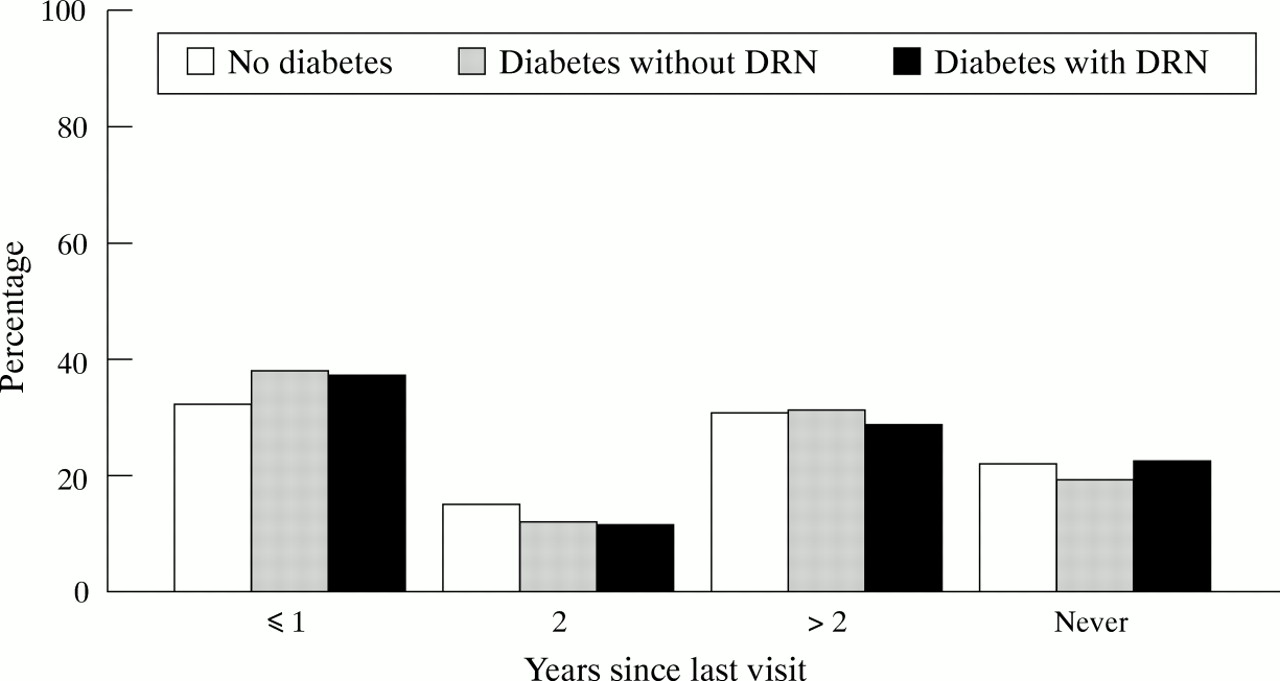
People with diabetes were not significantly more likely to visit an optometrist than people without diabetes (Table 3 and Fig 2). Overall, 37.7% of people with diabetes and 32.9% without diabetes had visited an optometrist within the past year (χ2=2.25, 1 df, p=0.13). The distribution of visits to an optometrist did not differ by diabetes or diabetic retinopathy status (χ2 3.10, 6 df, p=0.80).

{kind=link}
{kind=link}
Years since last visit to an optometrist by diabetes/diabetic retinopathy (DRN) status.
Some estimates for the frequency of retinal examinations are also available. Information concerning retinal examinations was available for 135 individuals (83.3% of people with diabetes). Only 74 (54.8%) could recall ever having a dilated fundus examination; 10 (14%) by an optometrist, 62 (86%) by an ophthalmologist, and five (7%) by a general practitioner. Of those 68 people who had seen an ophthalmologist in the past 2 years, 48 (71%) reported a dilated fundus examination during that time. This compares with 28 (43%) reported dilated fundus examinations in the 65 people who had seen an optometrist in the past 2 years. This finding is statistically significant (χ2 10.2, 1 df, p<0.005).
Discussion
These data indicate that nearly half of adults with diabetes in Melbourne are not receiving adequate 2 yearly screening for diabetic retinopathy. This is in contrast with our recent survey of general practitioners in which 88% of Victorian general practitioners reported referral of their patients with diabetes to an ophthalmologist at the recommended frequencies.16 The disparity in these results could be due to a reporting bias by the general practitioners, a breakdown in the referral chain, or a combination of the two.
Our results are generally consistent with findings from 2405 diabetic participants in the National Health Interview in the United States.13 Thirty four per cent of the people surveyed had not had a comprehensive eye examination, including pupil dilatation, in the past 2 years, and 20% had not had any eye examination during that time. No differentiation was made in that study between examination by an ophthalmologist or an optometrist. We might have expected to find higher rates of eye examinations in Australia than the United States because universal health care through Medicare exists in Australia. Provided patients visit public hospitals, they have no out of pocket expense for their retinal examinations in Australia. If they visit a private ophthalmologist and do not have private health insurance, they have to cover any gap in the scheduled Medicare fee and the amount billed by the ophthalmologist. Generally, the waiting time to see a private ophthalmologist is substantially less than to visit a public clinic.
Our results are also similar to those of the Wisconsin Epidemiological Study of Diabetic Retinopathy, which found that 50% of people with diabetes had not had an ophthalmic examination in the past 2 years.14 In the 10 year follow up of this study cohort, approximately 30% of people still had not had an eye examination in the last year.15 These results demonstrate that although treatment information has been available for many years, an appropriate level of care has still not been achieved.
Important characteristics of our study are that it is a population based, epidemiological study with a high response rate where a comprehensive eye examination has been performed on all participants, with and without diabetes, as well as collection of detailed information on the use of eye care services. The self reported 5.1% rate of diabetes in our study population is nearly identical to the rates reported in the 1989–90 National Health Survey in Australia.19 Researchers documented self reported rates of 2.91% in males aged 45–54 to a rate of 8.74% in people over age 75. These similarities further support the representativeness of our study population.
Only data on self reported diabetes have been collected in this study. There is estimated to be a high proportion of people in Australia with undiagnosed diabetes.1 18 19 It is believed that there is one case of undiagnosed diabetes for every known case.1These people would be even less likely to receive recommended eye examinations than people known to have diabetes. Therefore, our results probably overestimate the level of eye care received by the total population of adults who actually have diabetes.
Diabetic retinopathy status in our study was based on clinical assessment. Results from previous studies have shown good agreement between the methods of clinical assessment and fundus photography with a slight underestimation of diabetic retinopathy with clinical diagnosis.23 A recent study in Barbados found the prevalence of diabetic retinopathy by clinical grading was 7.7% compared with 8.7% with fundus photography.24
Primary prevention of diabetic retinopathy has been shown to be cost effective,10-12 but requires innovative public health strategies. Education of people with diabetes and their relatives is a key to encouraging more regular screening for diabetic retinopathy. People with diabetes must be made aware that early stage diabetic retinopathy can exist without visual symptoms and that early detection through regular dilated eye examinations can ensure timely diagnosis and treatment to preserve vision. Relatives of people with diabetes can help to encourage timely examinations.
Primary care providers play an important role in the coordination of care for people with diabetes. Greater continuity of patient care could be achieved if primary care providers regularly screened their diabetic patients for diabetic retinopathy or had a system in place to follow up on referrals made. Because people are more likely to see an optometrist than an ophthalmologist, it may be appropriate for optometrists to be more actively involved in screening people with diabetes for diabetic retinopathy. The use of a non-mydriatic camera to augment existing eye care services has also been suggested as a possible cost effective means of improving the screening rate for diabetic retinopathy among people with diabetes.23 25 26
In conclusion, people with diabetes in Melbourne do not receive adequate screening for the detection of diabetic retinopathy. Collaboration between eye care specialists and primary care providers, together with improved patient awareness of the risks and consequences of developing diabetic retinopathy, is essential to ensure that people with diabetes receive regular eye examinations to prevent vision loss.
Acknowledgments
Each author declares that he or she has no proprietary interest in connection with this study.
The work described in this paper was partially funded by the Victorian Health Promotion Foundation, the National Health and Medical Research Council, the Ansell Ophthalmology Foundation, and the Dorothy Edols Estate.