Article Text

Abstract
AIMS To determine whether there were any specific factors that influenced waiting list time (WLT) for patients undergoing cataract surgery.
METHODS 70 preoperative cataract patients were interviewed by one of the authors using a questionnaire to score visual acuity, coexisting ocular pathology and disabilities, threat to independent living/employment, and perceived visual handicap for detailed, gross, and driving vision. Individuals were analysed separately according to whether it was their first or second cataract operation.
RESULTS The median WLT for first eye surgery was 9 months (n = 31) and 13 months for second eye surgery (n = 36). The WLT ranged from 2 to 25 months for first eyes and 0.25–18 months for second eyes. Where there was a perceived threat to independent living or employment the WLT was found to be significantly shorter than the median. A high overall score correlated with a shorter WLT. Surgical priority was also given to individuals with anisometropia >3 dioptres.
CONCLUSION This study has demonstrated that there are specific factors that influence clinicians when prioritising patients for cataract surgery.
- cataract surgery
- waiting list time
Statistics from Altmetric.com
In a recent editorial in the BMJ and an article in the BJO, Gray and colleagues discuss the issue of waiting time for cataract surgery.1 2 How to ration or prioritise individuals on the cataract waiting list appears to be top of the ophthalmology agenda since almost every hospital is experiencing an ever increasing demand for surgery without any parallel increase in staffing or resources.
We carried out a survey to determine whether we could identify any factors that influenced the waiting time for cataract surgery among our patients.
Materials and methods
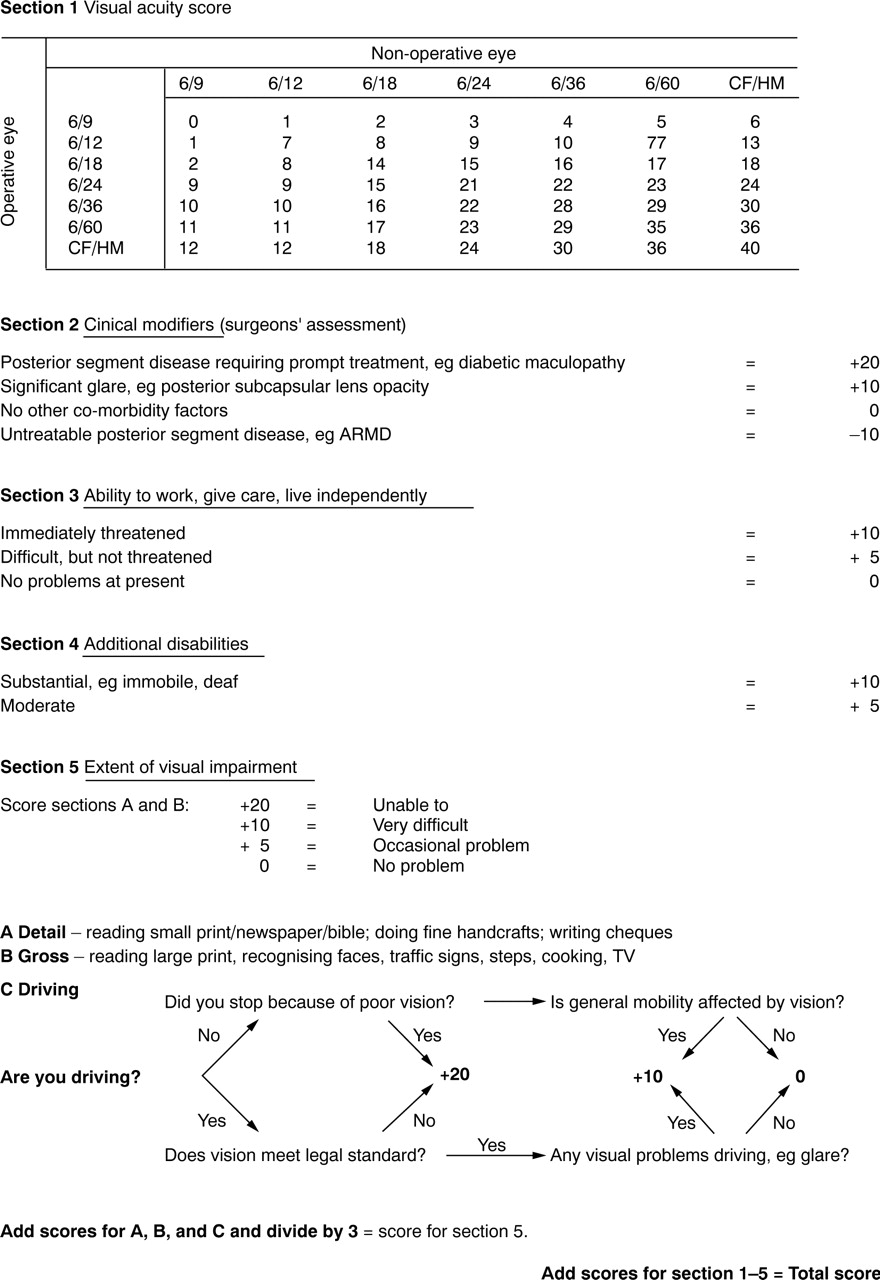
We asked local ophthalmologists what factors influenced their decision when deciding how to prioritise patients for cataract surgery. We identified a questionnaire (currently used in prescreening cataract clinics in New Zealand, unpublished data) which incorporated most of these factors and allocated a severity score to each. Seventy consecutive patients were interviewed preoperatively about the extent of their visual handicap using the questionnaire which consisted of five sections (Fig 1). The interview took between 2–3 minutes. Two non-English speaking and one confused patient were excluded. Section 1 assigns a score to the objective measure of visual acuity in each eye at the time of listing. Section 2 scores any coexisting pathology that might have relevance to the visual prognosis. Section 3 scores the perceived threat to independent living or employment because of the cataract. Section 4 scores any additional disabilities—for example, deafness, immobility. The final section measures the visual handicap that the patient experiences, with equal weighting given to detailed, gross, and driving vision. Patients were split into two groups according to whether this was their first or second cataract operation. Time spent on the surgical waiting list was recorded. Clinically significant anisometropia (>3 dioptres) was noted as some ophthalmologists felt this was an important factor in prioritising surgery.
{kind=link}
The visual function questionnaire used in this study.
Results
There were 31 “first” and 36 “second” eye patients. Three individuals had useful vision in only one eye and were not included in the analysis because, owing to their special circumstances, waiting time was reduced to 6 months or less.
The age ranges were as follows: 53–91 years in females (median = 76 years, n=15) and 28–92 years in males (median = 74 years, n=16) for first eyes; 62–95 years in females (median = 78 years, n=19), 47–92 years in males (median = 81 years, n=17) for second eyes. The waiting list time (WLT) ranged from 2 to 25 months for first eyes (median 9 months, mean 10 months) and 1 week to 18 months (median 13 months, mean 10 months) for second eyes. Using the Spearman's rank correlation test no correlation was found between the waiting time and age (r = 0.107, p = 0.391 where n = 67).
The overall totalled scores ranged from 9 to 51 (median 24, mean 25) for patients undergoing first eye surgery and −5 to 41 (median 9, mean 13) in those having their second cataract removed (a minus score indicating untreatable posterior segment pathology). A negative correlation, r, was found between WLT and the totalled score in males undergoing first eye surgery (r = −0.614, p = 0.011 where n = 16) indicating that the higher the score the shorter the WLT. This was not the result of an unusually high score in any of the individual sections in this group.
When each individual section was analysed, only one factor, scored by section 3, produced an overall correlation with WLT (r = −0.343, p = 0.004, where n = 67). This was most obvious among females undergoing second eye surgery (r = −0.468, p = 0.043 where n = 19). Section 3 rates the perceived threat to independent living and employment, illustrating that when the score is high the WLT is reduced. None of the other sections, including visual acuity, showed any correlation with the WLT.
Nine individuals had clinically significant anisometropia of >3 dioptres. Their WLT ranged from 0.25 to 16 months, median time 4 months. Anisometropia >3 dioptres was the most important objective reason for expediting surgery in our group of patients.
Discussion
We used a questionnaire based assessment to score the severity of the cataract in individuals about to undergo surgery. This allowed us to determine what factors, if any, influenced prioritisation for surgery. This sample of patients was taken from consecutive surgical sessions (representing three consultants) and therefore reflects the amalgamated views of several clinicians. All consultants had waiting lists of similar duration. The fact that one section, a perceived threat to independent living or employment, shows statistical correlation with WLT suggests that all clinicians placed greater importance on this.
There was a weak negative correlation between the totalled scores and WLT which merely indicates that the more severe the overall visual handicap, general disabilities, or coexisting factors were, the more rapidly cataract surgery was performed. This partly corroborates a previous study where 27 consultants interviewed felt that the level of visual handicap was more important than the visual acuity alone when prioritising cataract patients.3
One third of the 67 patients analysed were drivers. For those undergoing first eye surgery the median WLT for drivers was 13 months compared with 9 months for the group overall. Second eye surgery was carried out sooner in drivers (median WLT was 9.5 months in drivers compared with 13 months overall). These conflicting data probably indicate that within our department there is no group policy regarding drivers and prioritisation for surgery.
The median WLT for second eye surgery was 13 months compared with 9 months for first eyes. There have been several studies to show the benefit of second eye surgery4 5 and we do not feel that “first eye surgery only” should be practised. Given the current constraints on operating sessions, however, one should consider first eye surgery to have a degree of priority over second eyes. A solution might be parallel first and second eye waiting lists so that operating lists could be planned to take this into account.
Understandably, prioritisation is a very emotive subject among our patients and one that needs to be addressed urgently. Most people recognise that there are long waiting lists for cataract surgery and, while not happy about it, accept that resources are limited. The frustration felt by patients is compounded by the long wait, sometimes up to 9 months, for their first appointment in the outpatient clinic. The total waiting time could be reduced if ophthalmologists address what factors are important in prioritising cataract patients. General practitioners, practice nurses, or optometrists could use such a questionnaire to include this information in their referral letters. It would then be possible for patients to be prioritised to cataract prescreening clinics more appropriately from the outset.
Acknowledgments
The authors wish to thank Vicki Allgar for her help in the statistical analysis of the results.