Article Text

Abstract
AIMS Corneal perfusion chambers are important tools in the development and assessment of ophthalmic drugs. The aim of this study was to design and test a modified perfusion chamber suitable for topical application of drugs to isolated corneoscleral preparations, and which allowed continuous monitoring of endothelial cell function.
METHODS A polycarbonate and stainless steel perfusion chamber was designed to clamp corneas in a horizontal plane suitable for topical drug delivery. Endothelial cell function was assessed by ultrasonic pachymetry and specular microscopy during perfusion. Epithelial barrier function was assessed by penetration of fluorescein. Leakage was examined by measuring penetration of a large protein, IgG. Tissue architecture after perfusion was examined by conventional histology.
RESULTS Corneas maintained a functionally and morphologically intact endothelial monolayer during perfusion periods of up to 14 hours. The epithelial barrier function was well preserved. The tissue clamp sealed the preparation effectively against leakage of macromolecules.
CONCLUSION The new chamber device forms a reliable tool for in vitro drug penetration and toxicity studies in isolated perfused corneoscleral tissue.
- cornea
- perfusion chamber
- drug penetration
Statistics from Altmetric.com
In vitro drug penetration and endothelial toxicity studies on isolated corneoscleral preparations are important for developing and testing ophthalmic drugs, drug vehicles, and irrigation solutions.1-10 We describe a modified, simple perfusion chamber that allows the topical application of drugs in eye drop formulations to corneal epithelium over periods of up to 14 hours. The corneoscleral preparation is mounted horizontally in the chamber between an air interface on the epithelial side and an artificial fluid filled anterior chamber on the corneal endothelial side. An appropriate positive pressure gradient is applied. The chamber design allows direct visual and functional assessment of the endothelial cells by specular microscopy and ultrasonic pachymetry, respectively, at any stage during perfusion and drug delivery.
Materials and methods
CORNEAL PERFUSION CHAMBER
The perfusion chamber was constructed from polycarbonate and consisted of the main body, a clamping sleeve, and a fixation ring (Fig1). The central cavity of the main body was 12 mm in diameter and 3 mm in depth and, together with the mounted cornea, formed the artificial “anterior chamber”. The main body contained channels for inflow and outflow perfusion lines and an additional drainage channel that connected with a channel in the clamping sleeve. This channel allowed removal of excess fluid after topical application, mimicking lacrimal drainage. Corneoscleral preparations were placed over the central cavity of the main body and secured with the clamping sleeve, which covered both sclera and peripheral cornea. The sleeve had two stainless steel guide pins to direct its vertical movement without twisting, minimising sheer stress and edge damage to the cornea. The fixation ring secured the sleeve and the underlying cornea to the main chamber, creating a tight seal. The fixation ring had a 1 mm pitch thread to allow precise adjustment of the clamp. A construction plan for the perfusion chamber is shown in Figure 2 (more detailed plans are available from the authors).

Corneal perfusion chamber shown without a mounted cornea. The clamping sleeve sits on top of the main body. The fixation ring that screws onto the main body is shown on the left.

Chamber design: (A) main body, (B) clamping sleeve, and (C) fixation ring. All parts were made of polycarbonate and stainless steel. Corneas are clamped between the main body and the clamping sleeve.
CORNEAL PERFUSION USING THE CHAMBER
Normal pig eyes were obtained from a local abattoir, transported to the laboratory at 4°C, and used within 2–3 hours of enucleation. Eyes had not been heat treated in the abattoir in any way. Any eye with a collapsed anterior chamber was discarded. Corneoscleral buttons were dissected using standard eye bank techniques, care being taken to minimise tissue distortion. The preparation was mounted in the perfusion chamber and the inflow tube was attached to a peristaltic pump. Corneas were perfused with BSS-Plus (Alcon Laboratories, Frenchs Forest, NSW, Australia) at a flow rate of 1 ml/min. The perfusate from the outflow tube was collected in a reservoir and recirculated back into the chamber. The total fluid volume recirculating through the chamber, tubing, and reservoir was 4 ml. The reservoir was elevated 25 cm above the level of the clamped cornea to create a positive pressure of 18 mm Hg inside the artificial anterior chamber, simulating physiological conditions. The perfusion chamber was surrounded with a brass heat exchange block through which warm water circulated from a 40°C water bath to maintain a chamber temperature of approximately 35°C. The corneal epithelial surface was kept moist by applying BSS-Plus eye drops every 20 minutes. Excess fluid was removed through the drainage channel. A glass slide was used to cover the top opening of the chamber on the epithelial side to create a humid chamber, reduce evaporation when measurements were not being taken, and prevent drying of the corneal surface.
ASSESSMENT OF THE CORNEAL PENETRATION BARRIER
Corneas were equilibrated with BSS-Plus for 45–60 minutes before the start of the experiments. In some instances, corneal epithelium was removed before perfusion by scraping the epithelial surface with a scalpel blade. Preservative-free sodium fluorescein eye drops (2% w/v Minims, Chauvin Pharmaceuticals Ltd, Essex) were applied to the corneal epithelium at the rate of 50 μl every 20 minutes. Each hour, 200–250 μl perfusate was removed from the reservoir for analysis and replaced by the same volume of fresh BSS-Plus. No correction was applied for the dilution of fluorescein that occurred when a sample was removed for testing and was replaced by fresh BSS-Plus. Penetration of fluorescein through the cornea into the perfusate was measured in duplicate 100 μl samples of perfusate aliquoted into ELISA plates. The optical density at 492 nm of the samples was compared with those of dilutions of a fluorescein standard on the same plate. The detection threshold for fluorescein was 250 ng/ml. To assess the tightness of the tissue clamp, supernatant from a growing culture of OX38 hybridoma (European Collection of Animal Cell Cultures) containing 1 μg/ml of mouse IgG with specificity for rat CD4 was applied topically to the epithelium every 20 minutes. Penetration of IgG through the cornea was measured by high sensitivity flow cytometry11 on normal rat thymocytes, which are CD4 positive. The sensitivity of detection was 1 in 30 000; replicates were assayed and mean fluorescence intensity recorded.
ASSESSMENT OF CORNEAL TISSUE VIABILITY
Tissue viability was assessed by measuring corneal thickness every 60 minutes with a hand held ultrasonic pachymeter (BV International, Clermont-Ferrand, France). During the initial equilibration period, three or more pachymetry measurements were taken every 15 minutes to identify corneas with compromised endothelial pump function (two of 23 corneas had to be replaced before the start of the experiment). Once an experiment had been initiated, an increase in corneal thickness of more than 10% compared with the initial value was regarded as reflecting endothelial dysfunction and the experiment was discarded (one of 23 experiments). Endothelial cell photography was performed with the Keeler-Konan contact specular microscope using 320 ASA Kodak tungsten slide film. At the end of each experiment, corneoscleral buttons were fixed in buffered formalin, embedded in paraffin, and cut at 10 μm. Sections were stained with periodic acid Schiff and examined by light microscopy.
Results
PACHYMETRY DURING CORNEAL PERFUSION
Eight pig corneas were perfused with BSS-Plus and the corneal thickness was measured hourly by ultrasound pachymetry for 4–14 hours. Initial mean pachymetry values were 729 μm (SD 59) μm. The maximum observed increase from baseline in any individual pig cornea at any time point was less than 10% (Fig 3). The experiment was repeated on four normal cat corneas with similar results: corneal thickness increased by no more than 10% over an 8 hour observation period (data not shown). After an initial perfusion period of 60 minutes, the endothelium of one pig cornea was intentionally destroyed by a 60 second perfusion with 100% ethanol before the perfusion was continued with BSS-Plus. Endothelial destruction was followed by a rapid increase in corneal thickness within 15 minutes and the corneal thickness almost doubled from its baseline level during the following 4 hours (Fig 3).

Corneal thickness (mean (SD)) as measured by pachymetry plotted against perfusion time for isolated perfused pig corneas mounted in the modified perfusion chamber. Toxic destruction of the endothelium by a brief perfusion of ethanol resulted in irreversible tissue swelling.
SPECULAR MICROSCOPY DURING CORNEAL PERFUSION
The morphological integrity of the endothelial monolayer was examined by specular microscopy in three pig corneas during perfusion. Representative photographs of endothelium in a freshly enucleated whole eye and in a cornea after 4 hours of perfusion with BSS-Plus in the perfusion chamber are shown in Figure 4A and B, respectively. Minimal cell damage was observed.
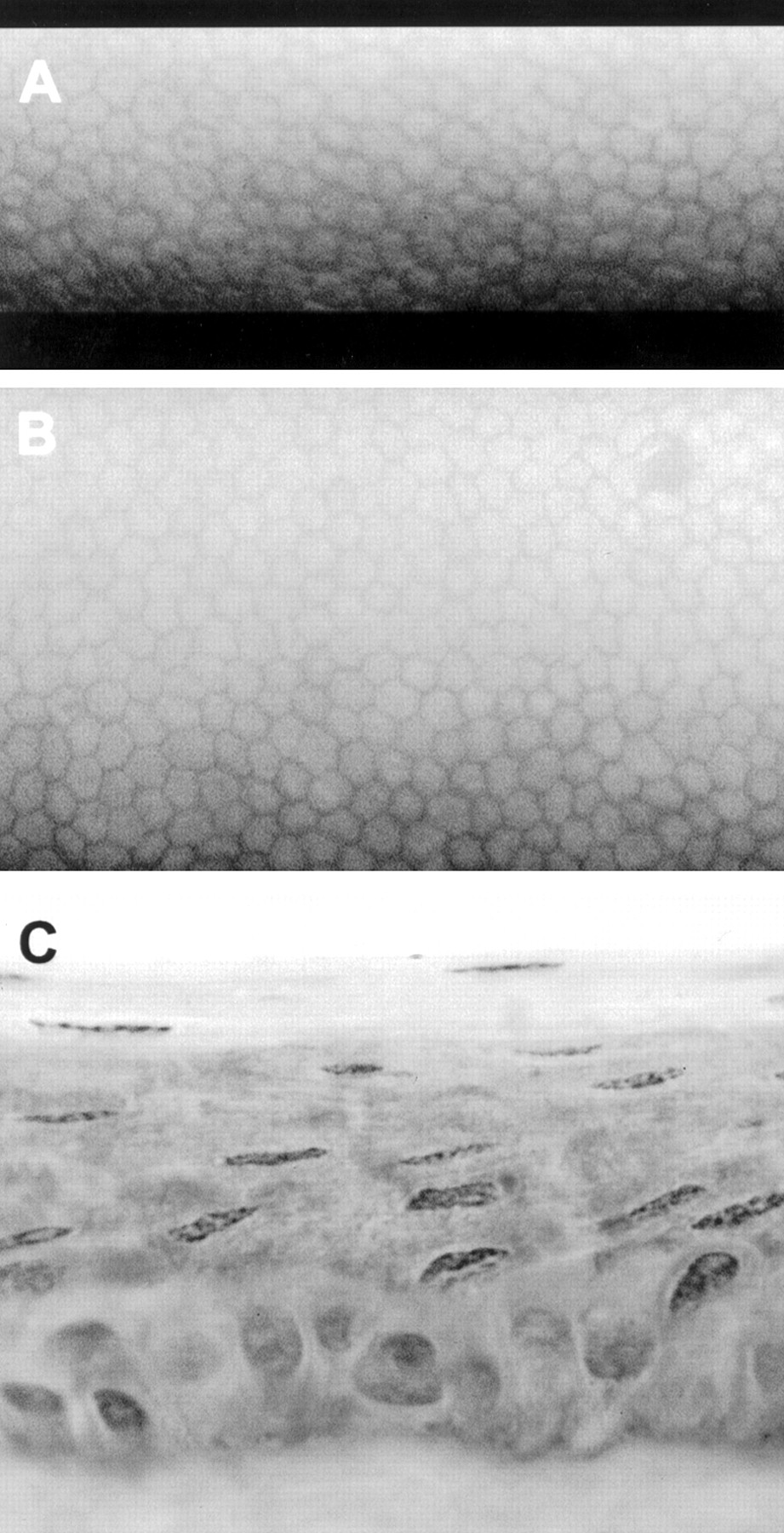
Specular microscopy (A, B) and histology (C) of a perfused pig cornea. (A) Endothelium before tissue dissection, (B) endothelium after 4 hours of perfusion (magnification ×40), (C) epithelium after perfusion for 10 hours, topical BSS eye drops every 20 minutes (periodic acid Schiff stain, magnification ×100).
ASSESSMENT OF CORNEAL BARRIER FUNCTION
Penetration of sodium fluorescein was measured in three corneas with epithelium and in four corneas after removal of epithelium. In corneas with preserved epithelium, fluorescein became detectable in the perfusate after 3 hours and increased slowly thereafter in a linear fashion over the experimental period of 10 hours (Fig 5). In corneas without epithelium, fluorescein was detectable in the perfusate 15 minutes after application of the first drop and increased thereafter 200 times faster than in corneas with preserved epithelium (Fig5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fluorescein penetration (mean (SD) of replicate determinations) through pig corneas with or without epithelium. No correction was applied for the dilution of fluorescein that occurred when a sample was removed for testing and was replaced by fresh BSS-Plus. The epithelial barrier was well preserved over the perfusion period of 10 hours.
EFFECTIVENESS OF THE CORNEAL CLAMP
Three corneas without epithelium were exposed to topically applied anti-CD4 IgG antibody three times an hour for 4–14 hours. No IgG binding activity was observed in the perfusate for up to 14 hours, indicating that the corneal clamp formed an effective seal against leakage into the perfusion chamber (data not shown).
END POINT HISTOLOGY
End point histology of six pig corneas showed intact corneal epithelium after 14 hours of perfusion. The epithelium was compressed in the area of the clamp but the superficial epithelial cells appeared well preserved (Fig 4C). The basal and intermediate epithelial cells seemed to have been forced laterally to the side of the clamping point. The corneal stroma, Descemet's membrane, and corneal endothelium were intact.
Discussion
An ideal perfusion chamber should allow perfusion of an isolated cornea for a substantial period, with maintenance of a viable corneal endothelial monolayer and an intact epithelial barrier function. The chamber must not leak around the clamp. We describe a modified corneal perfusion chamber that meets these essential criteria, that permits topical application of drugs to the corneal epithelium at an air epithelial interface, and that has the advantage that assessment of endothelial pump function can readily be performed throughout perfusion.
To assess the function of the perfusion device described, the viability of corneal endothelium during perfusion was confirmed by regular pachymetry and specular microscopy over periods of up to 14 hours. The thickness of corneas perfused for 14 hours increased by less than 10% over baseline values, indicating that the corneal endothelial cell pump function was capable of maintaining appropriate tissue hydration despite a positive perfusion pressure of 18 mm Hg.
Specular microscopy performed during perfusion experiments showed morphologically well preserved endothelial cells. Destruction of endothelial cells by brief perfusion with ethanol resulted in an immediate and progressive corneal swelling. The perfusate in our device was not continuously aerated. Instead, 200–250 μl of the total perfusate volume was replaced every hour, mimicking to some extent the normal human aqueous humour turnover of 120–300 μl per hour. This design simplification clearly permitted supply of enough glucose and oxidised glutathione to maintain endothelial cell function.
Fluorescein is commonly used in humans to investigate epithelial barrier function.12 The integrity of the epithelial barrier in isolated corneas perfused in our device was tested by applying fluorescein topically as an eye drop. Fluorescein was first detected in the perfusate after a time lag of 3 hours, followed by a slow increase until the end of the experiment at 10 hours. Destruction of the epithelial barrier resulted in a 200-fold increase in penetration of fluorescein into the artificial anterior chamber. The low permeability of normal corneas to fluorescein over periods of 10 hours indicated that the epithelial barrier was well preserved during tissue dissection, mounting on to the chamber, and subsequent perfusion.
Potential leakage through the chamber was excluded by confirming that IgG, a molecule known to penetrate the cornea only within days to weeks,13 did not penetrate through the perfused cornea over periods of up to 14 hours when applied topically. Even after removal of the epithelium, no IgG was detected in the perfusate of three corneas perfused for up to 14 hours, indicating that the tissue clamp performed reliably. End point histology of perfused corneas showed that the tissue was well preserved.
There are several basic designs of corneal perfusion chamber. In Ussing-type chambers, the corneal tissue is clamped in the vertical plane between two perfusion baths.146-9 Drugs are added to one bath (usually on the corneal epithelial side of the chamber) and corneal penetration is assessed by measuring drug concentration in the other bath (usually on the corneal endothelial side of the chamber). Endothelial cell viability is assessed at the end of the experiment by calculating tissue hydration from wet and dry tissue weights. This basic chamber design has some disadvantages in that the corneal epithelium is continuously immersed in a stirred bath, and the pump function of the endothelial monolayer can only be assessed after drying the cornea at the experimental end point, an error prone method at best.14 Further, it can be difficult to achieve the pressure gradient across the perfused tissue that is essential for normal function. A modified chamber in which the cornea was clamped in the horizontal plane was described by Dikstein and Maurice.2 The design permitted specular microscopy of the corneal endothelium to be performed but the corneal surface was covered with silicone oil, excluding direct topical application of drugs as eye drops. The modifications of Krohn and Breitfeller3involved use of a humid chamber (rather than a bath) on the epithelial side of the cornea, but the clamping device did not allow ready assessment of corneal endothelial cell viability by corneal pachymetry or specular microscopy.
In the modification described here the cornea is clamped in a horizontal plane, the epithelial surface of the cornea is exposed to air in a humid chamber rather than being immersed in a perfusion bath, the design of the clamp allows access for a pachymeter probe or specular microscope cone, and a constant perfusion pressure in the range of 8–25 mm Hg can easily be maintained. Topical application of individual eye drops is straightforward. In our experiments we recirculated the perfusate, but a single pass system could equally well have been used. Our chamber is similar to the device described by Bourne and his colleagues,10 but is somewhat simpler. A stirrer was not found to be necessary for the perfusate (a benefit of the relatively high perfusion rate). The inclusion of a port for drainage of solutions applied to the epithelial surface was found to be a helpful modification. We have shown that the penetration chamber is suitable for both pig and cat corneas, and the dimensions of the device are such that it should also be useful for the human cornea, for which it was originally designed.
Acknowledgments
The authors thank Angela Chappell for expert assistance with photography. This work was supported by the NH&MRC of Australia, the Ophthalmic Research Institute of Australia, the Flinders Medical Centre Foundation, the Swiss National Science Foundation, EMDO Foundation and the Swiss Foundation for the Prevention of Blindness.