Article Text

Abstract
AIM To examine the efficacy, safety, and long term outcomes of amniotic membrane transplantation for corneal surface reconstruction in cases of partial limbal stem cell deficiency.
METHODS 17 eyes of 15 patients with partial limbal stem cell deficiency underwent superficial keratectomy of the conjunctivalised corneal surface followed by amniotic membrane transplantation. Cases were followed up for at least a year.
RESULTS All eyes exhibited a stable, intact corneal epithelial surface after a mean follow up period of 25.8 months with no eyes developing recurrent erosion or persistent epithelial defect. The mean time to re-epithelialisation was 22.8 days. Overall improvement in visual acuity was observed in 92.9% of 14 eyes with visual potential. Of those, five eyes gained six or more lines, two eyes gained between four and five lines, six eyes gained between one and three lines, and one eye lost three lines of Snellen acuity. Pain and photophobia were abolished in 86% of cases and substantially reduced in 14%, with all eyes exhibiting decreased vascularisation and inflammation at final follow up.
CONCLUSIONS Amniotic membrane transplantation appears to be a safe and effective method of restoring a stable corneal epithelium for cases of partial limbal stem cell deficiency and can be considered as an alternative to limbal autograft or allograft.
- amniotic membrane
- cornea
- transplantation
Statistics from Altmetric.com
Corneal epithelial stem cells are located at the limbus,12 which is the anatomical junction between the corneal and conjunctival epithelia. This specialised area harbours a unique stromal microenvironment that is crucial for the survival and function of corneal epithelial stem cells (reviewed by Tseng3). Diseases that destroy limbal epithelial stem cells or their stromal microenvironment can lead to limbal stem cell deficiency (LSCD) (for reviews see Tseng3 and Tseng and Sun4). Patients suffering from LSCD complain of photophobia and reduced vision as a result of recurrent or persistent corneal epithelial defects. Histopathologically, LSCD is characterised by progressive invasion of conjunctival epithelial cells onto the cornea, superficial vascularisation, destruction of the corneal basement membrane, and chronic inflammatory cell infiltration.5 These pathological changes explain why corneas characterised by LSCD are not good candidates for conventional keratoplasty.
Whether LSCD involves only part of the limbus (termed partial LSCD) or the entire limbus (termed total LSCD) of one eye, an autologous source of limbal epithelial stem cells can be transplanted. This procedure has been shown to restore the corneal surface more effectively than conjunctival transplantation in a rabbit model,6 and has been practised successfully by many to relieve the ocular discomfort experienced by many patients and to restore their vision and corneal surface.7-21 One major concern, however, about the autologous transplantation of limbal epithelial stem cells is the wellbeing of the donor fellow eye, from which one third to a half of the limbal circumference has been removed. The possibility of future abnormal corneal epithelial wound healing has been raised following the observation that rabbit corneas with similar limbal removal develop LSCD when the central corneal epithelium is subsequently removed.2223 Although this complication has not been observed in most of the clinical reports cited above (also reviewed by Holland and Schwartz24), a recent report of three cases did show that the donor eye developed pseudopterygium.25 This potential complication may also apply to the use of limbal epithelial stem cells obtained from an allogeneic source—that is, HLA matched living donors.121326 One solution, which does not risk compromise of the donor eye, is the use of limbal epithelial stem cells obtained from non-matched cadavers.121727-30 Both techniques of allogeneic transfer, however, carry with them the potential for systemic toxicity arising through the use of cyclosporin A121727-29 or FK50630 which is necessary, and probably needs to be used indefinitely, to prevent allograft rejection. Even with the use of systemic immunosuppression, the success rate for keratolimbal allografts declines from 75% to 85% in the first year to 50% in the third year.31
An alternative solution to these issues is to perform amniotic membrane transplantation (AMT). We have previously reported our preliminary experience32 demonstrating that AMT can help to restore corneas with partial LSCD without the transplantation of limbal epithelial stem cells. As no specific marker for limbal stem cells has been described, and the maximum lifespan of transient amplifying cells (corneal epithelial basal progenitor cells committed to epithelial cell differentiation) is thought to be between 3 and 6 months, the best indication that successful stem cell function has been restored is the presence of a normal corneal epithelium for at least 1 year following a transplantation procedure. In the present study, we provide evidence that preserved amniotic membrane is a suitable matrix to maintain and expand limbal epithelial stem cells in vivo and is capable of restoring and maintaining the long term stability of an intact and stable corneal epithelial surface.
Methods
PATIENTS
All patients were enrolled under a protocol approved by the medical science subcommittee for the protection of human subjects in research of the University of Miami School of Medicine, Miami, FL, USA. Written informed consent was obtained from each participant following the explanation of the nature, risks, and possible adverse consequences of the procedure according to the tenets of the Declaration of Helsinki. To ensure standardisation, one surgeon (SCGT) performed all surgery at the Bascom Palmer Eye Institute (BPEI), Miami, USA, between July 1996 and January 1999. All of the 17 consecutive cases exhibited partial LSCD with between 90° and almost 360° of limbal involvement, and were followed up for a minimum period of 12 months after AMT. The diagnosis of LSCD was made either clinically by the loss of limbal palisade of Vogt33 or in selected cases by the demonstration of goblet cell mucin at the corneal surface using impression cytology as previously reported.3234 The aetiologies of LSCD included chemical burns (eight eyes), idiopathic causes (three eyes), multiple surgery (two eyes), contact lens related keratopathy (two eyes), radiation induced LSCD (one eye), and conjunctival intraepithelial neoplasia (one eye) (Table 1). Among these 17 eyes, 12 did not have previous surgery while five eyes had between one to five previous surgeries or radiation therapy.
Clinical characteristics of patients with partial limbal stem cell deficiency
AMNIOTIC MEMBRANE TRANSPLANTATION
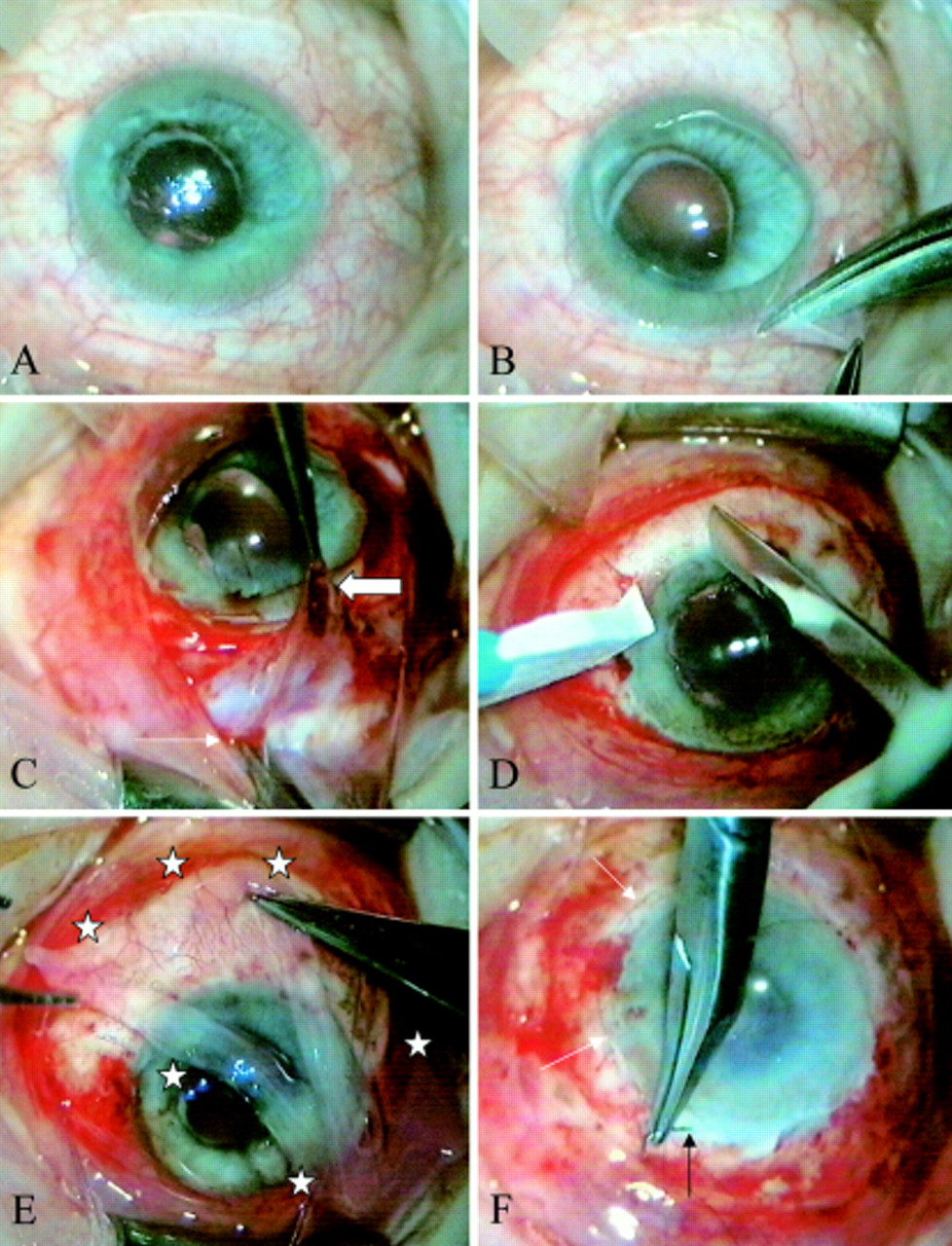
Preserved human amniotic membrane (AM) was obtained from Bio-Tissue (South Miami, FL, USA) following methods previously been described323536 from donors3236seronegative for HIV, human T cell leukaemia virus, hepatitis B virus, hepatitis C virus, and syphilis at delivery and 6 month post partum. All patients, apart from one child who received a general anaesthetic (case No 2), were anaesthetised using a retrobulbar block. Several drops of 1:1000 adrenaline (epinephrine) were initially applied to the ocular surface to prevent excessive bleeding. The intact corneal epithelium and adjacent healthy limbal epithelium were then protected by Healon (Pharmacia, Kalamazoo, MI, USA). A conjunctival peritomy was performed at the limbus only in the area of LSCD (Fig 1A and B) and subconjunctival fibrotic tissue was removed (Fig 1C), usually resulting in a conjunctival recession of 5–7 mm from the limbus. In cases of subtotal LSCD the peritomy was extended to 360° of the limbus. This conjunctival recession enabled the identification of a surgical plane between the fibrovascular corneal pannus and the underlying episclera so that a superficial keratectomy could be performed by blunt dissection over the involved corneal surface (Fig 1D). Following thaw at room temperature, AM was removed from its storage medium, peeled from the nitrocellulose backing paper to which its stromal surface was adherent, and placed over the healthy limbus and adjacent cornea (that is, with an intact epithelium) with the basement membrane side facing up (Fig 1E). Adherence of the membrane to the touch of a Weckcel sponge (Edward Weck & Company, Inc, NC, USA) verified the stromal side and was used to orient AM. The membrane was sutured into place with interrupted 10/0 nylon bites to the cornea if LSCD involved less than 2 clock hours, or a purse string suture if more than 2 clock hours. A running purse string suture with 10/0 nylon was placed at the sclera 2–3 mm from the limbus with episcleral bites (Fig 1F) so that the membrane was tightly adherent on the entire corneal surface. 10/0 Nylon or Vicryl interrupted sutures were also placed between the AM and the recessed conjunctiva after the excess membrane was trimmed. Topical neomycin/polymyxin B/dexamethasone suspension (Alcon, Ft Worth, TX, USA) was instilled and the eye patched. From the first postoperative day patients were treated with topical preservative free methyl prednisolone (BPEI pharmacy) or prednisolone acetate 1% (Allergan, Irvine, CA, USA) four times a day and ofloxacin 0.3% (Allergan, Irvine, CA, USA) three times daily. The latter was discontinued when complete epithelialisation was noted, while the former was tapered off over the course of 1–2 months. Patients were followed with particular attention to the clinical and photographic documentation of inflammation and revascularisation.

Intraoperative steps of amniotic membrane transplantation (AMT). A nearly total limbal stem cell deficiency (LSCD) was noted in case No 14 (A). Following application of Healon to protect the remaining central corneal epithelium, a conjunctival peritomy was performed at the limbus in the area of LSCD (B). While elevating the conjunctival edge (thin white arrow), subconjunctival fibrous tissue (thick white arrow) was excised (C). A superficial keratectomy was performed to excise the peripheral corneal pannus (D). AM (outlined by white stars) was placed to cover the corneal epithelium and the perilimbal scleral defect (E). A purse string 10/0 nylon suture (white arrows) was used to secure the membrane to the perilimbal region (black arrow) and tightly adherent onto the corneal surface (F).
Results
A total of 17 eyes of 15 patients underwent AMT for partial LSCD and each was followed up for more than 1 year with a mean period of 25.8 (SD 2.5) months. Nine patients were male and six female with a mean age of 42.3 (4.6) years (Table 1). The extent of the LSCD involved from 90° to nearly 360° of the limbus. In two cases (Nos 14 and 15) of nearly 360° of limbal involvement the central corneal epithelium appeared intact and clear. Surgery was uneventful in all cases; in particular there were no episodes of postoperative graft infection or rejection. All eyes showed less inflammation and vascularisation immediately postoperatively, and this effect was maintained or improved over the entire follow up period (for examples see Fig 2B, D, F, H) even in those whose stromal vascularisation recurred with time (patient Nos 2, 4, 7, and 10). In the 10 eyes in which it was recorded, the mean time to complete corneal and conjunctival epithelialisation was 22.8 (5.0) days. All eyes maintained a smooth and stable corneal epithelial surface at the last follow up visit without recurrent erosion or persistent epithelial defect. As a result, visual acuity was improved in the large majority of cases. Excluding those whose visual potential was limited by pre-existing or concomitant disease (case No 2 by radiation induced optic neuropathy, case No 9 by total retinal detachment, and case No 12 by established age related macular degeneration), visual acuity improved in 13 eyes (92.9%) and decreased in one eye (7.1%) of the remaining 14 eyes. Of these cases, five eyes (38.5%) gained at least six lines, two eyes (15.4%) gained four to five lines, and six eyes (46.2%) gained one to three lines of Snellen acuity. The one eye of case No 3 lost three lines; this eye suffered from a bilateral alkali burn and had previously undergone a rotational autopenetrating keratoplasty followed by a conjunctival flap. The cause was due to progression of central corneal fibrosis and thinning after AMT. Of the 14 cases with the complaint of pain or photophobia, these symptoms completely resolved in 12 cases (85.7%) and significantly reduced in two cases (14.3%). One patient (case No 9) underwent evisceration for phthisis bulbi 14 months following AMT. Owing to trauma induced dislocation, the AM had to be replaced in the child (case No 2). Postoperative complications were minimal and included the removal of loose sutures and in one case temporary treatment with systemic cyclosporin A for an idiopathic inflammatory reaction between the AM edge and the host conjunctiva. In particular no cases of inadvertent perforation or elevated intraocular pressure occurred.

Comparison of preoperative (left panels) and postoperative (right panels) corneal appearance following AMT. Patient No 8 complained of severe photophobia and decreased vision. Bilateral contact lens induced LSCD involved 300° of the right limbus (A) and 270° of the left limbus (C). Following AMT, a clear, smooth, and avascular epithelial surface was noted in the right cornea 23.5 months (B) and in the left cornea 21 months postoperatively (D). Patient No 4 with 270° of LSCD due to a chemical burn (E) resulting in prominent vascularisation (delineated by white stars) and an irregular epithelium (white arrows) affecting the visual axis. 23 months after AMT, the cornea became less inflamed and vascularised with residual stromal haze (white arrows) (F). Patient No 12 with CIN (white star) involving 330° of the limbus (G). Following excision of the lesion, removal of fibrovascular pannus, and AMT, the cornea became avascular, smooth, and stable 6 months postoperatively (H). Black arrow indicates the limbal running 10/0 nylon suture.
REPRESENTATIVE CASES
Case 13
A 28 year old woman sustained a chemical burn to her left eye resulting in photophobia, decreased vision and sustained hyperaemia, the right eye was unaffected. At presentation the best corrected visual acuity (BCVA) was 20/25 left eye with a mild ptosis. Slit lamp examination revealed loss of the palisades of Vogt and fibrovascular pannus invading the peripheral cornea for 300°; the central cornea was intact and clear (Fig 3A). The diagnosis of partial LSCD was made clinically and the patient underwent AMT. At surgery, a peritomy was performed in the area of the LSCD and subconjunctival fibrous tissue that appeared to be the worst, followed by a conjunctival recession of between 5–7 mm from the limbus. Using this plane, fibrovascular pannus was excised from the cornea by blunt dissection and an AMT graft placed over the defect only using interrupted 10/0 Vicryl sutures over the resected sclera and completed with a 10/0 nylon running suture over the limbal region. The area from 7 to 10 o' clock was left uncovered with no dissection at the limbus. Nine days postoperatively the membrane was noted to be securely in place (Fig 3B) and partially epithelialised (Fig 3C). Three months postoperatively the AM dissolved over the cornea (Fig 3D) resulting in a transparent and stable ocular surface with a BCVA of 20/60. Eight months postoperatively, however, the area that was left unoperated—that is, not covered by AM, showed progressive vascularisation and conjunctivalisation (Fig 3E). This region was characterised by an irregular epithelial surface which displayed delayed fluorescein uptake caused by poor epithelial integrity (Fig3F). At final follow up 21 months following surgery the operated area remained stable and non-inflamed and the patient was minimally symptomatic with a BCVA of 20/20.

Comparison of preoperative and postoperative appearances of case No 13 with LSCD arising from a chemical burn. Prominent fibrovascular pannus of 300° noted at presentation extending from 11 to 9 o' clock (A). Nine days following AMT and superficial keratectomy (B), the eye was non-inflamed and AM was held in place by a running 10/0 nylon suture. The AM was partially epithelialised with a residual central defect apparent on fluorescein staining (arrows) (C). Four months postoperatively, the cornea was transparent with an intact and smooth epithelial surface (D). However, 8 months postoperatively progressive vascularisation and conjunctivalisation (arrows) arose from the limbal area that was originally thought only to be mildly affected and not excised or covered with AM (E). Delayed fluorescein staining was noted in the area of corresponding epithelial irregularity (F).
Case 14
A 52 year old woman initially presented to the referring ophthalmologist with a 5 year history of photophobia, ocular irritation, and decreasing vision worse on the right eye. No previous history of atopy or significant systemic illness was obtained. Bilateral corneal peripheral fibrovascular pannus was observed with conjunctival foreshortening worse on the right, and a BCVA of 20/60 right eye and 20/40 left eye. Immunofluorescence studies of a conjunctival biopsy were inconsistent with ocular cicatricial pemphigoid and no eosinophils were observed in the specimen. Cataract surgery of the right eye was followed by deterioration of the condition and no improvement was obtained with topical steroids or topical and systemic antibiotics. Corneal topography revealed increasing astigmatism and at the time of referral she complained of severe photophobia, foreign body sensation, ocular irritation, and progressive loss of vision. Examination revealed a BCVA of 20/100 right eye and 20/60 left eye with fine pannus predominantly of the superior and inferior limbus affecting the right eye (Fig 4A) more than the left and associated with poor epithelial integrity (Fig 4B). Lipid tear deficiency was diagnosed on the basis of meibomium orifice metaplasia, short tear break up time (3 seconds), and facial rosacea. Floppy eyelid syndrome was also present but corneal, conjunctival, and lid margin sensitivity measured with the Bonnet-Cochet aesthesiometer was normal. The diagnosis of idiopathic, bilateral LSCD affecting almost 360° of the right limbal zone was made on the basis of the clinical examination and impression cytology findings. Excision of the fibrovascular pannus to the intact corneal epithelium followed by AMT of the right eye (Fig1). Despite topical treatment with preservative-free methylprednisolone (BPEI pharmacy), the procedure was followed by marked inflammation of the host conjunctiva and systemic immunosuppression with cyclosporin A was commenced. The membrane was re-epithelialised 30 days postoperatively and the cyclosporin A discontinued 2 months later. Two months following the procedure the patient reported that the right eye was comfortable and non-photophobic, examination revealed the eye to be non-inflamed with a clear, smooth, intact corneal epithelial surface (Fig 4C and D). The BCVA was improved at 20/30 right eye and unchanged on the left at 20/60 at final follow up 13 months following surgery. This contrasted with the left eye which had been maintained on medical treatment only and displayed no change in the corneal findings of vascularisation (Fig 4E) and poor epithelial integrity (Fig 4F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Preoperative and postoperative appearances of case 14 with idiopathic LSCD. At presentation, prominent fibrovascular pannus was noted (white stars) to involve nearly 360° of the limbus (A). This was associated with an irregular epithelium (white arrows) characterised by delayed fluorescein uptake (B). Two months following AMT the corneal surface showed no recurrence of the fibrovascular pannus (C) with a restored epithelial integrity demonstrated by fluorescein staining (D) although a prominent stromal vessel was still apparent at 12 o' clock. This appearance contrasted with the fellow eye (E), which acted as a control as no surgery was performed. In this eye the epithelial irregularity is still evidenced by delayed fluorescein uptake (F).
Discussion
In this report, we have shown that AMT ameliorated annoying photophobia or pain, facilitated rapid epithelialisation, restored a normal corneal epithelial surface, and improved the final visual acuity in the majority of these 17 consecutive eyes with partial LSCD. Photophobia and ocular discomfort were abolished in 85.7% and substantially reduced in the remaining 14.3% of the 14 patients who presented with these complaints. Epithelialisation of the entire membrane covered surface took an average of 22.8 days. Excluding the three eyes with limited visual potential due to radiation optic neuropathy, macular degeneration, or total retinal detachment, 92.9% of eyes gained visual acuity with 42.9% of eyes gaining one to three lines, 14.3% gaining four to five lines, and 35.7% gaining six or more lines. These findings substantiate our earlier report,32 and more importantly confirmed that this favourable outcome could be maintained in all of the above cases for more than 1 year of follow up (with a mean of 25.8 months). Collectively, these data support the hypothesis that AMT can help preserve and expand the remaining limbal epithelial stem cell population in vivo that is left in partial LSCD. This effect was noted even in eyes with more than 300° of LSCD. In two cases of nearly total LSCD (cases 14 and 15), we found AMT was still workable if a central island of epithelium remained intact. This observation suggested that surviving islands of transient amplifying cells were worth preserving and may have contributed to the regeneration of the corneal epithelium. In these two cases, the defect healed in 15 and 30 days, respectively, despite the nearly total loss of limbus. Taken together these observations have prompted us to propose the use of AMT as a first line procedure to treat patients suffering from partial LSCD. Because no transplantation of autologous or allogeneic limbal epithelial stem cells is needed, the potential complications of systemic immunosuppression and risk to the donor eye can be avoided. In one of our reported cases (case 14) we did employ systemic immunosuppression for a 2 month period. In this case the idiopathic inflammation at the junction between the conjunctiva and AM was noted to resolve fairly rapidly without the features of hypopyon uveitis recently reported following repeated AMT for deep trophic ulcer.37
The beneficial effect of AMT may be due in part to the restoration of an intact basement membrane that is invariably damaged in LSCD. Basement membrane is known to support epithelial cell adhesion, differentiation, and migration (see review by Tseng and Tsubota38), and to suppress epithelial cell apoptosis.39 Compositionally, the basement membrane component of the amniotic membrane resembles that of the conjunctiva.40 Amniotic membrane basement membrane is an ideal substrate for supporting the growth of epithelial progenitor cells by prolonging their life span and maintaining their clonogenicity.41 This action explains why AMT facilitates epithelialisation for persistent corneal epithelial defects with stromal ulceration.3542-45 In tissue culture, amniotic membrane supports epithelial cells grown from explant cultures444647 and other cultures,48 and maintains their normal morphology and differentiation. The resultant graft with an epithelial cell layer and amniotic membrane can be successfully transplanted back to reconstruct the damaged corneal surface in rabbits4748 and in humans.4849
The stromal side of the membrane may also provide additional benefit in treating LSCD. We have reported that this side contains a unique matrix component that suppresses TGF-β signalling, and the proliferation and myofibroblast differentiation of normal human corneal and limbal fibroblasts50 and normal conjunctival and pterygium body fibroblasts.51 This action explains why AMT reduces fibrosis during conjunctival surface reconstruction,3652 prevents recurrent scarring after pterygium removal,53-55 and reduces corneal haze following phototherapeutic keratectomy and photorefractive keratectomy.55-58 The stromal matrix of the membrane can also exclude inflammatory cells,5859 and contains growth factors60 and several forms of protease inhibitors.61 These actions explain why stromal inflammation is reduced after AMT3536 and corneal neovascularisation is mitigated.62 Collectively, these actions are useful to prepare a stromal bed that may subsequently support limbal epithelial stem cells (for review see Tseng3). In this manner, AMT has been used either simultaneously or following the transplantation of allogeneic limbal epithelial stem cells to treat patients with total LSCD.31325463-66 Taken together, these findings and the results of the present study suggest that AMT may be superior to repeated debridement of the conjunctivalised corneal surface which has been reported to be effective in six cases of partial LSCD with a follow up less than 8 months6768 although a randomised clinical trial would be required to answer this question.
In summary, this report demonstrates that AMT is a safe and effective procedure to restore the corneal epithelial surface in patients with partial LSCD. By avoiding the potential complications of autograft or allograft transplantation of limbal tissue, AMT may offer a superior alternative. Future studies directed to the molecular mechanism by which AM may help preserve and expand limbal epithelial stem cells may clarify our understanding of this unique biological matrix and unravel other potential clinical applications.
Acknowledgments
Supported in part by an unrestricted grant from Research to Prevent Blindness, Inc, New York, USA and in part by a research fellowship grant (to DFA) from the TFC Frost Charitable Trust, UK.
Proprietary interest: SCGT has filed a patent on preparation and clinical uses of amniotic membrane.