Article Text

Abstract
BACKGROUND The factors that influence pulsatile ocular blood flow (POBF) were evaluated in normal subjects.
METHODS POBF was measured in 80 normal subjects using Langham OBF computerised tonometry. The effect of age, systolic and diastolic blood pressure, refractive error, intraocular pressure, and axial length on POBF was evaluated using multiple regression analysis.
RESULTS The mean (SD) POBF value was 593.3 (203.6) μl/min (range 290.7–1201.6). Of all the independent variables in the model, only the axial length was statistically significant (p=0.008). The regression coefficient was negative, indicating that the axial length decreased with increasing POBF.
CONCLUSIONS These data suggest that, in normal subjects, the POBF decreases as axial length increases. Choroidal blood flow may decrease as the axial length increases. The axial length may therefore be a major factor affecting POBF.
- pulsatile ocular blood flow
- axial length
- choroidal blood flow
Statistics from Altmetric.com
The determination of pulsatile ocular blood flow (POBF) by measuring intraocular pressure (IOP) pulse using Langham OBF computerised tonometry is a reliable way of evaluating choroidal blood flow.1-3 POBF has been evaluated in several ocular diseases including glaucoma,4 diabetic retinopathy,5 retinal pigmentosa,6 and age related macular degeneration.7 Several authors have reported that factors such as age, heart rate, blood pressure (BP), and axial length influence POBF.8-11
In this study we evaluated the factors that influence POBF in normal subjects. We determined the relation between POBF and age, systolic and diastolic BP, IOP, refractive error, and axial length using multiple regression analysis.
Materials and methods
Eighty Japanese subjects (27 men, 53 women) were enrolled in the study. The characteristics of the subjects are summarised in Table 1. Subjects with diabetes, heart disease, systemic hypertension, glaucoma, other ocular diseases, and a history of ophthalmic surgery were excluded from the study. Only one eye of each subject was randomly included. The study protocol was reviewed by the ethics committee of our institution and informed consent was obtained from all subjects. All procedures adhered to the tenets of the Declaration of Helsinki.
Characteristics of the subjects
POBF was measured by Langham OBF computerised tonometry (Langham Ophthalmic Technologies, Timonium, MD, USA) with the subjects in the sitting position. Data were collected from each subject and the mean measurements were calculated from five representative pulses. Systolic and diastolic brachial arterial BP were measured with a sphygmomanometer with subjects in the sitting position, IOP was measured with a non-contact tonometer (CT-90, Topcon, Japan), and axial length was measured using A-scan biometric ultrasound (OcuScan, Alcon, Fort Worth, TX, USA). The refractive error was expressed as a spherical equivalent refraction obtained by autokeratorefractometry (KR-7100, Topcon).
Multiple regression analysis was performed to determine the correlation between POBF and age, systolic and diastolic BP, IOP, refractive error, and axial length. The results are expressed as mean (SD).
Results
The range of POBF values is shown in Figure 1. The mean (SD) value of POBF was 593.3 (203.6) μl/min (range 290.7–1201.6).

Distribution of pulsatile ocular blood flow in the study population (n=80).
Table 2 shows the results of multiple regression analysis with POBF as the dependent variable. Of all the independent variables in the model, only the axial length was statistically significant (p=0.008). The regression coefficient was negative, indicating that the axial length decreased with increasing POBF.
Results of multiple regression analysis
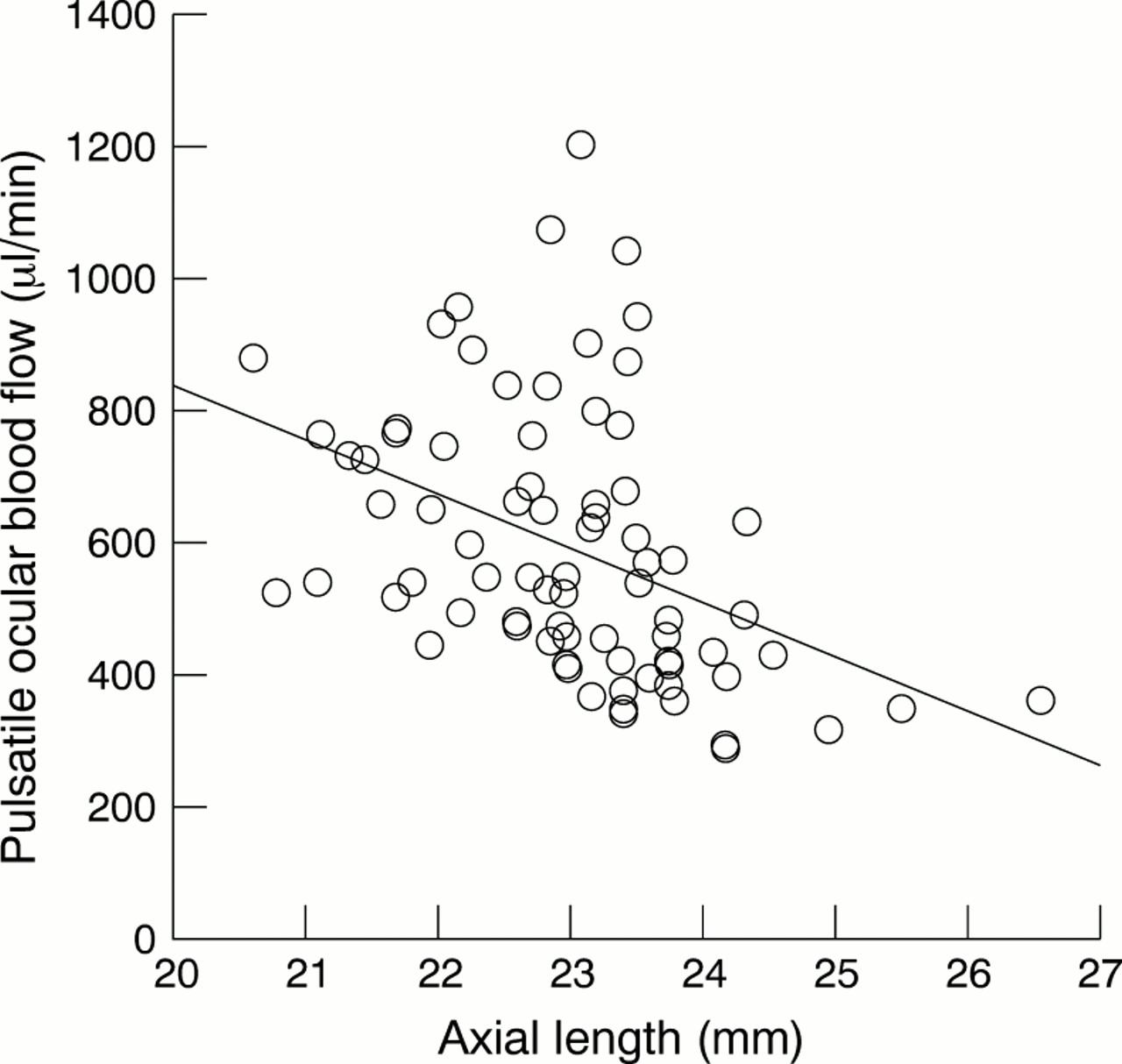
Stepwise elimination of non-significant variables led to an optimum model that included only axial length (coefficient = –0.42; p=0.0002), indicating that it was the only variable contributing to the POBF. Figure 2 shows the relation between POBF and axial length.

{kind=link}
{kind=link}
Relation between pulsatile ocular blood flow and axial length.
Discussion
In this study the mean POBF value was 593.3 μl/min (range 290.7–1201.6). Several authors have reported mean POBF values between 444 and 803 μl/min in normal subjects.13-11 The values were consistent with those of the Japanese subjects in the present study.
The results of this study show that, as axial length increased, POBF decreased in normal subjects. In experimental chick models the choroidal blood flow decreased in myopic eyes with ocular enlargement induced by wearing goggles or corneal incisions.12-15 A reduction in ocular blood flow has been reported in severe myopia with increasing axial length.1617 The choroidal blood flow may decrease as the axial length increases.
The axial length was the major factor affecting POBF in the normal subjects in this study. Several authors have reported a relation between the ocular axial length and the ocular pulse amplitude and POBF.8111819 They have suggested a number of possible reasons, other than decreasing choroidal blood flow, for the relation between axial length and the ocular pulse amplitude and POBF. Firstly, the ocular volume increases with increasing axial length so the effect of a small increase in volume caused by each bolus of blood may be reduced. Secondly, the negative correlation between scleral rigidity and ocular volume and axial length may affect the POBF. Honmura et al reported a significant correlation between scleral rigidity and axial length.20We believe that we need to consider the relation between POBF, axial length, and scleral rigidity in the future.
Ravalico et al found that ocular pulse amplitude and POBF decreased in normal subjects with increasing age.10 However, these authors performed multiple regression analysis without considering refractive error or axial length. In our study we have determined the relation between POBF and age, BP, IOP, refractive error, and axial length using multiple regression analysis and found no significant regression between POBF and age.
The results of our study suggest that, as axial length increases, POBF decreases in normal subjects. The choroidal blood flow may decrease as the axial length increases. We conclude that axial length is the major contributory factor to POBF in normal subjects.