Article Text

Abstract
AIM To define the clinical and microbiological profile of bacterial keratitis at the Jules Gonin Eye Hospital and to test the in vitro bacterial resistance.
METHODS Patients presenting with bacterial keratitis were prospectively followed; clinical features (age, risk factors, visual acuity) and response to therapy were analysed. Bacteriological profile was determined and the sensitivity/resistance of isolated strains were tested towards 12 ocular antibiotics (NCCLS disc diffusion test).
RESULTS 85 consecutive patients (mean age 44.3 (SD 20.7) years) were prospectively enrolled from 1 March 1997 to 30 November 1998. The following risk factors were identified: contact lens wear, 36%; blepharitis, 21%; trauma, 20%; xerophthalmia, 15%; keratopathies, 8%; and eyelid abnormalities, 6%. The most commonly isolated bacteria wereStaphylococcus epidermidis, 40%;Staphylococcus aureus, 22%;Streptococcus pneumoniae, 8%; othersStreptococcus species, 5%;Pseudomonas, 9%;Moraxella andSerratia marcescens, 5% each;Bacillus,Corynebacterium, Alcaligenes xyloxidans, Morganella morganii, andHaemophilus influenza, 1% each. 1–15% of strains were resistant to fluoroquinolones, 13–22% to aminoglycosides, 37% to cefazolin, 18% to chloramphenicol, 54% to polymyxin B, 51% to fusidic acid, and 45% to bacitracin. Five of the 85 patients (5.8%) had a poor clinical outcome with a visual loss of one or more lines of visual acuity.
CONCLUSION Fluoroquinolones appear to be the therapy of choice for bacterial keratitis, but, based upon these in vitro studies, some strains may be resistant.
- bacterial keratitis
- microbiology
- antibiotics
- fluoroquinolones
Statistics from Altmetric.com
Bacterial keratitis, because of its high incidence and potential complications, is one of the most visually threatening ocular infectious pathologies. The avascular corneal stroma is particularly susceptible to bacterial infection, and many patients have a poor clinical outcome if aggressive and appropriate therapy is not promptly initiated. Corneal perforations, which can occur in less than 24 hours, have been reported in the presence of particularly invasive pathogens such as Pseudomonas aeruginosa andStaphylococcus aureus.1Furthermore, clinical outcome can be influenced by onset of a corneal opacity within the visual axis, which can cause a decrease in visual acuity that can be reversed only by a corneal graft transplantation. In addition, emergence of multiresistant strains is a major concern when antibiotics such as fluoroquinolones are used as monotherapeutic agents.
The conjunctiva and ocular adnexae are rapidly colonised by bacteria at birth,2 and conjunctival bacterial microflora undergo constant turnover. The flora isolated in healthy individuals consist primarily of Staphylococcus epidermidis and diphtheroids. Species of greater virulence, such asStaphylococcus aureus,Streptococcus pneumoniae,Pseudomonas aeruginosa, and evenNeisseria meningitidis, have been reported.3
Corneal infections result mostly from a failure of one of the protective mechanisms that maintain the ocular surface integrity; most ocular pathogens cannot penetrate an intact epithelial corneal layer that is protected by the eyelids and the tear film. Passive and active host defence mechanisms protect corneal tissues from bacterial invasion. Complement activation and enzyme secretion within the lacrimal fluid are part of the natural host defence mechanisms, and although lysozymes, lactoferrin, betalysin, orosomucoid, and ceruloplasmin have been isolated within the lacrimal fluid,2 the specific role of each of these enzymes has yet to be determined. Once the passive mechanisms of corneal protection have failed or the corneal epithelium is breached, bacteria are free to invade the cornea. Polymorphonuclear cell attraction is induced primarily by interleukin 8 (IL-8) and occurs 8–10 hours after the corneal damage. This IL-8 secretion may also be responsible for further development of neovascularisation.45 Corneal infiltration by inflammatory cells appears, by slit lamp examination, as corneal cloudiness that surrounds the infected tissues. The specific immunity arises from the limbus, which is surrounded by numerous lymphoid T and B cells that are part of the mucosal associated lymphoid tissues (MALT).6 Secreted immunoglobulins also enhance bacterial phagocytosis.
Recurrent attacks of bacterial keratitis are particularly frequent in the presence of constitutional factors such as dry eye syndrome or eyelid abnormalities.
Gram negative bacteria are known to be associated with soft contact lens wear, and disposable contact lens wear has been linked to an increased incidence (15–20-fold) of ulcerative keratitis.7
Finally, the bacterial pattern of keratitis can also be influenced by geographic and climatic factors; many differences in keratitis profile have been noted between populations living in rural or in city areas. This may be explained by the high variation of habits between these two groups, such as antibiotic use, contact lens wear, or even specific rural pathogen exposure.
Adequate ocular prevention, knowledge of the microbiological pattern in a given clinical practice, and a prompt choice of appropriate fortified antibiotics constitute the management of bacterial keratitis. Identification of the pathogen, initiation of immediate therapy, modification based on the organism identified, and consideration of drug toxicity and bacterial resistances represent the keys to success in the management of bacterial keratitis.89
Aim
The objectives of this prospective study were to define the clinical risk factors, the prognosis, and the microbiological pattern of bacterial keratitis at the Jules Gonin Eye Hospital, and then to test these bacteria against the most commonly used ocular antibiotics in order to formulate new guidelines for therapy.
Material and methods
PATIENTS
From 1 March 1997 to 30 November 1998, all patients presenting with a corneal infiltrate compatible with a diagnosis of bacterial keratitis were enrolled in a prospective study.
To avoid the inclusion of chronic ulcerations, patients with a corneal ulceration lasting for 3 weeks or more were excluded. Patients suspected of having or with a positive culture for fungal, viral, orAcanthamoeba infection were also excluded.
The following standard protocol for bacteria isolation was used: a corneal smear was taken after topical anaesthesia was obtained by application of a drop of single dose unit oxybuprocaine 0.4% (Faure, Ciba Vision Ophthalmics, Novartis, Switzerland). The swabs were performed with surgical triangular spears from Merocels (Solanm Division of Xomed Surgical products, Jacksonville, FL, USA). Inoculation of agar culture plates (chocolate, blood and Sabouraud media) was performed according to the National Committee for Clinical Laboratory Standards protocol (NCCLS, Villanova PA, USA).10 An additional swab was performed and the spongy tip of the triangular spear was directly cut into a bottle of sterile brain heart infusion culture medium (BHI). Media were incubated at 37°C in a 2% carbon dioxide atmosphere.
Isolated bacteria were tested for their resistance against the following 12 ocular antibiotics: bacitracin, cefazolin, chloramphenicol, gentamicin, neomycin, polymyxin B, lomefloxacin, ciprofloxacin, norfloxacin, ofloxacin, tobramycin, and fusidic acid. The resistance to antibiotics was evaluated with the standard disc diffusion method, according to the modified test recommended by the NCCLS. The discs of antibiotic for resistance testing were obtained from Difco Laboratories (Dispens-O-disc susceptibility test system, Difco Laboratories, Detroit, MI, USA). Since no criteria for resistance of corneal infections are available, the cut-off values for systemic bacterial infections applied for septicaemia were used according to the NCCLS recommendations.1112
TREATMENT PROTOCOL
The standard treatment consisted of topical cefazolin 50 mg/ml (Kefzol, Lilly Pharmaceuticals, Vernier, Switzerland) and fortified gentamicin 9 mg/ml (Garamycin, Essex Pharmaceuticals, Luzern, Switzerland) given alternately every 15 minutes during the first 2 hours, then every hour for the following 24 hours. Later, antibiotics were progressively tapered according to the clinical response. Bottles of antibiotics were freshly prepared and cefazolin was changed every 4–5 days as it contains no preservative. This standard protocol was used for all patients unless they had a corneal infiltrate that was less than 1 mm in diameter or another suitable therapy had already been initiated.
PARAMETERS STUDIED
History and examination were focused on the following risk factors: corneal injuries (organic or mineral foreign bodies), contact lens wear, blepharitis, keratopathies (due to previous herpetic infection, corneal dystrophy or surgical procedure, as in bullous keratopathy), dry eye syndrome, corneal surgery (graft transplantation, excimer treatment), or eyelid abnormalities (entropion, ectropion, lagophthalmos, and others). Visual acuities were measured with Snellen charts.
Extension of keratitis was measured with the Haag-Streit 900 slit lamp. The major site of keratitis was determined according to five zones that were previously defined: central or pupillary area, nasal, inferior, temporal, and superior. The ulceration depth was evaluated as < 30%, 30–60%, or >60% of the total corneal depth. Anterior chamber inflammation, when present, was scored, according to Hogan and associates, a 0+ to 4+ for Tyndall effect and cells.13 To define the clinical outcome, patients were considered to have a poor outcome if they had visual loss of acuity of one or more Snellen lines or if a major complication occurred, such as corneal perforation, or if corneal transplantation was indicated.
Results
PATIENT DATA
During 21 consecutive months (from 1 March 1997 to 30 November 1998), 85 patients were seen at the Jules Gonin Eye Hospital with a corneal infiltrate that was compatible with a diagnosis of bacterial keratitis. Twenty (23.5%) patients were admitted to the hospital for therapy, while the other 65 (76.5%) were treated in the outpatient clinic. The mean age of the patients was of 44.3 (SD 20.7) years (range 7–91 years); sex distribution was 1:1 (43 men and 42 women).
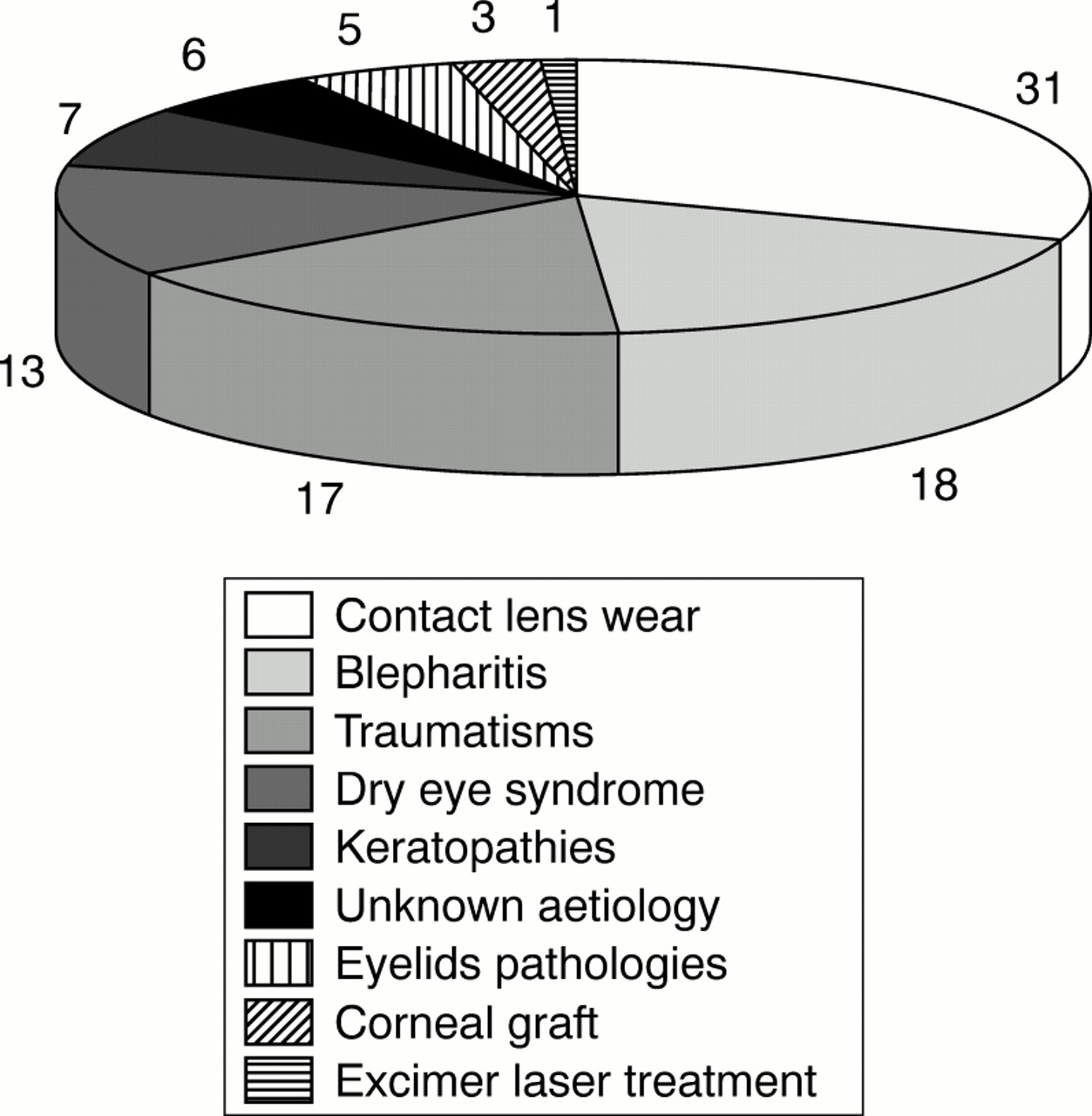
Contact lens wear was by far the most common risk factor; this was encountered in 31 (36%) patients. Severe blepharitis was present in 18 (21%) of the patients. In 17 patients (20%), the keratitis was induced by foreign bodies—10 patients with organic material (vegetable or animal) and seven patients with mineral particles. Dry eye syndrome was diagnosed in 13 (15%) patients. Keratopathies (including herpetic, bullous, and postoperative keratopathies) were present in seven (8%) patients. Other aetiologies are summarised in Figure 1. Fifteen (18%) patients had more than one risk factor: dry eye disease was present in one patient with an eyelid pathology, in two patients with previous corneal trauma, and in three patients who wore contact lenses. Blepharitis was present in four patients having eyelid pathologies, in three patients with previous corneal trauma, in one with contact lens wear, and in one with a corneal graft. No significant difference in risk factors was noted between patients living in rural or urban areas, but organic foreign bodies tended to be more common in patients from rural areas, and all three patients presenting with a corneal infection after keratoplasty were from a rural area.

Contact lens wear is by far the most common risk factor encountered. The numbers refer to the numbers of patients. Blepharitis and trauma are also major risk factors for the development of keratitis. Other aetiologies, such as dry eye syndrome, keratopathies, and eyelid pathologies, are less common risk factors.
The corneal localisation of the ulcers was randomly distributed—32% were central, 28% nasal, 48% inferior, 33% temporal, and 28% superior (total percentage is greater than 100 because more than one area was affected in many patients). Lesions of the inferior zones were associated primarily with contact lens wear or trauma. Interestingly, lesions of the temporal and superior zones were never associated with eyelid pathologies.
The diameter of the corneal ulceration was of 1 mm or less in 44 patients (51.7%), 1–2 mm in 21 patients (24.8%), and over 2 mm in 20 patients (23.5%).
Ulceration depth was less than 30% in 49 patients (57.6%), between 30% and 60% in 31 patients (36.5%), and over 60% in five patients (5.9%).
Anterior chamber inflammation was absent in 56 patients (65.9%). A 1+ to 2+ Tyndall effect with 1+ to 2+ cells was present in 21 patients (24.7%), and severe anterior chamber inflammation (3+ to 4+ Tyndall effect and cells, with or without hypopyon) was present in eight patients (9.4%).
MICROBIOLOGICAL CONSIDERATIONS
In 73 (86%) patients, bacteria were isolated from the corneal smears. In five of the 12 patients with negative cultures, treatment with ocular antibiotics had been initiated before they were referred. Three patients were treated by chloramphenicol drops for, respectively, 12, 6, and 1 day before inclusion; one patient was taking neomycin for 6 days and one gentamicin for 1 day. The remaining seven of the 12 negative cultures (58%) came from patients who were not taking any treatment before the corneal smears were obtained.
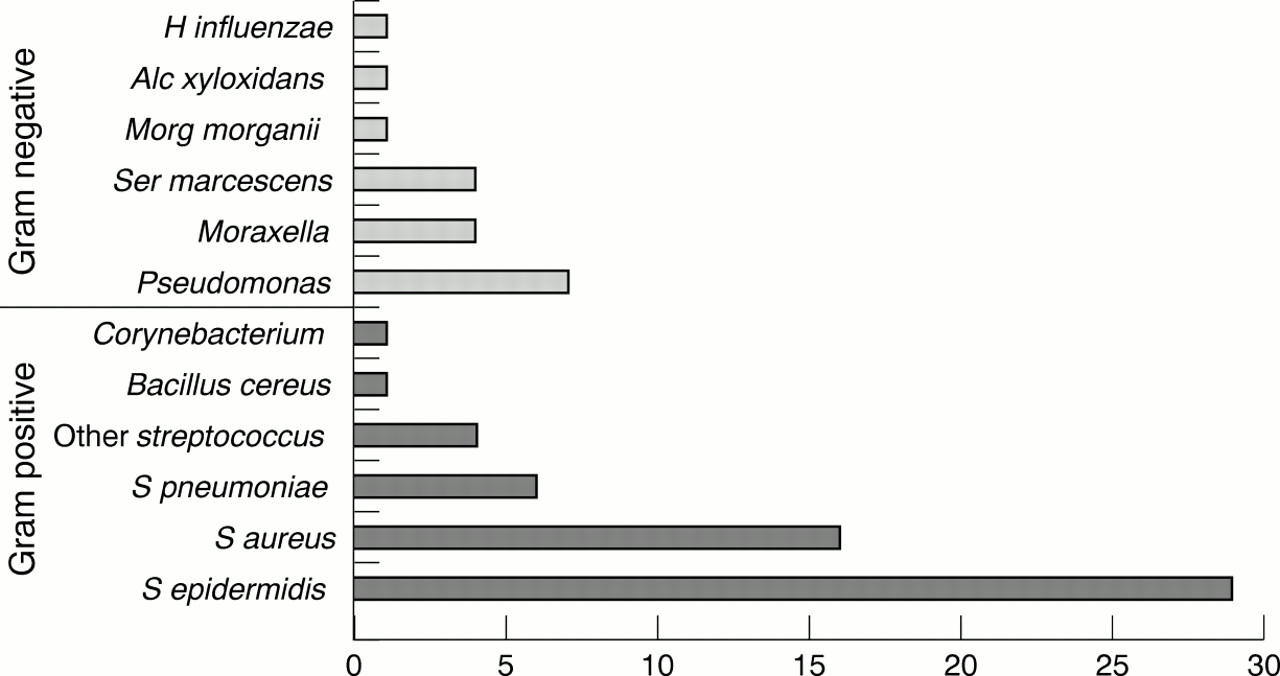
BHI media was more sensitive than agar plates for bacterial isolation since 66 (90%) of the 73 positive cultures were in BHI medium, whereas only 39 (53%) were positive in agar plates. In 34/73 (46%) patients, culture was positive in BHI medium only, whereas 7/73 (9%) were positive exclusively in agar plates. In 32/73 (44%), both culture media were positive. The incubation period was similar in 20 cases (30.7 (SD 13.8) hours), shorter in agar plates in seven cases and shorter in BHI in five cases. However, when incubation time was shorter in agar plates, the difference was always less than 24 hours. Bacteria were isolated in less than 3 days (72 hours) in all positive cases. In more than 90% of cases, bacteria were isolated in less than 48 hours. In only two patients were two pathogenic bacteria isolated in the same culture (total number of bacteria, 75 for 73 patients). The bacterial pattern is shown in Figure 2. Gram positive bacteria were predominant, mainly Staphylococcus species; Gram negative bacteria were mostly Pseudomonas species.

Gram positive bacteria are by far the most commonly isolated organisms of which Staphylococcus species predominate. Pseudomonas aeruginosa is the Gram negative bacterium most encountered.
In almost all risk groups (except contact lens wearers and patients who had undergone a corneal graft transplantation), primarily Gram positive bacteria were isolated (75%), mostlyStaphylococcus species. In patients wearing contact lenses, 12/28 (43%) were Gram negative, mostly Pseudomonas species. Two of three patients presenting with a keratitis after keratoplasty were infected by Gram negative bacteria (one Moraxella and one Morganella); the third patient was infected by Staphylococcus aureus.
SENSITIVITY AND RESISTANCE TO ANTIBIOTICS
All (save for eight) isolated bacteria were tested on 12 antibiotics that are currently used in ophthalmology; the eight strains could not be tested because of improper technical management. The results of bacterial in vitro tests are represented in Figure 3.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chloramphenicol, cefazolin, and new fluoroquinolones (particularly ofloxacin) are very effective against Gram positive bacteria. In contrast, many of these same bacteria are resistant to polymyxin B (A). Similar to the effectiveness against Gram positive bacteria, the new fluoroquinolones are also effective against Gram negative bacteria. Aminoglycosides (tobramycin, neomycin, and gentamicin) also provide a broad spectrum of activity against Gram negative pathogens. Bacitracin, cefazolin, chloramphenicol, and fusidic acid, on the contrary, have little effect against these bacteria (B).
Testing showed that more than 40% of strains (Gram positive and Gram negative) are resistant to polymyxin B and fusidic acid. Only 18% of bacteria are resistant to chloramphenicol; in fact, the sensitivity rate is 98% for Gram positive bacteria although 65% of Gram negative strains are either resistant or show only intermediate sensitivity.
The new class of fluoroquinolones showed a good effect against both Gram positive and Gram negative bacteria, except for several strains ofStreptococcus pneumoniae and a multiresistant Pseudomonas. A few bacteria were highly resistant to almost all of the antibiotics available for use in ophthalmology: 3/75 strains (4%) were considered highly resistant as they were resistant to seven or more of the tested antibiotics.
Seventy of the 85 patients (82%) were treated according to the standard protocol as defined previously. The remaining 15 patients, who did not benefit from the cefazolin-gentamicin regimen, received the following—13 patients were on monotherapy (six with ofloxacin, five with lomefloxacin, two with chloramphenicol), two were on a different combined therapy (one ofloxacin-cefazolin and one ofloxacin-chloramphenicol).
CLINICAL OUTCOME
Among the 70 patients who were treated with the combination of cefazolin 50 mg/ml and fortified gentamicin 9 mg/ml, only three patients (4%) had a poor clinical outcome:
-
An 85 year old woman with severe entropion, chronic secondary corneal oedema and neovascularisation had a 2 × 2 mm corneal ulceration in the superotemporal area. The culture was positive for Morganella. Corneal ulceration depth was 90% of the total corneal thickness. She developed a corneal perforation 2 weeks after presentation despite application of fortified antibiotics according to our standard protocol.
-
An 80 year old man with chronic bullous keratopathy after anterior chamber intraocular lens implantation developed a central corneal abscess, due to Streptococcus pneumoniae, that reached 4 × 2 mm and involved 60% of the corneal depth. Two months after the abscess healed he developed a central corneal scar and visual acuity was limited to hand movement.
-
A 70 year old man with progressive rheumatoid arthritis developed a nasal corneal ulceration measuring 1.5 × 1 mm involving 60% of the corneal depth. This was due to Pseudomonas aeruginosa. He developed a corneal perforation after 3 days of in-hospital therapy and required a corneal graft transplantation.
Of the 15 patients (13%), who did not benefit from the standard therapy, two (13%) had a poor clinical outcome:
-
A 77 year old man with severe blepharitis, ocular rosacea and ectropion developed a 4 × 5 mm ulceration in the inferior half of his right cornea; this ulceration, due to Streptococcus oralis, involved 60% of total corneal depth. Combined therapy with cefazolin and ofloxacin was introduced. The abscess healed but he subsequently developed major thinning of the cornea and a Gundersen's procedure was performed.
-
The second patient was a 40 year old man with severe dry eye syndrome. He received monotherapy of chloramphenicol for a small corneal abscess of 1 × 1 mm, with corneal ulceration depth of less than 30% (near the limbus) after excision of a pterygium. Staphylococcus epidermidis was isolated. The keratitis quickly resolved but he developed severe irregular astigmatism 2 months later and his visual acuity decreased from 10/10 to 7/10.
Discussion
Bacterial keratitis is rare in the absence of a predisposing factor. Until recently, most cases of microbial keratitis were associated with ocular trauma or ocular surface disease, but the widespread use of soft contact lenses has greatly increased the risk of bacterial keratitis,14 which is estimated to be 10–15 times higher with the use of extended wear disposable contact lenses.71516 In our series of 85 cases of bacterial keratitis, 31 (36%) were associated with contact lens wear (Fig 1). Ocular trauma remains the second most common cause of bacterial keratitis, accounting for 17 (20%) of our cases. Trauma is a far more common predisposing factor for bacterial keratitis in low income countries, where it accounts for up to 77.5% of cases.17The presence of organic materials within the wound represents a much higher risk than does the presence of non-organic substances.
Ocular surface diseases such as dry eye syndrome, chronic blepharitis, and eyelid pathologies also predispose to bacterial keratitis. Older individuals are more commonly affected, particularly those with rheumatoid diseases, who may have difficulty with drop administration, leading to recurrent attacks of bacterial keratitis. Older age, delay in referral, topical steroid treatment, past ocular surgery, poor vision at presentation, large size of ulcer, and central location of the ulcer are all major risk factors that can necessitate penetrating keratoplasty,18 or even evisceration or enucleation in patients with bacterial keratitis.19 The specific bacteria isolated is also implicated in loss of the eye, asPseudomonas strains were more often isolated in eyes that had to be removed because of ulcerative keratitis.19
Various methods have been described for bacterial isolation. When only blood agar and chocolate agar plates were used, the isolation rate was estimated to be 67%, and in 70% of these cases, blood and chocolate agar plates yielded similar results.20 The overall success rate of bacterial isolation was high in the present study, with 86% of smears being positive. The isolation rate of bacteria using blood and chocolate agar plates or BHI media was 45.9% and 77.6% respectively. The higher isolation rate in BHI can probably be explained by the fact that the spongy tip of the Merocels spears was directly cut into the BHI media, whereas agar plates were inoculated by rolling the spear tip across the surface, as described in CUMITECH 13A.10 Our technique yields an isolation rate similar to that of corneal biopsy and tissue microhomogenisation, in which the isolation rate was of 88%.21
Our current treatment of bacterial keratitis consists of topical instillation of fortified antibiotics (cefazolin and gentamicin), which has been the “gold standard” for the therapy of bacterial keratitis.22 However, a rapid decrease in the concentration of gentamicin on the ocular surface does occur. The longest elapsed time after instillation for detection of gentamicin on the conjunctiva was 40 minutes for ointment and only 10 minutes for drops. At 10 minutes, the ocular surface concentration was 310 mg/ml for ointment and 45 mg/ml for drops.23 Furthermore, gentamicin has poor corneal penetration; the anterior chamber concentration of gentamicin was below limits of detection (<0.6 mg/l) at the time of surgery, after the administration of five drops or ointment 30–60 minutes before cataract surgery.23
The use of fortified antibiotics has also been associated with local toxicity to the corneal epithelium.24 Patients often complain of ocular irritation or intense conjunctival reactions during drop instillation. The use of antibiotics without preservatives, such as cefazolin, can be associated with bottle contamination by bacteria. This study was conducted to determine the percentage of clinical cases of bacterial keratitis that are resistant to fluoroquinolone monotherapy.
Since 1991, fluoroquinolones have been available for the treatment of bacterial conjunctivitis. These relatively new agents are bactericidal, exert their effect by DNA gyrase inhibition, and have a broad spectrum of activity against both Gram negative and Gram positive bacteria. Many experimental and clinical studies have shown the efficacy of ciprofloxacin ointment or solution in the treatment of bacterial keratitis.1025-28 Fluoroquinolones have been shown to be effective in the treatment of methicillin resistantStaphylococcus aureus29 andPseudomonas aeruginosa,25 but the increasing number of bacterial strains resistant to fluoroquinolones is a major concern when they are used as monotherapeutic agents.
A recent report30 has shown a rapid increase inStaphylococcus aureus resistance to ciprofloxacin, with a 5.8% resistance in 1993, 9.4% in 1994, 11.4% in 1995, 26.5% in 1996, and 35% resistance in 1997; a similar rate of resistance progression was observed with ofloxacin. The resistance of other bacteria, such as Streptococcus pneumoniae, remained stable. In our study, multiresistant Gram negative strains were detected, and the rate of resistance was higher in bacterial keratitis than in conjunctivitis. The bacteria causing keratitis are possibly more virulent strains that may have been resistant to previously used systemic antibiotics.
Recent reports of bacterial resistance to fluoroquinolones suggest that bacteria isolated from bacterial keratitis must be periodically tested against available antibiotics in order to know the current resistance pattern. The disc susceptibility method provides quantitative measurements that are critical for epidemiology and drug resistance surveillance. Although this approach is both fast and cost effective,31 resistance criteria apply only to systemically achieved drugs levels, which are different from those achieved with topical treatments.
Two criteria must be considered when choosing a therapeutic agent in bacterial keratitis: the resistance rate and the penetration of the antibiotic at the level of infection. Among all fluoroquinolones, lomefloxacin has the best penetration of corneal tissues. Corneal tissue levels measured after topical administration of one drop was between 29 and 55 μg/g for lomefloxacin,32 5.28 (3.4) μg/g (range 1.43–10.58 μg/g) for norfloxacin,33and 8.82 (8.24) μg/g for ciprofloxacin.34 The aqueous humour concentration after topical administration was 0.072 μg/ml for ciprofloxacin, 0.057 μg/ml for norfloxacin, 0.338 μg/ml for ofloxacin, and 2.2–7.6 μg/ml for lomefloxacin.3335
Visual prognosis after bacterial keratitis depends on the size, locality, and depth of the ulcer, as well as on the risk factors and the bacteria isolated.18 In this study, five patients had a poor clinical outcome. The presence of chronic diseases such as dry eye syndrome, acquired eyelid deformities, bullous keratopathy, and rheumatoid diseases seems to play an important part in the development of such poor visual outcomes and to predispose to recurrence. Of the five patients in this report who had a poor visual outcome, three had ulcers of 2 × 2 mm, and the central cornea was affected in two. The depth of the ulcerations was 60% or more of total corneal depth in all but one case. This last patient had undergone a surgical procedure 4 weeks before the onset of keratitis (pterygium excision) that led to thinning of the cornea. Depth of the ulceration seemed then to have a more significant role in visual prognosis than did extent and location of the ulcer.
Bacteria isolated from our patients were Morganella morganii, Streptococcus pneumoniae, Pseudomonas aeruginosa, Streptococcus oralis, andStaphylococcus epidermidis, but the numbers are too small to allow for conclusions concerning the prognosis related to specific bacterial patterns.
In conclusion, bacterial keratitis remains a therapeutic challenge and a vision threatening ocular condition. Contact lens wearers in particular should be informed of the potential risk, and should be carefully instructed on how to care for their lenses. Extended wear contact lenses represent an even more important risk factor for development of bacterial keratitis. Patients suffering from chronic ocular conditions such as dry eye syndrome, eyelid pathologies, severe blepharitis, and bullous keratopathy and those with chronic rheumatoid diseases, should be monitored closely and forewarned about the development of corneal ulcerations.
Rapid isolation of bacteria and treatment with intensive ocular antibiotics represent decisive steps in the management of such pathologies. New classes of fluoroquinolones, such as lomefloxacin, provide a broad spectrum of antibacterial activity, better tolerance, and good tissue penetration, compared with what is currently the gold standard of therapy, which consists of a combination of cefazolin and gentamicin. However, bacterial resistance (in particular withStreptococcus pneumoniae) must be taken into account with any monotherapy. A double blind study comparing the benefits of both types of treatment could help in the future management of bacterial keratitis.
Acknowledgments
This work was supported by Ciba Vision Ophtalmics AG, Grenstrasse 10, 8180 Bülach, Switzerland.