Article Text

Abstract
Background/aims: Few studies have reported on the change in visual acuity (VA) in patients with choroideraemia. In order to determine the degree and rate of VA impairment associated with this disease, the central VA was analysed in a large group of patients with choroideraemia.
Methods: The authors completed a retrospective, cross sectional review of 115 patients with choroideraemia from three tertiary care centres. A longitudinal analysis was performed on 45 of these patients who met the inclusion criteria of at least three visits over a minimum period of 4.5 years. Multiple linear regression analysis was used to explore the 5 year rate of VA change while controlling for initial VA and initial age. Multiple logistic regression was also used to investigate VA impairment.
Results: In the cross sectional group (n = 115), 84% (87/103) of patients under the age of 60 had a VA of 20/40 or better while 33% (4/12) of patients 60 years of age or older had a VA of 20/200 or worse at their most recent visit. The majority of the patients (93%) in the longitudinal subgroup of 45 patients had a VA of 20/30 or better at their initial visit. The mean 5 year rate of VA change was 0.09 logMAR equivalent (approximately one line on the Lighthouse chart).
Conclusion: In this cohort of patients with choroideraemia, there was typically a slow rate of VA loss and the prognosis for central VA retention was, as a group, favourable until the seventh decade.
- choroideraemia
- retinal degeneration
- visual acuity
Statistics from Altmetric.com
Choroideraemia is an X linked, recessively inherited, progressive, diffuse degeneration of the choroid, retinal pigment epithelium (RPE), and retinal photoreceptor cells.1,2 Patients with choroideraemia characteristically experience nyctalopia in the first decade of life followed by visual field restriction with progression from annular scotomas to concentric field loss. Impairment in visual acuity (VA) is eventually noticed. Initial fundus findings in choroideraemia include pigmentary stippling and focal areas of choroid atrophy in the equatorial fundus that eventually encompass the more peripheral retina and posterior pole.1 In the final stage, there are extensive degenerative changes of the RPE with only remnants of the choroidal vasculature apparent in the macula, far peripheral retina, and near the optic disc. Eventually, the choroidal vessels within the macula may also atrophy, especially after the age of 40.1 In the advanced stages, the sclera becomes visible on fundus examination in the areas of total choroidal and RPE atrophy.
Although there have been a number of case reports, to our knowledge limited studies have been published concerning VA impairment in a large cohort of choroideraemia patients. Krill1 correlated VA in 11 choroideraemia patients with his suggested stages of retinal and choroidal degeneration. He reported no loss of central VA in “stage I,” mild to moderate loss of VA in “stage II,” and severe loss of VA to be more common after 40 years of age when atrophy of the major choroidal vessels occurs (“stage III”). Krill commented that VA could remain “reasonably good” until the sixth decade of life or later if the macular choroidal vasculature had not atrophied. Consistent with Krill's observations, Cheng et al,3 in their study of eight Chinese subjects with choroideraemia, reported that central VA was generally preserved in earlier stages and was markedly impaired in advanced stages. Following the study of a large family with choroideraemia, McCulloch and McCulloch4 reported that VA retention was related to the degree of remaining visual field. They indicated that loss of central VA occurred when the visual field was reduced to a remaining central 5–10 degrees.
A study of 84 Finnish patients with choroideraemia by Kärnä5 reported that good central vision was observed in the better seeing eye from the majority of 68 cases analysed (ages 3–69 years). He reported that 31 patients had a VA of at least 1.00 on the Snellen E chart (20/20 Snellen). In the remaining patients, the VA was 0.4–0.9 (approximately 20/25–20/50 Snellen) in 30 patients and 0.1–0.3 (20/70–20/200 Snellen) in three patients. The VA was worse than 0.1 (20/200 Snellen) in four patients, three of whom were 62 years of age or older. Although the author reported considerable variation in VA independent of age in his cohort of patients, he suggested that central vision at the age of 50 years was typically still sufficient for reading. Kurstjens6 studied 45 choroideraemia patients in the Netherlands and determined that VA usually remained good until age 40–50. He commented that a few patients still had reasonably good VA at approximately 50 years of age.
We analysed the central VA in a large group of patients with choroideraemia to comprehensively determine the degree and rate of change of their VA impairment. Our analysis provides clinically useful information about central VA retention in this progressive retinal degeneration.
MATERIALS AND METHODS
A retrospective review of all patient data from three tertiary care centres in the United States was completed on patients diagnosed with choroideraemia. The diagnosis was made if the following characteristics were present: a history of nyctalopia, peripheral visual field loss, a genetic transmittance pattern consistent with X linked disease, and a characteristic fundus appearance of extensive RPE and choroidal atrophy. One of us (MFR) initially reviewed all pertinent patient records (n = 95) at two sites (sites I and II) to document the best corrected VA, patient age, number of years of follow up, presence and extent of ocular media opacification, and any coexisting eye disease at the patients' initial and subsequent visits. A similar review was completed by RGW for the patients (n = 24) included from the third site (site III). Four patients were excluded either because of clinically significant lens opacities (n = 1) or insufficient information available in their clinical record (n = 3). All VA data were converted to logMAR equivalents of Snellen acuity for the purpose of analysis. We used a value of 1/400 Snellen (logMAR = 2.6) to represent vision of counting fingers and used extrapolated values of 2.7, 2.8, and 2.9 logMAR to represent hand movement, light perception, and no light perception, respectively.
The final study cohort of 115 included 53 patients from 44 families who were seen at the Eye and Ear Infirmary of the University of Illinois at Chicago, Department of Ophthalmology and Visual Sciences (site I), 38 patients from 34 families who were seen at the Jules Stein Eye Institute of the University of California at Los Angeles, Department of Ophthalmology (site II), and 24 patients from 22 families who were seen at the Casey Eye Institute of the Oregon Health Sciences University (site III). In two instances, different individuals from the same family were followed at two different sites (I and II). When available, all affected members of a single family were included.
A cross sectional analysis was obtained on all patient data (n = 115) to investigate the VA of the better seeing eye at the most recent visit. Twenty year age interval subgroups were utilised as part of this analysis, and multiple logistic regression was used to predict the odds of certain VA levels as a function of age.
As part of this investigation, we also conducted a longitudinal analysis on a subset of 45 patients who had been seen on at least three separate visits over a minimum follow up period of 4.5 years. Included in this component of the analysis were 19 patients from site I, 22 patients from site II, and four patients from site III. With the data from the initial and most recent visits, a 5 year rate of VA change was calculated by analysing the change in VA in the better seeing eye over the course of follow up. Multiple linear regression was then used to explore the 5 year rate of change as a function of initial age and initial VA. For the purpose of this analysis, we assumed that change in VA over time was a linear function. We felt justified in using this approach since we are unaware of any published data that document a functional relation other than linear for VA change in patients with choroideraemia.
RESULTS
Cross sectional analysis
A cross sectional analysis of the entire study cohort (n = 115) was done of the VA in the better seeing eye at their most recent visit. The mean (SD) age of the study cohort was 39.0 (17.5) years (range 5.2–88.4 years). The mean (SD) acuity in logMAR equivalents was 0.28 (0.51) (range −0.12 to 2.80) or approximately 20/40+ Snellen acuity. A comparison of data from the three sites included in the cross sectional study was obtained (Table 1). The mean (SD) age at the most recent visit was 36.5 (16.0) years (n = 53) for site I, 38.7 (16.5) years (n = 38) for site II, and 44.8 (21.2) years (n = 24) for site III. A one way ANOVA did not indicate a statistically significant difference in age at the most recent visit among the three sites (p = 0.16). The mean (SD) VA at the most recent visit was 0.23 (0.51) logMAR equivalent for site I, 0.23 (0.25) logMAR equivalent for site II, and 0.46 (0.76) logMAR equivalent for site III. Again, a one way ANOVA did not indicate a statistically significant difference in mean VA at the most recent visit from the three sites (p = 0.16).
Cross sectional cohort (n = 115) characteristics
Among the total group, 91 of 115 or 79%, had a VA that was equal to or better than 20/40 in their better seeing eye at the most recent visit (Table 2). Thirteen of the 115 patients (11%) had a VA worse than 20/40 to better than or equal to 20/70. A small number of patients with poorer acuity in the better seeing eye fell into one of two categories: worse than 20/70 to better than 20/200 (n = 3 of 115 or 3%) or 20/200 or worse (n = 8 of 115 or 7%). Thus, a substantial majority of the 115 patients had a VA of 20/40 or better in at least one eye at their most recent examination.
Cross tabulation of data from 115 choroideraemia patients at their most recent visit by age subgroup and VA range
A breakdown of the 115 patients by age subgroup revealed that the majority of patients were either 20–39 years of age (42 of 115) or 40–59 years of age (43 of 115). Fewer patients were found in the younger category (less than 20 years of age) 18 of 115 and older category (60 years of age or older) 12 of 115.
When analysing the cross sectional data by 20 year age subgroup, we found that, overall, patients younger than 60 years of age generally had better VA than those who were 60 years of age or older (also in Table 2). The majority of patients less than 60 years of age (87 of 103 or 84%) had a VA of 20/40 or better. Of the patients equal to or greater than 60 years of age, 33% (four of 12) had a VA better than or equal to 20/40, while 33% (four of 12) had a VA of 20/200 or worse. We observed that 50% (four of eight) of patients with vision worse than 20/200 were in the 60 years of age or older subgroup.
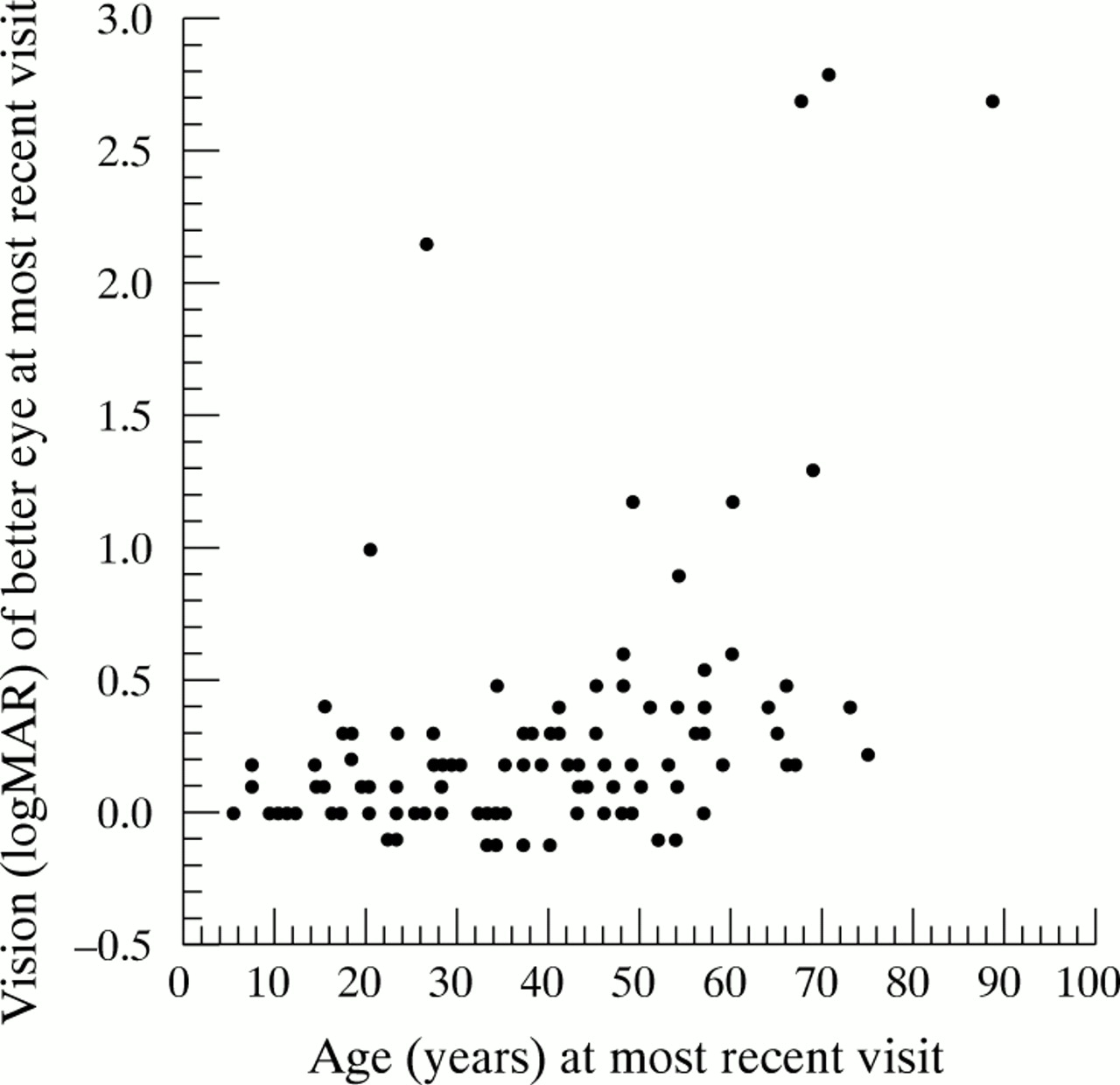
Using logistic regression to evaluate the cross sectional data in our cohort of patients, we found a strong relation between actual age and dichotomised VA in the better seeing eye at the most recent visit (Fig 1). To summarise, the odds of a VA worse than 0.3 logMAR equivalent (Snellen = 20/40) increased by a factor of 1.4 (95% CI = 1.2 to 1.7) for each 5 year age increment. Virtually identical results (1.4x, 95% CI = 1.1 to 1.7) for each 5 year age increment were obtained for the odds of a VA at the most recent visit in the better seeing eye being worse than 0.5 logMAR equivalent (Snellen≈20/60 to 20/70).
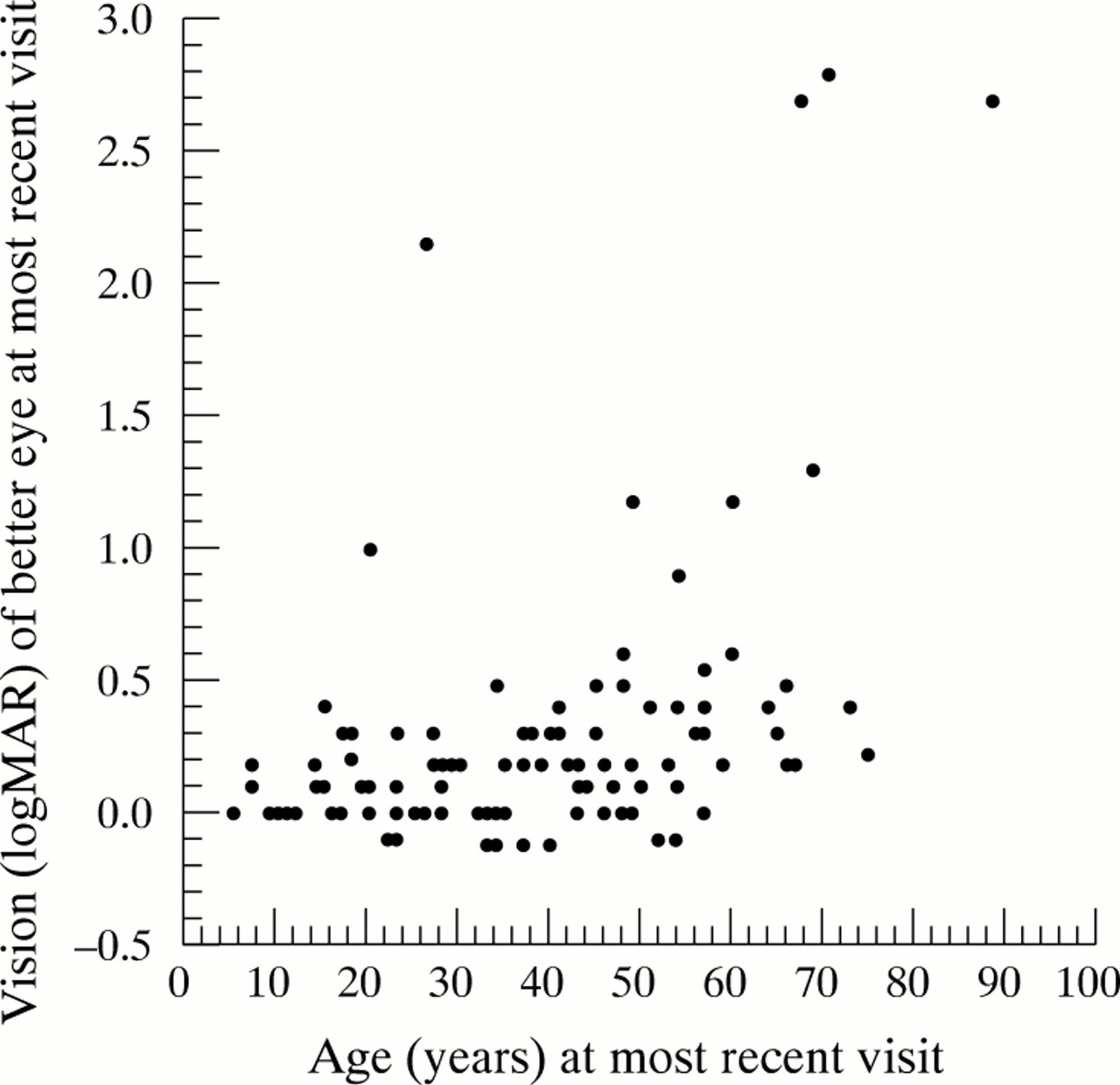
Cross sectional analysis. Scatter plot of the VA in the better seeing eye at the most recent visit.
Longitudinal analysis
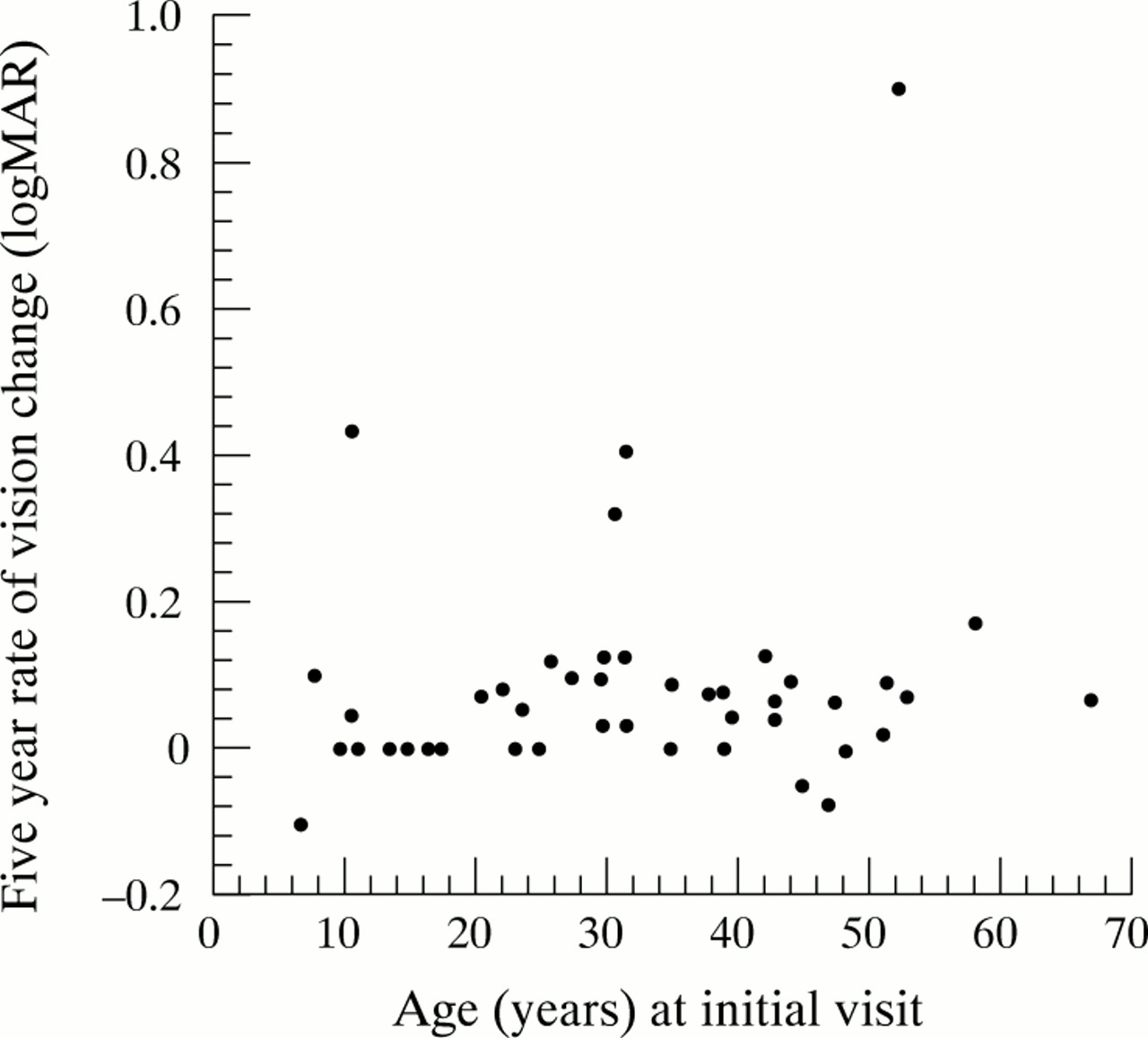
The mean (SD) 5 year rate of change in VA for our longitudinal cohort (n = 45) was calculated to be 0.09 (0.16) logMAR equivalent, or approximately one line on the Lighthouse chart (2nd ed).7 Although there appeared to be a tendency towards an increasing rate of VA change with increasing age, linear regression analysis of our longitudinal subgroup did not detect a significant relation between age at the initial visit (while controlling for baseline VA in the better seeing eye) and the 5 year rate of VA change (p = 0.44) (Fig 2). Likewise (while controlling for age at the initial visit) a significant relation between VA and the 5 year rate of change was not detected. Most of the cohort (93%) had a slow rate of change in VA (≤0.13 logMAR equivalent/5 years).

{kind=link}
{kind=link}
Longitudinal analysis. Scatter plot of the 5 year rate of change in VA relative to age at initial visit.
We evaluated the inclusion and exclusion groups for the longitudinal analysis as to their age and the VA of the better seeing eye at the initial visit. The mean (SD) age at initial visit of the inclusion group (n=45) was 31.8 (15.1) years (range 6.7–66.9 years). This was not statistically different (two sample t test, p = 0.37) from the mean (SD) age (34.7 (17.8) years) at initial visit of the exclusion group (n = 70). However, the mean (SD) initial VA of the inclusion group was 0.08 (0.14) logMAR equivalent compared to 0.28 (0.58) logMAR equivalent for the exclusion group. While this difference in VA at the initial visit was statistically different (two sample t test, p = 0.007), the amount of difference (two lines on the Lighthouse chart, 2nd ed) was clinically relatively minor.
A comparison of the longitudinal subgroup data (n = 45) was performed among the three sites (Table 3). A comparison of age at initial visit for patients from sites I and II indicated no statistically significant difference (two sample t test, p = 0.51). Further, a comparison of VA in the better seeing eye at the initial visit did not indicate a statistically significant difference (two sample t test, p = 0.09) in the patient data from sites I and II. Site III was not included in the comparisons owing to the small number of patients from this site who met the inclusion criteria for the longitudinal analysis.
Longitudinal cohort* (n = 45) characteristics
For the longitudinal subgroup, the initial visit VA data were quite homogeneous (Table 4). Nearly all (42 of 45 or 93%) of the patients had a VA of 0.18 logMAR equivalent (Snellen = 20/30) or better in the better seeing eye. Since the observed average 5 year rate of VA change was 0.09 logMAR equivalent (approximately one line on the Lighthouse chart, 2nd ed), it is clear that most of the patients in the longitudinal subgroup had good VA at baseline and experienced very little change during the course of follow up.
Data from 45 patients included in the longitudinal analysis
DISCUSSION
In the literature to date, the age at which patients with choroideraemia will experience severe loss of VA has been variably reported to occur “by middle age” to beyond the age of 50 years.1,5,6,8,9 In the present study of 115 patients with choroideraemia, we found that the most severe VA impairment did not occur until the seventh decade of life (after 60 years of age). That is, a VA of counting fingers or worse was observed only in patients above 60 years of age (n = 3). The majority of patients in the overall study group (91 of 115 or 79%) had good VA (20/40 or better) at their most recent visit. When analysing a longitudinal subgroup (n = 45), we calculated the average 5 year rate of VA change to be 0.09 (0.16) logMAR equivalent, or approximately one line. This rate is within the short term variation of VA testing.10 Good initial VA in this subgroup, combined with a slow rate of acuity change provides a favourable prognosis for the retention of VA until a more advanced age than has been previously reported.
In the cross sectional analysis, we considered the possibility that our analysis might be spuriously skewed by the inclusion of four individual outliers with more severely reduced VA (worse than 2.0 logMAR or 20/2000 Snellen equivalent in the better seeing eye at their most recent visit). The mean (SD) age of the study cohort was 39.0 (17.5) years (range 5.2–88.4 years). The mean age without these four individuals was 38.1 (16.6) years, a negligible difference. The mean (SD) acuity in logMAR equivalents for the total group was 0.28 (0.51) (range −0.12–2.80) or approximately 20/40+ Snellen acuity. The mean acuity without the four individuals was 0.20 (0.26) logMAR equivalent (20/32 Snellen). The difference of 0.08 logMAR (four letters) is also clinically negligible. In the longitudinal subgroup, one notable individual (age 66 at the most recent visit) had a marked decline in VA from 20/40 to hand movement in 12 years. This individual was observed to develop elevated intraocular pressure in both eyes, which may have contributed to his visual loss.
The inclusion of patient data from three tertiary eye care centres has potential to lead to selection bias. We attempted to reduce the effect of this potential bias for both our longitudinal and cross sectional analyses by including all eligible patients from each site. VA measurements were made by trained personnel at all three sites who were experienced in acuity measurement and refractive techniques. When analysing the longitudinal data by site, no statistically significant differences in mean age and mean VA at initial visit were found for the two major sites (sites I and II). Similarly, when comparing both the mean age at baseline and the mean VA at the most recent visit for the cross sectional group, no statistically significant differences were found among the three sites.
Any retrospective study of this nature is subject to potential selection bias. It is conceivable that, in our longitudinal study, patients with worse visual outcomes over time were less likely to return for the minimum 4.5 years required for inclusion. This could potentially lead to a more optimistic prognosis for visual acuity. It is relevant in this regard that we did observe a statistically significant two line less initial mean visual acuity between those included versus those excluded from this longitudinal study. This difference was not accounted for by a difference in age at the initial visit between these two groups. However, our statistical assessment of visual acuity at the initial visit between these two groups showed a considerably greater standard deviation in the excluded group. Of 70 patients in the exclusion group, 49 had an initial VA within the mean (SD) (equal to or better than 0.22 logMAR equivalent) of the inclusion group. Thus, 21 patients (less than a third of the exclusion group) who had a greater degree of initial VA impairment accounted for the overall difference between the two groups. It is therefore unlikely that selection bias would have had an untoward impact on our conclusion that, overall, patients with choroideraemia have a favourable prognosis for the retention of substantial central vision.
The findings from the present study should be useful for counselling patients with choroideraemia as to the degree and likely rate of visual acuity loss experienced by patients with this disease.
Acknowledgments
Supported in part by the Foundation Fighting Blindness (centre grants), Hunt Valley, Maryland, the Illinois Society for the Prevention of Blindness and the Grant Healthcare Foundation, Chicago, IL, core grant EY01792 from the National Eye Institute, National Institutes of Health, Bethesda, Maryland, and by an unrestricted grant (University of Illinois) and Distinguished Clinician-Scientist Award (JRH) from Research to Prevent Blindness, Inc, New York, USA.
Presented in part at the annual meeting of the Association for Research in Vision and Ophthalmology, Ft Lauderdale, FL, May 2001.
The authors do not have any proprietary interest in this work.