Article Text

Abstract
Aims: To determine the eligibility for laser photocoagulation treatment or for photodynamic therapy (PDT) with verteporfin in eyes at the earliest stage (first month of symptoms) of exudative age related macular degeneration (AMD) based on fluorescein angiographic (FA) features; to evaluate the potential contribution of indocyanine green angiography (ICG-A) for occult choroidal neovascularisation (CNV) at this stage.
Methods: Retrospective review of 252 consecutive patients (269 eyes) examined within the first month of symptoms of exudative AMD.
Results: On FA, 97 eyes (36%) had classic CNV alone. Occult CNV associated with fibrovascular retinal pigment epithelium detachments (PEDs) was observed in 71 eyes (26%) and without fibrovascular PED in 101 eyes (38%). 91 eyes (34%) met the Macular Photocoagulation Study criteria for laser photocoagulation. 53 eyes (20%) met the Verteporfin In PDT (VIP) or Treatment of AMD with PDT (TAP) studies criteria. By ICG-A, occult CNV was visualised as focal spots in 49% of eyes examined within 15 days v 32% of eyes examined between 16 and 30 days after the onset of symptoms (p=0.07). 8.5% of late staining plaques disclosed in eyes examined within 15 days were combined with focal spots v 36% in eyes examined between 16 and 30 days (p<0.01).
Conclusions: Early examination of eyes with exudative AMD would allow the treatment of 47% of eyes. 60% of eyes with subfoveal CNV would be eligible for PDT with verteporfin. Up to half of eyes with occult CNV would be converted by ICG-A into well delineated focal spots.
- age related macular degeneration
- fluorescein angiography
- laser photocoagulation
- photodynamic therapy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- DA, disc area
- FA, fluorescein angiography
- FAZ, foveal avascular zone
- ICG-A, indocyanine green angiography
- PDT, photodynamic therapy
- PEDs, pigment epithelium detachments
- VA, visual acuity
- age related macular degeneration
- fluorescein angiography
- laser photocoagulation
- photodynamic therapy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- DA, disc area
- FA, fluorescein angiography
- FAZ, foveal avascular zone
- ICG-A, indocyanine green angiography
- PDT, photodynamic therapy
- PEDs, pigment epithelium detachments
- VA, visual acuity
Statistics from Altmetric.com
- age related macular degeneration
- fluorescein angiography
- laser photocoagulation
- photodynamic therapy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- DA, disc area
- FA, fluorescein angiography
- FAZ, foveal avascular zone
- ICG-A, indocyanine green angiography
- PDT, photodynamic therapy
- PEDs, pigment epithelium detachments
- VA, visual acuity
- age related macular degeneration
- fluorescein angiography
- laser photocoagulation
- photodynamic therapy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- DA, disc area
- FA, fluorescein angiography
- FAZ, foveal avascular zone
- ICG-A, indocyanine green angiography
- PDT, photodynamic therapy
- PEDs, pigment epithelium detachments
- VA, visual acuity
Choroidal neovascularisation (CNV) is responsible for nearly 90% of severe visual loss occurring in age related macular degeneration (AMD). Several clinical trials carried out in Europe and in the United States have established the benefit of laser photocoagulation treatment for patients with classic CNV.1–7 Verteporfin photodynamic therapy (PDT) was shown to be effective for eyes with predominantly classic subfoveal CNV.8 Recent data from the Verteporfin In PDT (VIP) Study suggest that the latter treatment is also effective for eyes with subfoveal occult CNV.9
Few studies have attempted to describe the features of CNV at a very early stage of exudative AMD10 or to determine the proportion of eyes that fulfil the MPS eligibility guidelines based on fluorescein angiography (FA) for laser photocoagulation treatment11,12 or the Treatment of AMD with PDT (TAP) Study criteria for verteporfin.13 Moreover, no study of the impact of the recent guidelines for PDT with verteporfin in eyes with subfoveal occult CNV is available yet.
Indocyanine green angiography (ICG-A) is suggested to improve imaging of occult CNV, though current therapeutic guidelines rely only on FA findings.14–22 However, few data are available about the specific contribution of ICG-A at a very early stage of exudative AMD.
This study was designed to analyse the initial angiographic features of CNV in exudative AMD, to specify the proportion of eyes that meet the MPS eligibility criteria for laser photocoagulation treatment or the TAP and VIP studies criteria for PDT with verteporfin based on FA, and to determine the potential contribution of ICG-A at the early stage of the disease.
MATERIALS AND METHODS
The charts of 2118 consecutive patients presenting for the first time at the eye university clinic of Creteil (France) between 1 September 1998 and 30 September 1999 were reviewed retrospectively. The eye university clinic serves mainly as a tertiary referral centre, but also as a primary care provider.
Inclusion criteria were each of the following: age >50 years; exudative (neovascular) AMD diagnosis based on the criteria of the International ARM Epidemiological Study Group23; patients examined within 1 month after onset of visual symptoms (loss of visual acuity, metamorphopsia, micropsia) with FA and possibly ICG-A (when FA showed occult CNV) performed at presentation.
Exclusion criteria were any of the following: (1) patients treated by laser photocoagulation in the posterior pole before referral, (2) presence of any other cause of choroidal neovascularisation such as degenerative myopia, angioid streaks, chorioretinal inflammatory diseases, hereditary retinal disorders, presumed ocular histoplasmosis syndrome, (3) clinical history or fluorescein angiographic documentation performed within 30 days after the onset of symptoms unavailable or not gradable.
Data concerning ophthalmological history, duration of symptoms, best corrected distance (determined with modified Early Treatment Diabetic Retinopathy Study 2 metre charts) and reading visual acuity, slit lamp biomicroscopy examination of the anterior segment, and ophthalmoscopy by means of a Goldmann contact lens or a 90 dioptre lens were recorded.
Fluorescein angiograms were performed using standard cameras. ICG-A was performed on the same day using one of two different infrared angiographic systems: an infrared fundus camera (Topcon 50IA, Topcon Imagenet, Tokyo, Japan) connected to a digitising system (Topcon Imagenet, Rotterdam, Netherlands) or a scanning laser ophthalmoscope (Heidelberg retina angiograph, Heidelberg Engineering, Heidelberg, Germany). The earliest angiographic documentation was studied. Informed consent was obtained from each patient before angiographies were performed.
For FA analysis, the MPS Group terminology24 was used to define areas of serous pigment epithelial detachment, classic CNV, and occult CNV (type 1 corresponding to fibrovascular pigment epithelial detachment (PED); type 2 corresponding to late leakage of undetermined source). Location of CNV was defined according to the MPS terminology3–5,24: extrafoveal (that is, more than 200 μm between the centre of the foveal avascular zone (FAZ) and the posterior edge of CNV), juxtafoveal (that is, CNV extending between 1 μm and 199 μm from the centre of the FAZ), and subfoveal (that is, CNV extending under the centre of the FAZ). On fluorescein angiography (FA), presence and location of classic and/or occult choroidal neovascularisation (CNV) as well as size of lesions with subfoveal classic CNV were recorded. The size of the subfoveal CNV complex was determined using an MPS disc area (DA) template as described previously.24
Laser photocoagulation treatment according to the MPS group strict eligibility criteria could be considered only for eyes with classic CNV alone (for extrafoveal and juxtafoveal CNV3,4) or with at least some classic CNV (for subfoveal CNV5). Other criteria included VA,3–5,7 size of the CNV lesion (according to the revised recommendations for the subfoveal group),7 extent of the CNV within the exudative lesion (at least 50% of any subfoveal neovascular complex),5 and location of the CNV (not further than 2500 μm from the foveal centre).3,4
Eyes were considered eligible for verteporfin PDT if they met the criteria used by the TAP8 or the VIP9 studies based on FA. According to the TAP Study criteria, the presence of subfoveal CNV and an area of CNV covering at least 50% of the area of the total neovascular lesion were required. VA had to be between 20/40 and 20/200. PDT with verteporfin was recommended for eyes with predominantly classic CNV (that is, an area of classic CNV equal to or greater than 50% of the area of the entire CNV lesion). According to the VIP Study recommendations, eyes with progressing occult subfoveal CNV and either small lesions (four disc areas or less) or low level of VA (≤20/50 but ≥20/100) were also considered amenable to PDT with verteporfin.
For ICG-A analysis in eyes with occult CNV by FA, the terminology of Guyer et al25 was used. Thus “focal spots” (or hot spots) represented a subretinal exudation that appeared as occult CNV by FA and as a hyperfluorescent lesion less than one disc area in size by ICG-A. Focal spots that are well delineated20 have been considered as potentially treatable by ICG guided laser photocoagulation given their small size and their often extrafoveal location.25 “Plaques” represented a subretinal exudation that appears as occult CNV by FA and as a hyperfluorescent lesion larger than one disc area in size by ICG-A. Their site is usually subfoveal. Plaques characteristically did not stain early in the angiogram and fluoresced less intensely than a hot spot in the late phase.25 Fibrovascular PEDs were classified on ICG-A on the basis of the respective location of the hot spot and the plaque. Whenever a distinct lacy network was visible on the early frames of ICG-A, this was also recorded.
Angiographic features were initially determined by the senior ophthalmologist who examined the patient in our clinic. The angiograms were reviewed independently by one of the authors (WMH). Differences were adjudicated by a second author (GC or GS).
The data were analysed using standard statistical methods. The relations between categorical variables were examined using Pearson's χ2 test. For small size samples, χ2 test with Yates's correction was used. Differences were considered significant when the probability of their occurrence by chance was less than 5%.
RESULTS
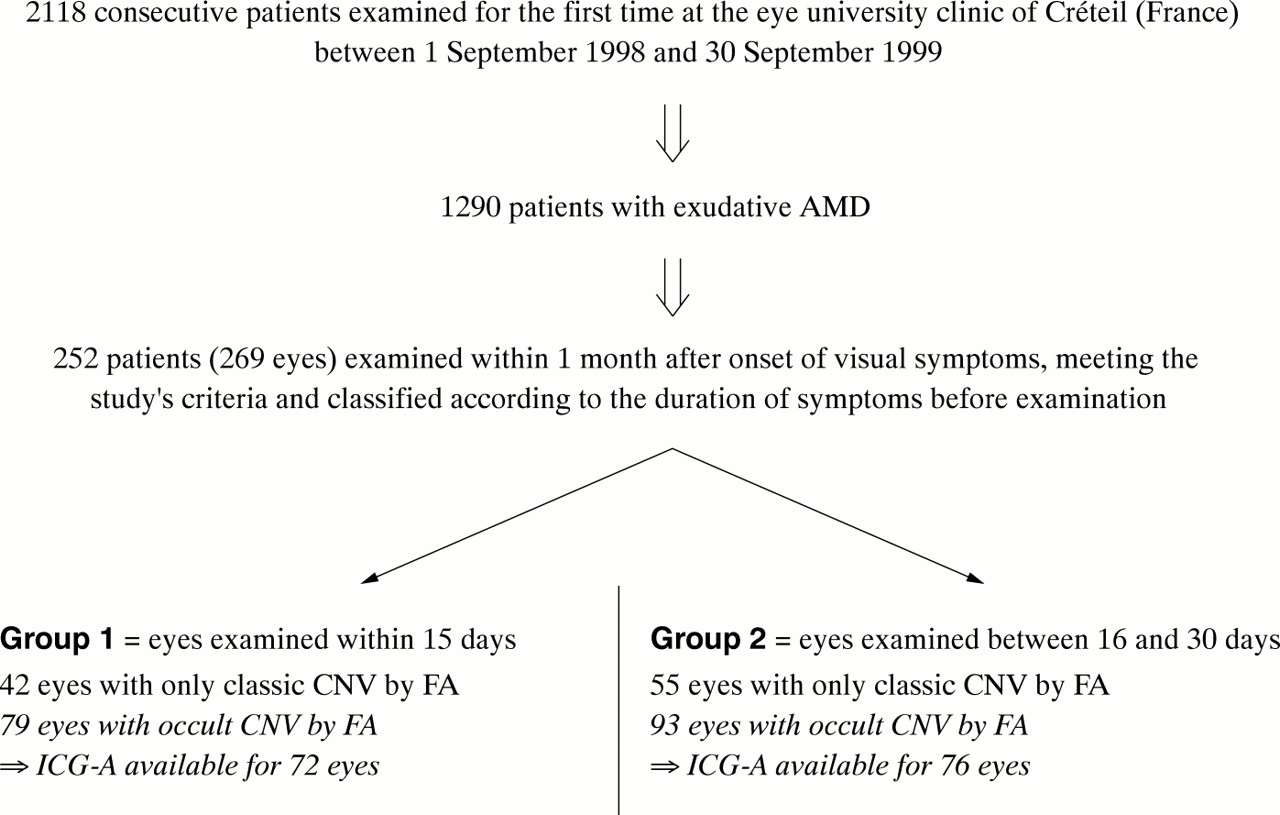
A total of 1290 patients presented with exudative AMD; 252 patients (269 eyes) met the above eligibility criteria (Fig 1). In all, 137 out of 252 patients were women (54%) and 115 men (46%). Mean age was 74.8 years (range 50–97). Initial VA of the 269 studied eyes (112 first eyes and 157 second eyes) was distributed as shown in Table 1. Mean duration of visual symptoms was 18.7 days (range 0–30 days) (Table 2).
Best corrected ETDRS visual acuity distribution according to the type of CNV
Mean duration of visual symptoms

Presentation of the study patient groups.
Angiographic findings are summarised in Figure 2. In addition, angiographic features were compared between eyes examined within 15 days of the onset of symptoms (group 1; 121 eyes) and those examined between 16 and 30 days after onset of symptoms (group 2; 148 eyes).

{kind=link}
{kind=link}
Distribution of fluorescein and indocyanine green angiographic features and eligibility for treatment at the early stage (within 30 days of symptoms) of exudative age related macular degeneration.
FA features
FA was available for all eyes. Classic CNV alone was disclosed in 97 eyes (36%). The location of classic CNV was extrafoveal in 23 of these eyes (24%), juxtafoveal in 50 (51%), and subfoveal in 24 (25%).
The rates of extrafoveal, juxtafoveal, and subfoveal classic CNV were respectively 29% (12 eyes), 55% (23 eyes), and 16% (7 eyes) in group 1 v 20% (11 eyes), 49% (27 eyes), and 31% (17 eyes) in group 2. These differences did not reach statistical significance.
Occult CNV was identified on FA in the remaining 172 eyes (64%).
Isolated occult CNV (occult CNV without fibrovascular PED or MPS type 2) was present in 101 eyes (38%). The location of isolated occult CNV was extrafoveal in 18 of these eyes (18%), juxtafoveal in 39 (39%), and subfoveal in 44 (43%). Mixed CNV (associated occult and classic CNV) was detected in 25 eyes (9% of all eyes). The location of mixed CNV was subfoveal in eight of these 25 eyes (32%).
Among the 101 eyes with isolated occult CNV, the rates of extrafoveal, juxtafoveal, and subfoveal CNV were respectively 22% (11 eyes), 37% (18 eyes), and 41% (20 eyes) in group 1 v 14% (seven eyes), 40% (21 eyes), and 46% (24 eyes) in group 2. These differences did not reach statistical significance.
Occult CNV with fibrovascular retinal PEDs (MPS type 1) was present in 71 eyes (26%). The location of CNV was extrafoveal in 16 of these eyes (22%), juxtafoveal in 19 (27%), and subfoveal in 21 (30%) whereas in 15 eyes (21%) FA was unable to identify the location or extent of the underlying CNV. Pretear characteristics26 were present in two eyes and chorioretinal anastomoses were suspected in three additional eyes. In one eye, a recent tear of the fibrovascular PED did not involve the foveal area.
Eligibility for treatment
A total of 91 eyes (34% of all eyes) met the MPS eligibility criteria for laser photocoagulation treatment. The distribution of these 91 eyes by location and type of CNV is shown in Table 3. In all, 41 out of these 91 eyes were included in group 1 v 50 in group 2.
Eligibility for laser photocoagulation treatment according to the Macular Photocoagulation Study Group (MPS) criteria in 122 eyes with classic (well defined) CNV
A total of 53 eyes (20% of all eyes or 60% of eyes with subfoveal CNV based on FA) were eligible for PDT with verteporfin based on either the TAP or the VIP studies' guidelines (Table 4).8,9 A total of 31 eyes (12% of all eyes or 35% of eyes with subfoveal CNV) with subfoveal purely occult CNV and either small lesions (four disc areas or less) or low level of VA (≤20/50 but ≥20/100) met the VIP Study recommendations. A further 22 eyes (8% of all eyes or 25% of eyes with subfoveal CNV) with subfoveal predominantly classic CNV met the TAP Study criteria. Reasons for not meeting the criteria for PDT with verteporfin in the remaining 36 eyes with subfoveal CNV are listed in Table 4.
Eligibility for photodynamic therapy (PDT) with verteporfin based on either the TAP or the VIP studies guidelines in eyes with subfoveal CNV (89 out of 269 eyes)
Overall, 126 eyes (47%) were classified as treatable either by verteporfin PDT or by laser photocoagulation treatment based on FA.
ICG-A features
In all, 70 out of 137 patients (148 eyes) evaluated with ICG-A were women (51%) and 76 men (55%). Mean age was 73.7 years (range 55–94). Mean duration of visual symptoms in those 137 patients was 18.9 days (range 0–30 days). ICG-A was performed whenever FA disclosed occult CNV. However, it was not available for 24 out of 172 eyes with occult CNV by FA (14%): 15 patients who refused another dye injection on the same day and nine patients who experienced minor adverse effects during the course of FA.
A total of 91 out of 101 eyes with isolated occult CNV (MPS type 2) were studied by ICG-A (Table 5). ICG-A showed focal spots in 37 eyes (41%), plaques in 40 (44%), combinations of plaques and focal spots in 12 (13%), and was not contributive in the two remaining eyes.
Compared findings between FA and ICG-A in eyes with occult CNV examined within 1 month after the onset of symptoms
In eyes with fibrovascular PED (MPS type 1), ICG-A, available for 57 out of 71 eyes, showed focal spots in 22 out of 57 eyes (39%) of which 17 (77%) were nasally located (Table 5).
The anatomical location of CNV membranes by ICG-A was compared with FA findings (Table 5). In total, 55% of occult CNV were subfoveal based on ICG-A v 38% based on FA.
Overall, ICG-A demonstrated focal spots in 59 out of 148 eyes exhibiting occult CNV on FA (40%). Focal spots were extrafoveal in 32 of these eyes (54%), juxtafoveal in 18 (31%), and subfoveal in nine (15%). A distinct lacy network was detected on the early frames of ICG-A in 29 out of these 59 eyes (49%).
In 79 out of 148 eyes with occult CNV (53%), ICG-A showed a plaque, of which 19 were combined with focal spots. The percentage of plaques combined with focal spots was 8.5% in group 1 (three out of 35 plaques) compared with 36% in eyes in group 2 (16 out of 44 plaques). This difference was statistically significant (p<0.01).
In group 1, ICG-A, available for 72 out of 79 eyes with occult CNV, disclosed focal spots in 35 eyes (49%). In group 2, ICG-A, available for 76 out of 93 eyes with occult CNV, disclosed focal spots in 24 eyes (32%). This difference did not reach statistical significance (p=0.07).
DISCUSSION
Fluorescein angiographic features are currently determinant in the selection of CNV in exudative AMD regarding therapeutic approaches. In this study, 26% of all affected eyes (examined within 30 days after the onset of symptoms) had, on FA, extrafoveal or juxtafoveal classic CNV alone and were amenable to laser photocoagulation treatment according to the MPS guidelines.3,4 The overall rate of eyes eligible for treatment increased to 47% when subfoveal CNV was included and when both laser photocoagulation treatment and PDT with verteporfin (based on both TAP and VIP studies recommendations) were considered.
To the best of our knowledge, specific analysis of FA features at the very early stage of exudative AMD has been performed previously in only one study,10 which found classic CNV alone in only 13% of 67 eyes examined within 1 month of the onset of symptoms. The higher prevalence of classic CNV in our study (36%) could be related to the fact that patients with treatable disease might be preferentially sent to a referral centre. However, most of these patients have not been previously evaluated by FA. Conversely, patients examined by retinal specialists were referred to our clinic for evaluation with ICG-A mainly for occult CNV on FA. Of the 67 eyes (studied by Freund et al10) 51% v 26% in the present study had fibrovascular or serous PEDs or both. This difference could be related to different referral habits. Table 1 suggests that severe visual loss (<20/200) is more often present at the onset of exudative AMD associated with fibrovascular PEDs. This fact might possibly result in a more rapid referral of patients with fibrovascular PEDs.
The quest for the earliest possible stage of exudative AMD is obviously limited by the subjective nature of visual symptoms. However, it can be assumed that most patients are likely to define with acceptable accuracy the duration of recent symptoms (≤30 days) that was considered in this study. Effect of duration of symptoms was assessed by Grey et al27 who found that 43% of eyes examined between 3 and 4 weeks after the onset of symptoms were amenable to laser treatment based on FA v only 10% of those examined between 5 and 6 months in a series of 414 eyes. The duration of symptoms before performing FA did not restrict the entry in two previous studies which found respectively 26% (26 out of 100)11 and 30% (15 out of 50)12 of eyes with exudative AMD to be suitable for laser photocoagulation. In another retrospective review of fundus photographs and FA of 64 eyes (59 patients) with exudative AMD examined in a tertiary referral centre, Bressler et al28 found 44% of occult CNV. All eyes with PED were excluded from their study. With the same criterion, occult CNV on FA would be 51% in our study, a percentage in the same range.
Twenty per cent of eyes (corresponding to 60% of eyes with subfoveal CNV based on FA) were found to be eligible for PDT with verteporfin at the early stage of exudative AMD in this study. This study is the first to provide an estimate of the percentage of eyes with exudative AMD that are suitable for PDT with verteporfin taking into account the recent recommendations of the VIP Study for occult CNV.9 The impact of this study is even more important than that of the TAP Study, since our findings suggest that subfoveal isolated occult CNV represents 13% of all eyes at the earliest stage of the disease, of which the vast majority (86%, corresponding to 12% of all eyes) were included in the subgroup for which the VIP Study suggests a greater benefit of PDT with verteporfin (that is, eyes with either lesions of four disc areas or less or VA between 20/50 and 20/100).9 These results correspond to a 150% increase of the number of eyes eligible for PDT with verteporfin, compared with the criteria of the TAP Study alone for subfoveal predominantly classic CNV (8% of all eyes).8 In fact, only four out of 122 eyes with at least some classic CNV in our series that did not meet the MPS eligibility criteria (2% of all eyes) were treatable according to the TAP Study guidelines for PDT with verteporfin. These four eyes had large subfoveal lesions (>2 MPS disc areas) and VA of 20/160 or better and therefore did not meet the revised criteria of the MPS for subfoveal CNV.7 One potential limitation for our results is the fact that it is not always possible to ascertain whether occult CNV with ill defined borders extends into the foveal centre or not.
The percentage of eyes with occult CNV potentially treatable by verteporfin PDT in this study did not include eyes with fibrovascular PEDs. No explicit recommendation of PDT with verteporfin for these eyes is presently available. Increased rates of RPE tears following PDT with verteporfin for eyes with fibrovascular PEDs have been reported.29–31 Nevertheless, if those eyes were considered eligible for PDT with verteporfin, it would account only for a modest increase in the total number of treatable eyes (3%) since the majority of those eyes with subfoveal CNV based on FA (13 out of 21) had a VA of less than 20/100 at presentation and therefore did not meet the VIP Study guidelines.
In a recent study, 36% of eyes at all stages of exudative AMD were eligible for PDT with verteporfin based on the criteria of the TAP Study8 alone for subfoveal predominantly classic CNV13v 8% of eyes at the earliest stage of the disease in the present study (based on the same criteria). This difference is probably related to the progression of extrafoveal and juxtafoveal CNV towards the fovea at a later stage of the disease and to the development of classic CNV in eyes with only occult CNV at the early stage (occurring in up to 52% of these eyes during 9–12 months follow up32). Thus, 83% of eyes included in the series of Margherio et al13 had subfoveal CNV (of which 44% were predominantly classic) compared with 33% in our series based on FA (of which 25% were predominantly classic). Conversely, 17% of eyes had extrafoveal or juxtafoveal classic CNV alone eligible for laser photocoagulation treatment according to the MPS guidelines in the study of Margherio et al13v 26% of eyes in the present study. Whether long term visual prognosis is better for eyes with extrafoveal or juxtafoveal CNV treated by laser photocoagulation at an earlier stage or for eyes with subfoveal CNV treated by PDT with verteporfin at a later stage remains an open debate.
ICG-A was available for 148 out of 172 eyes (86%) with occult CNV by FA included in this study. Lack of ICG-A was because of refusal of the patients to have another dye injection on the same day or because of the occurrence of adverse effects during the course of FA. Therefore, it should not have influenced our overall results.
Precise data concerning duration of symptoms were not available in other studies14–17,19–25,33–36 of occult CNV in exudative AMD with ICG-A. In the largest study to date, a retrospective review of 1000 ICG-A by Guyer et al25 showed focal spots in 29% of eyes, plaques in 61%, and plaques combined with hot spots (combined lesions) in 8%, to compare with 40%, 40.5%, and 13% respectively in our results. ICG-A seems to contribute most at the early stage of the disease to delineate occult extrafoveal CNV by FA (Table 5). The improved detection of focal spots with ICG-A in eyes examined within 15 days compared to eyes examined between 16 and 30 days after the onset of symptoms in this study (49% v 32%) approaches but does not reach statistical significance (p=0.07). It seems plausible to assume that with a longer delay (> 15 days) between the two study groups, the difference might be even more dramatic. This fact is possibly related to the smaller size of the CNV membrane at an earlier stage and to the presence of a lesser amount of blood, pigment, serous exudation, fibrous tissue, and metabolic waste products within and around the neovascular tissue, allowing a better display of the border of the CNV membrane on ICG-A.
The percentage of plaques (believed to represent “inactive” occult CNV25) combined with focal spots (believed to represent “active” occult CNV25) was significantly increased (p<0.01) in eyes examined between 16 and 30 days after the onset of symptoms (36%) compared with eyes examined within 15 days (8.5%). This fact suggests that focal spots might develop and become distinct on ICG-A within plaques during the natural course. It might be considered similar to the development of classic CNV on FA in eyes with only occult CNV at presentation.32 Prospective and longitudinal studies are required to confirm this finding and to determine whether this progression occurs mostly during the early stages or more uniformly during the history of plaques. Duration of symptoms seems therefore to be an important parameter to consider when analysing FA and ICG-A results.
It must be emphasised that no randomised clinical trial has presently established the effectiveness of any therapeutic method based on ICG-A. Therefore, despite some encouraging results of ICG guided laser photocoagulation in a number of pilot studies18,19,21,33–36 and several reports of clinicopathological correlation of hyperfluorescence seen on ICG-A and histopathological proof of CNV,37–39 the therapeutic contribution of ICG-A remains uncertain. However, the improved imaging of occult CNV by ICG-A raises several questions that are still unanswered. The therapeutic implications of the distinction between “inactive” or “dormant” (that is, plaques) and “active” occult CNV (that is, focal spots) remain unknown. Focal spots corresponding to retinal choroidal anastomoses seem to be associated with a poor visual outcome40,41 whereas the prognosis of those corresponding to distinct lacy networks warrants further studies with longitudinal follow up. Moreover, ICG-A showed subfoveal involvement in 35% of eyes with isolated occult CNV considered as juxtafoveal based on FA. Further studies are required to determine if these eyes should be considered as candidates for PDT with verteporfin. Likewise, future clinical trials may determine if the effectiveness of PDT with verteporfin for occult CNV would be enhanced if the laser spot was chosen based on the extent of occult CNV on ICG-A.
This study represents a large series of consecutive eyes at a very early stage of exudative AMD and might be useful to provide further data about the natural history of the disease. Assuming that this series reflects rather fairly the distribution of angiographic patterns at the onset of the disease, our data suggest that subfoveal involvement is already present within the first month of symptoms in 44% of eyes (55% in eyes with occult CNV) whereas extrafoveal location is found in only 22% of eyes at this stage (whether with occult or classic CNV). Besides, this study might allow estimating the potential impact of new therapeutic means for eyes examined at an early stage.
In conclusion, this study suggests that 47% of eyes examined within 1 month after the onset of symptoms of exudative AMD would be treatable, either by laser photocoagulation or verteporfin PDT based on the current guidelines. Up to 34% of eyes might benefit at this stage from laser photocoagulation treatment according to the MPS criteria. Sixty per cent of eyes with subfoveal CNV based on FA could be eligible for verteporfin PDT according to either the TAP or VIP studies' criteria. ICG-A seems to contribute most at this stage to the delineation of occult extrafoveal CNV by FA. However, further studies are still needed to establish the therapeutic benefit of the enhanced imaging of occult CNV by ICG-A.
Acknowledgments
The authors wish to thank Dr Agnés Glacet-Bernard (Eye University Clinic of Créteil) for providing statistical assistance.