Article Text

Abstract
Aim: To study the effect of the treatment of dry eye in Sjögren's syndrome patients with hypotonic or isotonic hyaluronate eye drops.
Methods: 40 Sjögren's syndrome patients were divided in two groups and treated as follows: group 1 with hypotonic (150 mOsm/l) 0.4% hyaluronate eye drops; group 2 with isotonic 0.4% hyaluronate eye drops. The eye drops were instilled six times a day for 90 days. Grading of subjective symptoms, break up time (BUT), corneal fluorescein staining, conjunctival rose bengal staining, Schirmer's I test, and conjunctival impression cytology were carried out at 0 and 15, 30, 90 days from the beginning of the study. Patients were examined in a blind fashion. For the statistical analysis the Student's t test, Mann-Whitney U test, and χ2 test were performed.
Results: Symptoms were statistically significantly improved at day 15 in both groups but group 1 patients had a global score statistically significantly better group 2 (p=0.02). At day 15 group 1 patients had an improvement from baseline values of BUT (p=0.003), fluorescein, and rose bengal score (p=0.000001 and p=0.0004 respectively). Group 2 patients had, at day 15, an improvement of BUT and fluorescein score compared to baseline values (p=0.05 and p=0.0001 respectively). A comparison between the two groups showed better results for group 1 patients at day 15 for rose bengal stain (p=0.01) and for BUT (p=0.05) and fluorescein score (p=0.0003) at day 90. The conjunctival impression cytology showed that group 1 had a statistically significant better total score than group 2 starting from day 15 and lasting throughout the study (p<0.02). Also group 2 patients showed an improvement from baseline values starting from day 30 (p=0.000005).
Conclusion: Hyaluronate eye drops are useful for treating severe dry eye in Sjögren's syndrome patients. The use of a formulation with pronounced hypotonicity showed better effects on corneoconjunctival epithelium than the isotonic solution.
- sodium hyaluronate
- hypotonic solution
- Sjögren's syndrome
- conjunctival impression cytology
Statistics from Altmetric.com
Sodium hyaluronate eye drops have been used in several trials for the treatment of dry eye.1–7 Experimental data show that sodium hyaluronate eye drops do not alter the normal conjunctival epithelium, as may happen with other lacrimal substitutes. In fact, these do not interfere with secretory processes of goblet cells and do not damage the intercellular junctions as may happen with other tear substitutes.8 Sodium hyaluronate eye drops increase precorneal tear film stability and corneal wettability, reduce the tear evaporation rate, and the healing time of corneal epithelium.4,5,9–12
Tear hyperosmolarity has been shown to be a main pathogenetic factor in dry eye and tear osmometry was suggested as a diagnostic tool for dry eye.13,14 An increased tear osmolarity was shown to be responsible for the presence of symptoms and epithelial changes in dry eye, since experimental studies on tissue cultures showed a toxic effect of hyperosmolarity on epithelial cells.15 Owing to the effects of hyperosmolarity on the ocular surface, it was claimed that a good tear substitute for dry eye patients should be hypotonic.16 However, therapies with hyposmotic agents in dry eye patients gave contradictory results since it was reported that dry eye patients prefer such treatment,17 but other data indicate no differences between the results with hypo-osmolar or iso-osmolar eye drops.6,18
The purpose of the present study was to evaluate the efficacy of two commercially available solutions of 0.4% sodium hyaluronate, with different osmolarity, in Sjögren's syndrome patients with severe dry eye.
MATERIALS AND METHODS
Patient population
Forty Sjögren's syndrome patients, 16 primary and 24 secondary (35 female and five male with a mean age of 44.7 (SD 10.8) years, range 22–67 years) were enrolled in the study. The 24 cases of secondary Sjögren's syndrome were in association with the following autoimmune diseases: 10 rheumatoid arthritis, five mixed connective tissue disease, four Hashimoto's thyroiditis, three systemic lupus erythematosus, two systemic sclerosis. Inclusion criteria were: fulfilment of the European diagnostic criteria for primary or secondary Sjögren's syndrome19 with a Schirmer's I test, without anaesthesia, lower or equal to 5 mm/5 minutes and signs of corneoconjunctival epithelium suffering shown at fluorescein and rose bengal stains with a score higher than 314; a well controlled systemic autoimmune disease stable for at least 2 months before the beginning of the study and unchanged during the course of the study; a systemic therapy unchanged for at least 2 months before the beginning of the study and during the study; absence of any ocular treatment other than tear substitutes, which were used according to their needs.
Exclusion criteria were presence of any ocular disease, present or past, other than dry eye; use of contact lens; presence of systemic diseases other than those related to Sjögren's syndrome; use of topical and/or systemic treatments potentially interfering with tear productions (tranquillisers, antidepressants, monoamine oxidase inhibitors, dopaminergics, neuroleptics, benzodiazepines, antiserotonergics, antiemetics, sleeping tablets, β blockers, hormones).
All the subjects who enrolled in the study gave informed consent.
Treatment
All patients included were treated for a run-in period of 7 days with one eye drop of saline six time a day. At the end of this period (time 0 of the study) the subjects were randomly divided into two groups and assigned to a treatment by personnel not involved with the patients' examination.
The visits and cytological examinations were carried out in a blind fashion by investigators who were not aware to which group the patients belonged. The study drugs were commercially available eye drops and the two groups were treated as follows: group 1 (17 female and three male, age 44.3 (9.8)) with unpreserved hypotonic (150 mOsm/l) 0.4% sodium hyaluronate eye drops (Ialurex, Fidia Oftal, Catania, Italy); group 2 (18 female and two male, age 44.7 (12)) with 0.4% unpreserved isotonic sodium hyaluronate eye drops (Dropstar TG, Farmigea, Pisa, Italy). In both eye drops the sodium hyaluronate had a molecular weight of 750 000 D. The eye drops were administered six times a day for 90 days and the subjects enrolled in the study underwent grading of subjective symptoms and clinical examination at time 0 and after 15, 30, and 90 days.
The patients were allowed to know the brand name of the eye drops they were using. They were asked to bring, at all visits, the used boxes of the eye drops in order to control the compliance with the study protocol.
Tests performed
The following symptoms were evaluated according to a scoring system from 0 (absent) to 3 (severe): burning, foreign body sensation, dryness, mucous discharge, itching, photophobia; a global score, obtained adding the score of each symptom, was considered for the evaluation of ocular discomfort.
The following tests were performed: break up time (BUT) (seconds), corneal fluorescein and conjunctival rose bengal vital staining,14 Schirmer's I test (mm/5 minutes), and conjunctival impression cytology.
For conjunctival impression cytology acetate cellulose filters (Millipore, GSWP02500, pore size 0.22 μm) were cut into pieces, approximately 4 × 5 mm in size, and were applied to the bulbar conjunctiva, gently pressed for 3–4 seconds and then removed. Specimen collection was carried out on bulbar conjunctiva at the 12 o'clock position, 3 mm from the limbus.
The specimens were fixed for at least 10 minutes in a solution of glacial acetic acid: 37% formaldehyde: absolute alcohol: distilled water in the proportion of 1:1:14:6. The specimens were stained with PAS-Papanicolaou stain according to Gill et al20 and evaluated according to a previously described scoring system.21–23 Seven parameters were evaluated—specimen cellularity, cell to cell junction, nucleus/cytoplasm ratio, nuclear chromatin, goblet cell distribution, keratinisation, presence of inflammatory cells. For each parameter a score was attributed: 0 for normal pattern, 1 for borderline pattern, 2 and 3 (only for keratinisation and inflammatory cells presence) for abnormal patterns. A total score was obtained adding the results of each parameter and the specimen was classified, according to the total score, into three classes: class A (score 0–3) normal features, class B (score 4–6) borderline features, class C (score >6) abnormal features (Table 1).
Conjunctival impression cytology parameters with the scoring system and the classes of cytology
Statistical analysis
Primary efficacy variables were considered—the global symptoms score and the impression cytology scores. The statistical analysis of the results was carried out in a blind method by a person not involved in the study, using the software sas (version 8.1). Only the results of right eyes were considered for statistical analysis. Student's t test, Mann-Whitney U test, and χ2 test were used as appropriate. A value of p <0.05 was considered statistically significant.
RESULTS
Symptoms
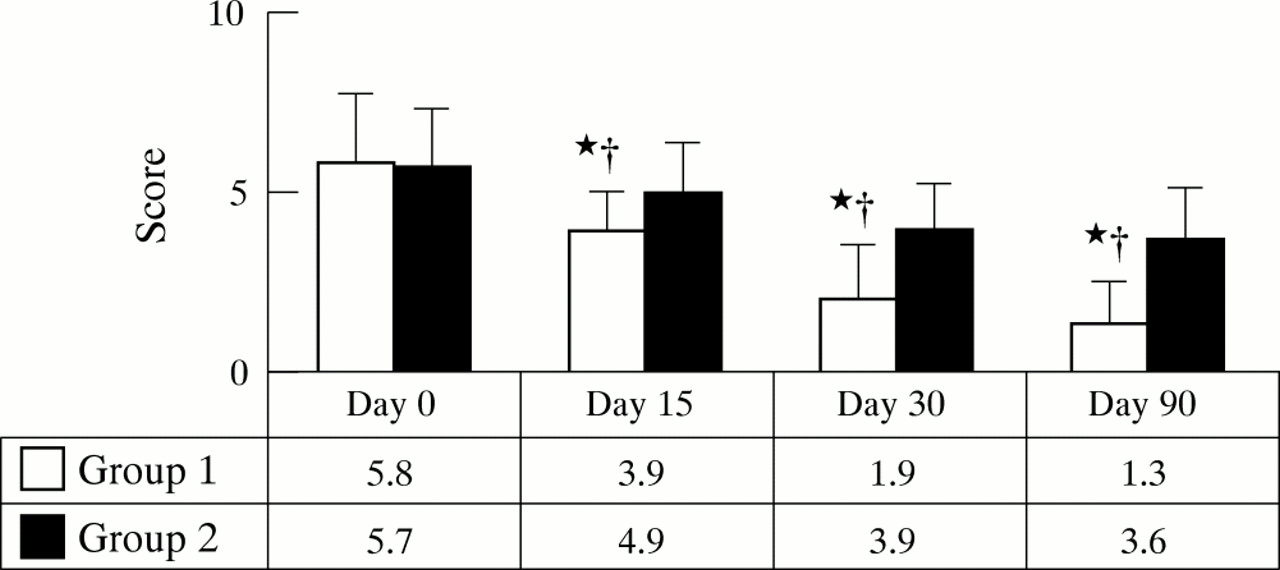
The global discomfort index for ocular symptoms showed in both groups a statistically significant improvement, starting from day 15 and lasting throughout the study. The improvement was more pronounced in group 1 at day 15 (p = 0.02 versus group 2). At days 30 and 90 there were no statistically significant differences between the two groups for the global discomfort index score. In both groups all symptoms, with the exception of photophobia, were statistically significantly reduced starting from day 15 and persisting up to the end of the study. Photophobia was statistically significantly reduced in both groups starting from day 30 (Table 2).
Scores for symptoms and global discomfort index (mean (SD)) of patients of both groups
Tests
Group 1
The ocular tests revealed a statistically significant improvement in BUT, fluorescein, and rose bengal score (p = 0.003, p = 0.000001, and p = 0.0004 respectively) starting from day 15 and persisting up to the end of the study.
Group 2
An improvement of BUT and fluorescein corneal staining was present starting from day 15 (p = 0.05 and p = 0.0001 respectively); also the rose bengal score became statistically significantly improved, starting from day 30, when compared to the baseline value (p=0.000001).
Comparison between the groups
It was possible to observe that, in group 1 patients, statistically significantly better results were achieved for rose bengal conjunctival stain starting from day 15 (p = 0.01) and for BUT and fluorescein corneal stain at day 90 (p = 0.05 and p = 0.0003 respectively) (Figs 1–3).

Results of the tear film break up time (mean (SD)) of patients in both groups. *p = 0.003 v time 0 starting from day 15 and lasting up to the end of the study; †p = 0.005 v time 0 starting from day 15 and lasting up to the end of the study; ‡p = 0.05 v group 2 patients at the same period of observation.

Results of fluorescein corneal stain (mean (SD)) of patients of both groups. *p = 0.000001 v time 0 starting from day 15 and lasting up to the end of the study; †p = 0.0002 v group 2 patients at the same period of observation.

Results of rose bengal conjunctival stain (mean (SD)) of patients of both groups. *p = 0.0004 v time 0 starting from day 15 and lasting up to the end of the study; †p = 0.01 v group 2 patients at the same period of observation.
No differences were shown, at any time, for Schirmer's I test either comparing the two groups or from time 0 in the same group (Fig 4).

Results of Schirmer's I test (mean (SD)) of patients of both groups. No statistically significant differences were observed at any time of the study from baseline and between the two groups of treatment.
Conjunctival impression cytology
Group 1
The conjunctival impression cytology showed a statistically significant improvement of the mean total score at day 15 (p = 0.02 versus baseline) and a further improvement at day 30 (p = 0.008 versus day 15); thereafter the amelioration was stable (p = 0.1 day 30 versus day 90) (Fig 5).

Total score of conjunctival impression cytology in the two groups of subjects. Mann-Whitney U test, *p<0.05 v group 2; †p<0.0001 versus baseline.
When the single parameters were taken into account, it was possible to observe at day 15 an improvement of the cell to cell junctions (p = 0.0002) and of nuclear chromatin (p = 0.04). At day 30 all the other parameters showed a statistically significant improvement versus baseline values (Fig 6).

Group 1: Conjunctival impression cytology parameters in group 1 patients, treated with hypotonic sodium hyaluronate. *p<0.05 versus baseline; †p<0.05 versus group 2. Group 2: Conjunctival impression cytology parameters in group 2 patients, treated with isotonic sodium hyaluronate. *p<0.05 versus baseline. Mann-Whitney U test for statistical analysis.
When considering the class of cytology it was possible to observe a statistically significant improvement starting from day 15 (p = 0.002), improving at day 30 (p = 0.05 versus day 15), and remaining unchanged at day 90 (Table 3).
Prevalence of the classes of cytology in the two groups of subjects
Group 2
An improvement of the mean total score was demonstrated starting from day 30 (p = 0.000005 versus baseline values) and lasting, without statistically significant changes, up to day 90 (Fig 5).
All the parameters studied, taken into account singularly, did not show at day 15 any statistically significant change compared to baseline features. A statistically significant improvement, versus baseline values, was observed at day 30 for the parameters: specimen cellularity (p = 0.000002), cell to cell junction (p = 0.0002), goblet cells distribution (p = 0.04), and presence of inflammatory cells (p = 0.01) (Fig 6). No statistically significant improvements were observed for the other parameters from baseline values for all the study period. The cytological classes demonstrated a statistically significant improvement starting from day 30 and persisting at day 90.
Comparison between the groups
It was possible to observe a statistically significant difference for the total score starting from day 15 and lasting throughout the study. The analysis of the single parameters showed no differences at day 15, while at day 30 group 1 values were statistically significantly better for nucleus/cytoplasm ratio (p = 0.02), chromatin pattern (p = 0.009), and goblet cells distribution (p = 0.0001). Comparing the cytological classes of the two groups, group 1 showed statistically significant better results starting from day 15 (p = 0.002) and persisting up to day 90 (p = 0.02).
Pictures representing the conjunctival impression cytology specimens in the two groups are shown in Figure 7.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Impression cytology specimen at time 0. The cells appear enlarged with a reduced nucleus/cytoplasm ratio and pyknotic nuclei. The cell to cell junctions are loosened so that cells appear isolated (PAS-Papanicolaou, ×360). (B) Time 0 specimen. It possible to observe isolated, enlarged cells with evident nuclear pyknosis. The nuclei are encircled by a perinuclear halo; it is also possible to see the presence of fragmented nuclei (PAS-Papanicolaou, ×360); (C) Day 30, group 1: the specimen shows a large sheet of cells which appear close to each other. Mucin spots (arrows), which indicate the presence of goblet cells, are shown. The nucleus/cytoplasm ratio is still reduced (PAS-Papanicolaou ×200). (D) Day 30, group 2: specimen with enlarged cells, mainly isolated but sometimes confluent in small clumps where the cellular borders are indistinct. The nucleus/cytoplasm ratio is reduced compared to normal (PAS-Papanicolaou, ×100). (E) Day 90, group 1: a large, multilayered sheet of cells where several goblet cells and many mucin spots can be observed (PAS-Papanicolaou, ×320). (F) Day 90 group 2 specimen, large sheet of cells with undefined borders; together with cells with normal nucleus/cytoplasm ratio, there are cells with reduced nucleus cytoplasm ratio (*). A goblet cell can be observed (arrow) (PAS-Papanicolaou, ×320).
DISCUSSION
Tear hyperosmolarity was indicated as the primary causative mechanism leading to discomfort, ocular surface damage, and inflammation.13,14,16,24,25 The eye drops used in the present study are commercially available, unpreserved eye drops, currently used for the treatment of dry eye and characterised by a same molecular weight of the hyaluronate molecule but a different osmolarity.
Sodium hyaluronate is a natural polymer and it was shown that its concentration increases in response to ocular damage and during corneal wound healing.26
It was recently demonstrated that a hyaluronate receptor, CD44, is expressed in corneal and conjunctival cells27,28 and that its activation promotes the interaction with cytoskeletal proteins,29 suggesting a role for hyaluronate in cell adhesion and motility.
Hyaluronate promotes, in vitro, cell migration and can stabilise the ocular surface epithelial barrier30,31 suggesting that it may be directly involved in the process of epithelial repair by means of the activation of the CD44.
It was also proposed that hyaluronate may have a role in controlling the localised inflammation often present in patients with keratoconjuctivitis sicca.32 Interestingly, it has been recently reported that the expression of CD44 is increased in patients with moderate dry eye and superficial keratitis and that sodium hyaluronate given for a 2 month period is associated with a decreased expression of this adhesion molecule.28 So sodium hyaluronate might have a direct role in the control of ocular surface inflammation in dry eye patients.
A previous study,6 carried out on patients with a mild dry eye, did not show any difference in dry eye symptom relief between a hypotonic sodium hyaluronate solution of 215 mOsm/l compared with an isotonic sodium hyaluronate solution (305 mOsm/l). Furthermore, both treatments determined an improvement of signs of corneoconjunctival epithelial suffering. In the present study, carried out on Sjögren's syndrome patients with severe dry eye, it was possible to demonstrate that a hypotonic solution of sodium hyaluronate with an osmolarity of 150 mOsm/l, lower than that previously tested, is able to induce a statistically significant improvement of ocular surface conditions, demonstrated either by impression cytology or by vital staining such as fluorescein and rose bengal. This improvement was better than that induced by an iso-osmotic solution of sodium hyaluronate of similar molecular weight. Therefore, it appears that a lower osmolarity may be important to obtain a better therapeutic result in patients with highly compromised lacrimal gland secretion like Sjögren's syndrome patients with severe dry eye.
The efficacy of sodium hyaluronate in reducing the epithelial changes in the ocular surface, in patients with dry eye, was evaluated by Nelson33 following a treatment period of 8 weeks. That study showed that although sodium hyaluronate was able to improve rose bengal staining, it did not change the degree of squamous metaplasia. It was concluded that significant changes of conjunctival epithelium could take longer than 8 weeks of treatment.
In the present study impression cytology, studied with a scoring system which included seven different cytological parameters, was used as an indicator of conjunctival epithelial damage. We found an improvement of ocular surface features after treatment with both hypotonic and isotonic sodium hyaluronate but the hypotonic solution showed a quicker and better improvement in the conjunctival conditions. It is noticeable that the method used to score the impression cytology specimens allowed us to study analytically seven parameters so it was also possible to have, together with a global assessment of the specimens, an evaluation of the single aspects related to the epithelial conditions and to analytically differentiate the epithelial features following the different treatments.
Our results seem to give further support to the findings of Gilbard et al,17 which showed a significant positive correlation between tear film osmolarity and ocular surface damage demonstrated by rose bengal staining.
The impression cytology demonstrated that total score and cytological classes were always better in patients treated with the hypotonic solution, although starting from day 30 an improvement was also present in subjects treated with the isotonic solution.
The seven parameters used for the evaluation of conjunctival impression cytology can be divided in two categories: the former is related to the cellular features and includes cell to cell junction, nucleus/cytoplasm ratio, nuclear chromatin, and keratinisation; the latter is related to tissue parameters and includes specimen cellularity, goblet cells distribution, and presence of inflammatory cells.
In group 1 subjects an improvement in cellular parameters such as cell to cell junctions and nuclear chromatin was observed at day 15. The former indicates an amelioration of the junctional complexes between the epithelial cells, so that the cells which initially appeared isolated were clumped in sheets where it was not possible to distinguish the cellular borders; the latter showed, before treatment, signs of cellular activation, such as presence of nucleoli, or damage like unevenly dispersed chromatin with presence of nuclear “snakes”21; already after 15 days of treatment the chromatin pattern was nearly normal, being characterised by the presence of evenly dispersed chromatin. From day 30 onwards, all the other parameters showed a statistically significant improvement from baseline values.
In group 2 subjects, a statistically significant improvement of cell to cell junctions and specimen cellularity, goblet cell distribution, and presence of inflammatory cells was observed only from day 30. The amelioration of these four parameters was enough to maintain a statistically significant improvement of the mean cytological score if compared with baseline features.
The goblet cells distribution is modified in response to irritating stimuli that, in more advanced stages of damage, bring a dramatic reduction or the disappearance of goblet cells from the conjunctival surface, this being a sign of squamous metaplasia like that typical of the advanced dry eye. When the irritating stimuli on the conjunctiva are relieved, goblet cells tend to appear again on the conjunctival surface.21
It is noteworthy that both isotonic and hypotonic sodium hyaluronate were able to induce an amelioration of the cell to cell junctions, since this effect could be an indirect demonstration of the interaction of hyaluronate with its receptor CD44, whose activation plays a part in cell adhesion and motility.29
From the results of this study it is possible to assess that sodium hyaluronate represents a useful treatment for severe dry eye in Sjögren's syndrome patients. In particular, high concentrations of sodium hyaluronate were able to provide a quick reduction in ocular symptoms in these patients. The treatment with hypotonic sodium hyaluronate eye drops gives a statistically significantly better improvement in clinical and cytological signs of the disease, compared with isotonic sodium hyaluronate at the same concentration.
The use of hypotonic hyaluronate eye drops should be encouraged for the treatment of patients with severe dry eye, where an increased tear osmolarity could play a part in the pathogenesis of the ocular surface damage.
REFERENCES:
Footnotes
-
Source of support: none.
Linked Articles
- BJO at a glance