Article Text

Abstract
Aim: To retrospectively study 26 patients with squamous cell carcinoma (SCC) of the ocular surface to determine pathological and clinical characteristics of tumour associated with outcome.
Methods: Patients with conjunctival SCC from St Vincent's Hospital and the private ophthalmology practices of the authors were reviewed.
Results: Patents were usually male (77%), elderly (69% > 60 years of age), with most lesions (81%) occurring at the limbus. Seven patients (27%) suffered recurrent ocular surface squamous neoplasia (OSSN) within 4–15 months and two of these patients (8%) died of metastatic disease. Intraocular invasion was noted in three patients (11%), while corneal and/or scleral invasion was found in eight (30%). Orbital invasion was noted in four patients (15%). Six required orbital exenteration. Preoperative impression cytology of five patients with minimally invasive disease showed OSSN in four (80%). In situ carcinoma could not be differentiated from minimally invasive disease using impression cytology. Preoperative diagnosis of SCC was made in 35% of cases. Clinical accuracy was higher for larger lesions (>10 mm) and those with hyperkeratosis.
Conclusions: Conjunctival SCC occurs in sun damaged ocular surface, usually at the limbus in elderly men. Recurrence of OSSN is common with significantly increased risk for older patients, lesions of large diameter, high proliferation index (Ki-67 score), and positive surgical margins. Orbital exenteration may be required for control of local disease and death from metastatic disease occurs in a small percentage of patients.
- CIN, corneal intraepithelial neoplasia
- CIS, carcinoma in situ
- HPV, human papillomavirus
- MMC, mitomycin C
- OSSN, ocular surface squamous neoplasia
- SCC, squamous cell carcinoma
Statistics from Altmetric.com
- CIN, corneal intraepithelial neoplasia
- CIS, carcinoma in situ
- HPV, human papillomavirus
- MMC, mitomycin C
- OSSN, ocular surface squamous neoplasia
- SCC, squamous cell carcinoma
Worldwide, conjunctival squamous cell carcinoma (SCC) is an uncommon disease, the incidence of which varies geographically from 0.02 to 3.5 per 100 000.1 Even before the term ocular surface squamous neoplasia (OSSN) was introduced to encompass the spectrum of conjunctival and corneal intraepithelial neoplasia (CIN) and SCC,2 published series often included both intraepithelial and invasive squamous neoplasia.3
OSSN is commonly seen in Australia2,4–6 and we have collected a series of 26 cases of SCC of the conjunctiva and cornea over a 7 year period. There are several issues that we wished to investigate. It is difficult to distinguish dysplasia, carcinoma in situ (CIS), and SCC on clinical grounds alone. In Lee and Hirst's series of 288 patients with OSSN including 62 cases of SCC,4 the overall clinical accuracy was 33% and only 30% for the SCC group. Macroscopic patterns of SCC have been described as gelatinous, velvety or papilliform, leucoplakic,3,7 nodular and diffuse.8 We have tried to identify features that might improve the accuracy of clinical diagnosis.
In general, SCC of the conjunctiva is regarded as a low grade malignancy. Recurrence rates are generally higher for more severe grades of OSSN and are also related to adequacy of margins at initial excision.6 Predictive factors for prognosis within SCC other than delay in seeking medical attention have not clearly been identified.
Impression cytology is a useful method for confirming the diagnosis of OSSN, particularly in recurrent cases being considered for topical chemotherapy, such as mitomycin C (MMC). Although we have found a high degree of reliability in detecting dysplasia,9 it is not clear whether SCC can be readily differentiated from in situ disease on cytological grounds alone, and we attempted to identify specific markers of invasive disease.
MATERIALS AND METHODS
All cases diagnosed as squamous cell carcinoma of the conjunctiva or cornea from March 1994 to the end of December 2000 were obtained from the records of the Department of Anatomical Pathology, St Vincent's Hospital, which receives histopathology specimens from the Royal Victorian Eye and Ear Hospital. Clinical data were obtained from the medical histories of public hospital patients and from referring ophthalmologists for private patients.
Pathology
Sections of all cases were reviewed by one pathologist (PMcK).
Tumours were assessed in both initial biopsies and definitive exenteration, excisional biopsy or enucleation specimens for the following features: differentiation, keratinisation, associated CIN or CIS, completeness of excision, associated solar damage in stroma, shape of lesion, extent of local invasion, and intraocular or orbital invasion. Pathology records were searched to determine whether any impression cytology had been performed before excision.
A proliferation index using Ki-67 was performed by immunohistochemistry. The primary antibody was a polyclonal antibody to Ki-67 (Dako, Carpinteria, CA, USA) used at 1:50 dilution and incubated for 1 hour. Antigen retrieval was performed by heating sections to 95°C for 3 × 5 minutes in microwave in 0.01M citrate at pH 6.0. Detection was performed using streptavidin alkaline phosphatase (Silenus SAP) and fast red substrate (Sigma). The number of Ki-67 labelled nuclei in tumour cells was analysed quantitatively, per 500 cells.
Statistical analysis
Results were expressed as median (range) for continuous variables and as actual numbers or percentage for categorical variables. Categorical factors influencing recurrence were examined by Kaplan-Meier estimator and groups compared with the log rank test.10 Factors examined included age, sex, size of lesion, involved margins, differentiation, shape of lesion, Ki-67 score, invasion of sclera and/or cornea, invasion of orbit, intraocular invasion. Cox regression was used for continuous variables.11 A p <0.05 was significant. Data were analysed with stata version 7.1 (Stata Corporation, College Station, TX, USA). Multivariate analysis was not possible because of the small numbers in each group.
RESULTS
Clinical
Demographic data are listed in Table 1. There were 26 patients (77% males) with age range 32–94 years (median 69 years). All patients were white. Patient age ranges included 30–39, one; 40–49, three; 50–59, four; 60–69, six; 70–79, five; 80–89, five; 90–94, two; 69% of patients were aged >60 years. Lesions were present on the right in 12 and on the left in 14. Twenty three were nodular and three were diffuse involving the limbus circumferentially. Limbus was involved in 19, limbus and cornea in two, fornix in two, medial canthus in two, bulbar conjunctiva in one.
Conjunctival SSC – clinical and pathological data
Clinical appearance at presentation was documented in 25. A mass (Fig 1) was most commonly seen, in 20 patients, nine of whom also had irritation or redness. Two of the 20 patients with a mass also had altered or decreased vision. Three presented with irritation or redness. One patient with diffuse disease presented as recurrent conjunctivitis and one was incidental. The duration of symptoms was available in 20. One was <1 week; six were 1–6 weeks, five were 2–6 months; two were 12 months, and six were ≥2 years. One patient was asymptomatic and was noted on incidental examination for floaters. Size of the lesion was recorded in 22 with 11 ≤6 mm and 11 ≥10 mm.

Clinical photograph of patient 7 showing the nodular tumour with prominent vascularity at the limbus.
Preoperative clinical diagnosis was SCC in nine, CIN or OSSN in 13, melanoma in one, recurrent pterygium in one, pingueculum in one, inflammatory mass in one. In lesions over ≤10 mm, SCC was correctly diagnosed in 23%, OSSN in 92%, whereas for >10 mm, SCC was diagnosed in 67% and OSSN in 78%.
Two patients had a history of previous OSSN—one with three episodes of CIN or CIS in the contralateral eye and one with five episodes of recurrent SCC since 1990. Other ocular disease included pterygium in either eye in seven, pingueculum in four (one bilateral), one with ectropion in same eye, one with entropion in same eye, one with ocular cicatricial pemphigoid, and one with conjunctival concretions. None had a history of herpes simplex keratitis or contact lens wear. Data about complexion and eye colour were available for 21 patients. Twelve had fair skin, 10 with blue or green eyes and two with brown. The others were described as olive skinned. Six patients of 15 in whom specific history was available had had previous skin cancers. Smoking history was available in 11, of whom five were smokers.
Follow up
One patient was lost to follow up. Eight patients had ≤9 months of follow up, including one death postoperatively at 1 month following exenteration. The remaining 17 had follow ups for 11–64 months (median 26 months). There were four deaths, two unrelated to the conjunctival tumour, at 1 month and 15 months after treatment. Two patients died of their disease. One developed recurrent tumour in the orbit at 5 months following exenteration and death from cerebral metastases at 13 months. The other patient experienced five local recurrences since first diagnosis in 1990. She developed cervical lymph node metastases at 4 months after exenteration, parotid metastases at 16 months, and died 22 months after exenteration (64 months after first occurrence of SCC).
Recurrences of OSSN (three as SCC, three CIS or CIN, are OSSN on cytology) were seen in seven patients (two of whom died of disease, see above). The five local conjunctival recurrences occurred at 4, 9, 14, 14, and 15 months and were treated with excisional biopsy in three and topical MMC in two. Of the six patients with positive surgical margins, four had local recurrence.
Treatment
Ten patients underwent more than one surgical procedure. In six of these, the second operation was orbital exenteration and in one enucleation. Modes of treatment are listed in Table 1. This included excisional biopsy in 13, excision + cryotherapy in one; excision and sclerectomy or superficial keratectomy plus or minus cryotherapy in four; excision and strontium 90 plaque in one; enucleation in one; and exenteration in six. Exenteration was performed for control of local disease.
Pathology
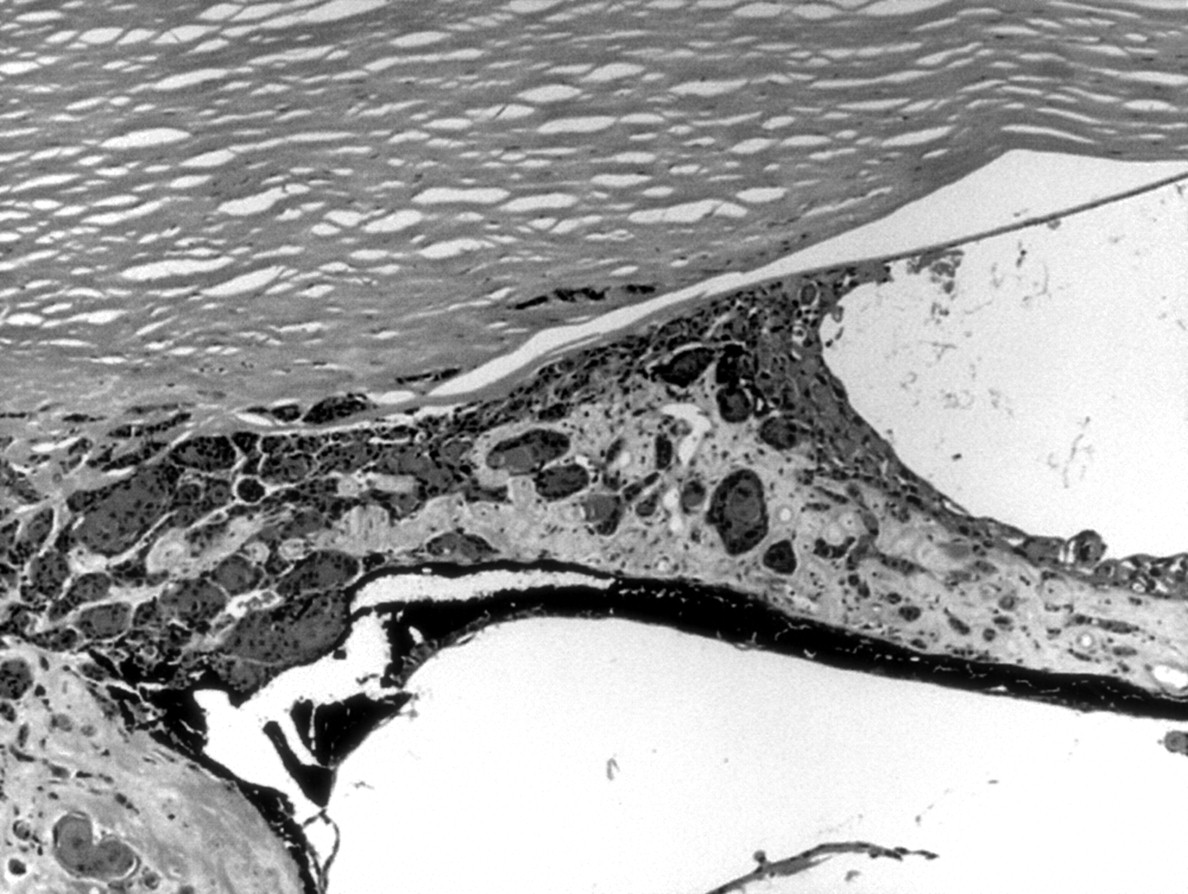
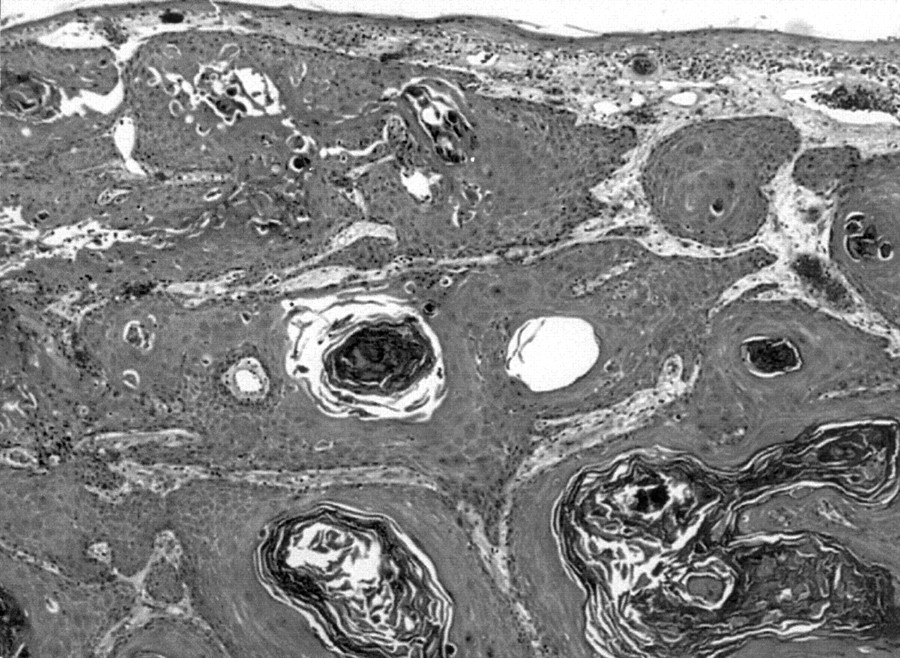
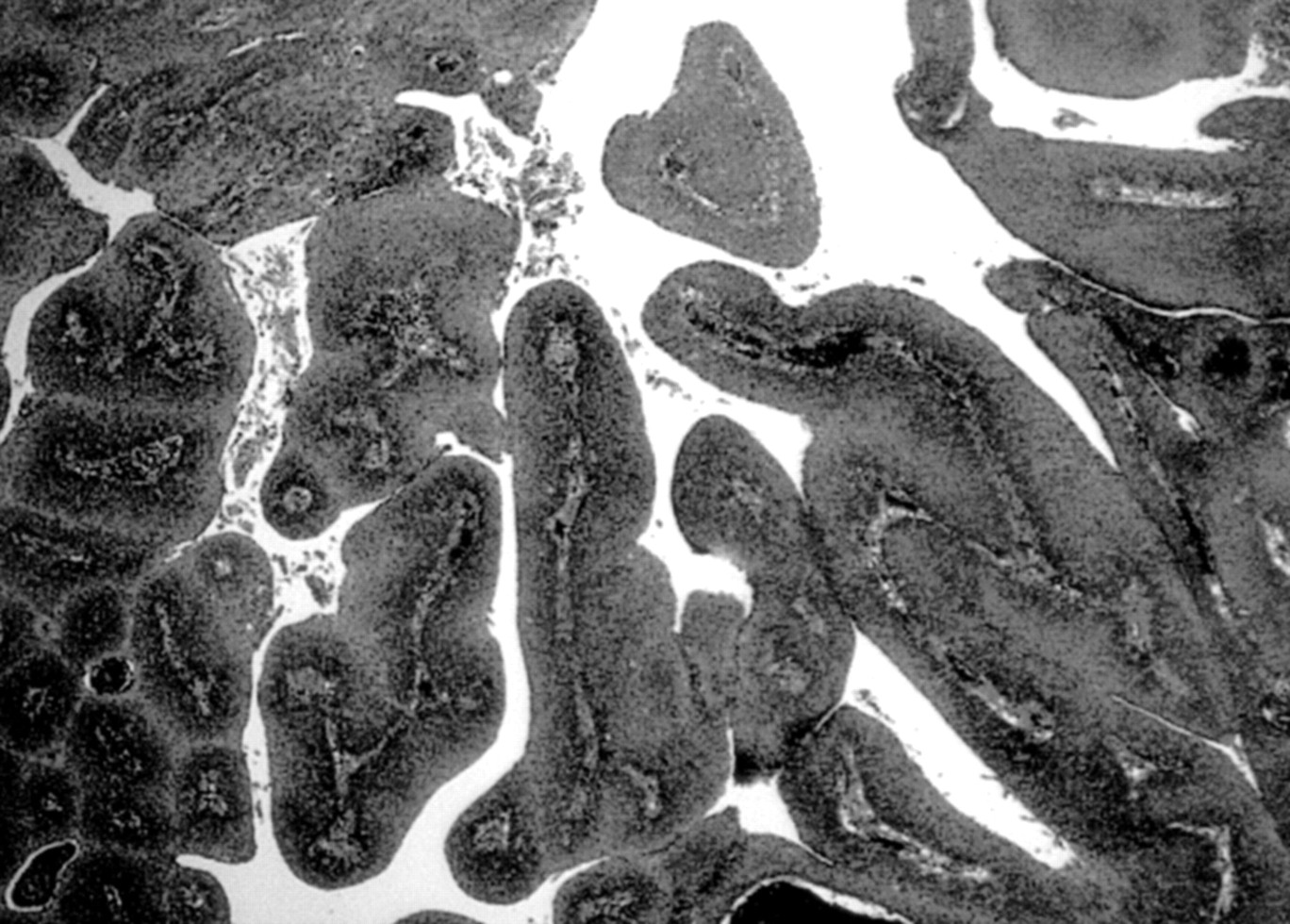
Three cases were well differentiated, 15 moderately, seven poorly to moderately, and one poorly. Although all lesions were keratinising, the degree varied from very minor focal in one to marked. In several cases, keratinisation was found only deep in the invasive tumour rather than on the surface. The invasive tumour appeared to arise in a field of CIS in seven, CIN in 16. One showed no associated CIN and in two the extent of invasive tumour precluded assessment. Solar damage, represented by basophilic, elastotic, or spheroidal degeneration in stromal collagen was seen in the conjunctiva in all cases. Shape of lesion was assessed on sections of tumour. Sixteen showed a thickened keratotic plaque, with invasion that varied from minimal to deep lobules (Fig 2). Minimal invasion, which was defined as focal microscopic tongues infiltrating stroma, was seen in 11 patients. Eight showed a predominantly endophytic lesion (Fig 3). Two were papillomatous or exophytic (Fig 4). .

Medium power photomicrograph of keratotic plaque type carcinoma, with microinvasion (arrows) showing thick layer of parakeratosis. Haematoxylin and eosin. Original magnification × 100

Low power view of endophytic type of carcinoma (patient 7) with lobules of invasive keratinising carcinoma in the stroma. Haematoxylin and eosin. Original magnification ×40.

Low power view of papillomatous type of squamous cell carcinoma (patient 23). Haematoxylin and eosin. Original magnification ×40.
Excision was incomplete for SCC in five patients and in one case for CIS, after the final procedure. Sclera was invaded in eight cases (two with sclerectomies, one enucleation, and five exenterations). Corneal invasion was seen in six (one enucleation, four exenterations, one keratectomy). Invasion of anterior chamber angle, trabecular meshwork, and iris (Fig 5) were noted in two and ciliary body invasion in three.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Medium power view of carcinoma infiltrating iris, posterior corneal stroma, and filling the anterior chamber angle. Haematoxylin and eosin. Original magnification ×100.
Eyelid infiltration was seen in two exenterations. Orbital invasion was noted in four exenterations.
Ki-67 count was performed in 18 cases with counts ranging from 2% to 29% with a median of 10% (Table 1). In eight of the cases with microinvasion, no residual invasive tumour was found on resectioning the blocks for immunocytochemistry for Ki-67.
Impression cytology
Five patients had preoperative impression cytology performed. All five had minimally invasive carcinoma and cytological diagnosis was positive for dysplasia in four (80%), with suspicion of invasive tumour in one of these. The negative case showed squamous metaplasia.
Statistical analysis
With only two deaths from disease, we were unable to predict factors associated with mortality. Factors affecting recurrence were determined by survival analysis based on the length of follow up and presence of recurrent disease. Significant factors included positive surgical margins (p = 0.028); size (both actual number and divided on a cutoff point of 10 mm) (p = 0. 049); Ki67 score (p = 0.047); and increased age (p = 0.0028). Insignificant factors included shape of lesion, differentiation, invasion of orbit, cornea and/or sclera, intraocular extension, and sex.
DISCUSSION
Our series confirms that SCC of the conjunctiva is a not uncommon lesion in Victoria with 26 cases recorded at one institution in a 7 year period. Like other series,2,4 we found that the tumour occurred predominantly in elderly males (77%), with most lesions involving the limbus (81%). All patients were white with none in the Aboriginal population. Reports from Brisbane, Queensland, which has a subtropical climate reveal that SCC occurs in a younger population with only 50% of patients older than 60 years compared with 69% of our series.4 Histological evidence of solar injury, which is recognised as a major risk factor for conjunctival SCC, was found in all of our cases, compared with only 50% found by Tabrizi and colleagues in a similar Australian population.5 Conjunctival SCC has also been associated with human papillomavirus (HPV) infection, especially genotype 16.5,12 As a previous study of a similar group of patients from the same institution, but from an earlier period (1980–92) demonstrated an incidence of 57% of HPV, including genotypes 6/11, 16, and 18 in conjunctival SCC,5 we did not repeat these investigations in our cohort.
Seventy per cent of our patients presented with a mass or growth, similar to the findings of Erie et al (77%),2 but in contrast with 28% in a large series from Queensland.4 Duration of symptoms ranged from days to years with a median of 3–4 months. Specific clinical preoperative diagnosis of SCC was only made in 35% of cases, similar to figures of 30%4 and 32%2 previously reported. However, a preoperative diagnosis of OSSN was made in 85% of our patients. For larger lesions measuring >10 mm diameter in our series, SCC was suspected clinically in 67% of cases. Although accuracy of preoperative diagnosis is high for in situ OSSN (CIN/CIS) with reported figures of 86%6 and 83%,2 reported accuracy is lower for invasive disease.
Despite the relatively short clinical follow up in about one third of our patients, seven patients (27%) developed recurrences of OSSN (including SCC, CIS, and CIN) at periods of 4–15 months. Significant predictors for recurrence in our series were size of the lesion, positive surgical margins, elevated proliferation index measured by Ki-67 score, and increased age. Previous studies have indicated that recurrence is usually a result of inadequate surgical margins.1 Of our six cases with involved surgical margins, four recurred as SCC or CIS. Immunostaining with antibody to Ki-67, which is a nuclear antigen expressed in proliferating cells, allows evaluation of the growth fraction of normal and neoplastic cells.13 Ki-67 scores have been found to be a significant predictor of clinical behaviour for a number of tumours,14,15 but not in others.16 Some laboratories routinely measure the proliferation index for certain tumours such as meningiomas as adjunctive prognostic information.
Two of our patients with recurrent SCC developed and died of metastatic disease following orbital exenteration. Although conjunctival SCC is regarded as a low grade malignancy, two of our 26 patients (8%) died of their disease. This is higher than previously reported figures of 4.5%,2 4%,17 and 0%.18 The presence of metastases has been said not to equate with a poor outcome, as only two of the four patients with metastases (50%) in two published series with a total of 49 cases2,17 were reported to have died of their disease. In another series of 10 patients with metastatic disease, only one death was reported with a mean follow up of 18 months.19 Both of our patients who died of their disease had poorly differentiated tumour, the largest tumours in the series (25 and 24 mm), orbital involvement at the time of exenteration and high proliferation index.
Although intraocular invasion has been reported to be rare in conjunctival SCC, with figures of 2–8% of cases,2,3,17,20 we found this in three patients (11%), which is similar to the incidence of 13% noted in another recent series.18 Corneal and/or scleral invasion was seen in eight (30%), including all three with intraocular infiltration. Orbital invasion was noted in four patients (15%), similar to other series.3,17,18,21 Orbital exenteration was required in all for control of local disease. However, infiltration of orbit, cornea and/or sclera, or intraocular structures was not associated with a significantly increased risk of recurrence. Only 11 (42%) of our cases showed minimal microscopic invasion of the stroma compared with 80% of the Mayo Clinic series.2
We have previously reported on the use of impression cytology using the Biopore membrane for the diagnosis of OSSN,9 where 80% accuracy can be achieved for dysplasia (CIN). To date, we have not identified cytological features that reliably differentiate carcinoma in situ (CIS) from invasive carcinoma. All five patients with preoperative impression cytology in this current study had minimally invasive disease on histology and 80% accuracy for OSSN on cytological examination. In the uterine cervix, where a parallel is drawn between the transformation zone at the squamocolumnar junction and the limbus, where most dysplasias/carcinomas arise, the presence of a tumour diathesis (necrotic debris and blood) is suggestive of an invasive lesion. With impression cytology, which only samples the surface layers of conjunctival epithelium, such a diathesis is not generally seen. Midena and colleagues, who report the use of smears from conjunctival scrapings, claim to be able to diagnose SCC by presence of a dirty necrotic background.22 Not all SCC develop on a background of CIS, which shows sheets of highly atypical epithelial cells on impression cytology. About 60% of our patients had histological CIN or partial thickness epithelial atypia adjacent to the invasive disease, which would not necessarily yield sheets of atypical cells if sampled by impression cytology. Endophytic lesions and orbital invasion cannot be identified with impression cytology, limiting its use as a diagnostic aid.
The macroscopic types of SCC include most commonly (62%) a thickened keratotic plaque with invasion that ranges from minimal to large lobules; an endophytic lesion in 31% and least commonly a papillomatous lesion. The keratotic plaque form was recognised preoperatively as OSSN in almost all cases (94%), with SCC suspected in 31%. Both papillomatous lesions were correctly identified as SCC, whereas for the endophytic group, which may or may not show surface hyperkeratosis, OSSN was only suspected in about 63% of patients.
SCC of the conjunctiva is part of the spectrum of OSSN incorporating CIN, CIS, and invasive tumour. Although the clinical diagnosis of in situ disease is high (86%), invasive carcinoma is much less often recognised (35%). Larger lesions and those with hyperkeratosis are more likely to be correctly diagnosed preoperatively. Impression cytology does not, in our hands, reliably distinguish in situ from minimally invasive disease, and therefore has limitations in the accurate diagnosis of SCC. Proliferation index using Ki-67 scoring varies considerably for SCC and offers useful prognostic information regarding risk of recurrence.
Acknowledgments
The authors would like to thank the following ophthalmologists for their help with clinical data and follow up: Drs Grant Snibson, John McKenzie, Laurie Sullivan, John Manolopoulos, Michael Haybittel, S Heery, G Koniuszko, and S Wangspa. Dr McKelvie would like to thank Dr Graham Mason of Dorevitch Pathology and Dr Ruth Storey of NorthWest Pathology, Burnie, for allowing access to original histology and blocks in three cases.
References
Linked Articles
- BJO at a glance