Article Text

Abstract
Aims: To investigate the current referral pattern and delays in treatment of patients with primary uveal melanoma.
Methods: 184 consecutive Finnish patients with uveal melanoma diagnosed between July 1994 and June 1999 were eligible, and 159 were enrolled (inclusion rate, 86%). Their mean age was 60 years (range 14–87). The dates of visits to dispensing optician, physician, ophthalmologist and ocular oncologist, the presence of symptoms, and reason for consultation were determined by structured telephone interview. Time intervals to treatment planning and treatment were calculated.
Results: 139 patients (87%) had symptoms at presentation and 44 patients (28%) had been seen by an ophthalmologist less than 2 years previously. The median height of the tumour was 6 mm (range, 1.0–17.0) and its largest basal diameter 11 mm (range 2.5–22.0) at diagnosis. Melanoma developed from a previously detected presumed naevus in 13 patients (8%). When the first contact was a dispensing optician (15%) the median time to treatment planning was 22 days (range 1–1156). When a physician other than an ophthalmologist (19%) was contacted the delay was 68 days (range 0–1283) and when an ophthalmologist (65%) was seen it was 34 days (range 1–1426). These differences were not significant (p=0.32). The chance of being referred at first visit was 89%. Median time to treatment was not associated with symptoms (p=0.16) and tumour volume (p=0.29), but it was significantly different between patients who were and were not referred at first visit (140 days v 34 days; p<0.001) and between those treated by ruthenium and iodine brachytherapy (59 days v 33 days; p=0.009).
Conclusions: Analysis of delays in management indicates that earlier treatment could be achieved if dilated fundus examinations were performed without exceptions, all suspicious naevi were referred for a second opinion, and if the patients with melanoma were referred to the ocular oncology service concurrently with staging examinations done at the regional hospital.
- uveal melanoma
- choroidal naevus
Statistics from Altmetric.com
Malignant melanoma of the uvea causes clinical metastases to one half of patients within 10 years.1 It is often a slowly growing, early metastasising cancer. A logical way to improve the survival of cancer patients is to diagnose their tumour earlier to decrease the chance for metastasis. The potential effect of early diagnosis and treatment of this tumour should not be disregarded, especially as they might also allow better preservation of vision in eyes that are treated with conservative methods.2–4 Because the incidence of uveal melanoma is low, it is not feasible to mass screen even the age groups which would be at highest risk of developing it.5 Moreover, a comprehensive ophthalmological examination would be needed instead of a simple screening test. Consequently, mainly patients with suspicious choroidal naevi and congenital melanocytosis are currently reviewed with varying intervals.6,7
How patients are exactly diagnosed as having primary uveal melanoma and how they are referred to treatment is known in detail only for the United Kingdom, which has a special type of healthcare system based on many ophthalmic opticians and general practitioners and relatively few ophthalmologists (Table 1).2,8 In Finland, ophthalmic opticians and optometrists are not licensed, and patients contact an ophthalmologist, a family physician, or a dispensing optician instead (Table 1). The dispensing opticians, who do not do dilated fundus examinations, are obliged to refer their customer to a physician if they suspect disease. When the diagnosis of an intraocular tumour is made or suspected, staging examinations are carried out usually at regional hospitals and the patient is thereafter referred as a rule to a single national ocular oncology service.
The number of practising dispensing opticians, optometrists, general practitioners, and ophthalmologists per 100 000 inhabitants in Finland and the United Kingdom
In Finland, ruthenium brachytherapy is used for melanomas less than 6 mm in height, and those that are over 6 mm in height are usually treated with iodine plaques. Enucleation is done routinely when conservative therapy is not technically feasible. The system is similar in the other Nordic countries, especially in Sweden and Denmark.
We evaluated in detail the current referral pattern and identified delays in referral of uveal melanoma in the above context.
PATIENTS AND METHODS
Eligibility criteria and enrolment
All consecutive patients with primary malignant melanoma of the uvea diagnosed between July 1994 and June 1999 were identified from the registry of Helsinki University Central Hospital, which is a tertiary referral unit that manages over 90% of uveal melanoma patients in Finland. Of the 184 eligible patients, 10 (5%) had died for various reasons. The 174 patients alive were sent a letter alerting them to an upcoming interview, but 15 (8%) of them could not be contacted. All 159 patients contacted consented to the study and underwent a structured telephone interview by one investigator not involved in their treatment (inclusion rate, 86%). Their mean age at the time of diagnosis of primary uveal melanoma was 60 years (median 61; range 14–87); 75 were male and 84 were female. The study was approved by the institutional review board and followed tenets of the Helsinki Declaration.
Data collection
The dates of all visits to a dispensing optician, a physician other than an ophthalmologist (designated non-ophthalmologist for the purpose of this study), an ophthalmologist, and the ocular oncology service were determined by structured interview and verified, whenever possible, from patient charts, bills, and other legal documents.
The reason for each appointment was identified. Whenever the appointment was made to get spectacles it was determined whether the reason was change in vision (coded symptomatic) or strictly a wish to repair spectacles or change them for cosmetic reasons (coded asymptomatic).
The presence of nine categories of symptoms was systematically questioned: blurred vision, visual field defect, photopsia, irritation, floaters, metamorphopsia, redness, change in the appearance of the eye, and other symptoms specified by the patient.
The date of diagnosis, the tumour height and diameter, and the date and type of treatment were obtained from patient charts. Tumour dimensions were based on ultrasonography examinations at the ocular oncology service. Whenever visible, tumour height was measured from the inner surface of the sclera. Best clinical estimates for tumour dimensions taken from notes and sketches in patient chart were used if ultrasonographic measurements and photographs were not available. If the patient had been reviewed because of a presumed intraocular naevus, the charts were obtained from the practitioner in question and the presence of the following high risk characteristics was recorded: presence of symptoms and subretinal fluid, tumour thickness greater than 2 mm, orange lipofuscin pigment over the tumour, tumour margin touching the optic disc, larger basal diameter, and absence of drusen and retinal pigment epithelium change adjacent to tumour.9–11
The volume (V) of the tumour was estimated from an equation based on ellipsoidal forms, V = π/6 × (H × LBD × PBD), where H is the height of the tumour, LBD is the largest basal diameter, and PBD is the diameter perpendicular to LBD.12,13
Statistical analysis
The distributions of continuous data that were not normally distributed were compared with the Mann-Whitney U test and Kruskal-Wallis test, and their interrelation was analysed with Spearman's rank correlation. Pearson's χ2 test was used to compare unordered contingency tables. To compare delay times, cumulative frequency distribution plots for time from initial presentation of the tumour to treatment planning and to treatment at the ocular oncology service were also drawn from which it can be determined by which time any specified proportion of patients were cared for. The tumours were categorised as: small if they were less than 10.5 mm wide in their LBD and less than 2.5 mm in height; medium if LBD was between 10.5 mm and 15.4 mm or the height was between 2.5 mm and 8.4 mm; and large if LBD or height exceeded these figures.3
RESULTS
Symptoms
By structured interview 139 patients (87%; 95% CI 81 to 92) had symptoms before their first contact with health care, most commonly blurred vision and a visual field defect (Table 2). The symptoms appeared a median of 84 days previously (range 0 days to 5 years 11 months), and 119 patients (86%; 95% CI 79 to 91) sought help because of the symptoms. The other 20 patients (13%; 95% CI 8 to 19) made or kept an appointment made for other reasons, most commonly to change spectacles and to attend a scheduled follow up examination for a presumed naevus (Table 3).
Symptoms before diagnosis of primary malignant melanoma of the uvea in 159 patients
The reason for making appointment for 40 patients with primary malignant melanoma of the uvea who did not seek help because of symptoms
Uveal melanoma was diagnosed in 20 entirely asymptomatic patients (13%; 95% CI 8 to 19) during an appointment made for various reasons, again most often to change spectacles and to attend a scheduled naevus follow up examination (Table 3).
Initial presentation
The first healthcare professional contacted was a dispensing optician in 24 cases (15%; 95% CI 10 to 22), a non-ophthalmologist in 30 cases (19%; 95% CI 13 to 26), and an ophthalmologist in 104 cases (65%; 95% CI 58 to 73). A school nurse referred one patient (1%; 95% CI 0 to 3) to an ophthalmologist. Before the first visit related to the tumour, 39 patients (25%; 95% CI 18 to 32) had seen a dispensing optician a median of 24 months earlier (range 3 weeks to 15 years 11 months), and 104 patients (65%; 95% CI 58 to 73) had seen an ophthalmologist for unrelated reasons a median of 26 months previously (range 3 months to 19 years 11 months) (Fig 1).

Cumulative frequency plot of the time span between the last visit (unrelated to the tumour) to an ophthalmologist and to a dispensing optician and initial presentation with the tumour.
Diagnosis and referral
The diagnosis made during the first visit was mentioned in 111 of the 159 (70%) patient charts. A tumour was mentioned in 77 (69%) of them.
The dispensing optician referred 21 of 24 patients (88%; 95% CI 68 to 97) to a private ophthalmologist (two of them contacted a family physician instead). Two patients were referred to a non-ophthalmologist (one contacted an ophthalmologist instead). The only patient who was not referred had seen floaters for 3 months and received a prescription for spectacles (when symptoms persisted he contacted an ophthalmologist).
The non-ophthalmologist referred 26 of 30 patients (87%) to an ophthalmologist. An intraocular tumour was mentioned in two referral letters. Of 25 patients who sought help because of tumour symptoms, four (16%) were not referred but were treated for presumed tension neck syndrome, conjunctivitis, blepharitis, and floaters interpreted to be a symptom of concurrent high blood pressure. All four contacted an ophthalmologist within 3 months (the patient with floaters saw a dispensing optician first and received a prescription for spectacles). Of the five patients who made contact for unrelated reasons, four had ocular symptoms, and one had tumour diagnosed when fundi were examined for diabetic retinopathy. All five were referred.
Of 104 patients seen first by an ophthalmologist, 23 (22%) were though to have findings typical of uveal melanoma, and 44 (42%) were diagnosed to have an unspecified intraocular tumour. A suspicious naevus was diagnosed in seven patients (7%) of whom three were referred and the rest scheduled for follow up. Thus, 74 patients (71%; 95% CI 61 to 80) were diagnosed as having a tumour during the first appointment. However, only retinal detachment was diagnosed in seven patients (7%) and one patient each was referred because of acute glaucoma, uveitis, cataract, vitreous haemorrhage, and an unidentified fundus lesion. In three of the latter, the tumour was not visible before the secondary problem had been treated. In 10 instances (10%), the reason for referral was not specified.
Of the other seven patients (7%) who were not referred, four were diagnosed to have a refractive error and received spectacles, and the reason for floaters and visual field defect was not identified in three patients. All made a new appointment (one saw a dispensing optician who referred him back to the ophthalmologist). During the second visit, four of them were diagnosed to have a tumour, one a retinal detachment, and one an unidentified fundus lesion. One tumour still remained undiagnosed and the patient was referred with headache and blurring of vision to a family physician, who suspected a tumour a year later.
Melanomas developing from naevi
Of the 159 patients, 13 (8%) developed a melanoma from a previously identified presumed naevus. A scheduled review led to diagnosis in nine of them (69%; Table 4), the others were not followed up systematically. The median follow up time before diagnosis of uveal melanoma was 3 years (range 1 to 35 years) and the review interval 12 months (range 3 months to 2 years).
Nine presumed naevi that were regularly reviewed and later evolved into a primary malignant melanoma
In eight of the 13 (62%) eyes, symptoms had developed since last review. Of 11 choroidal naevi, 10 (91%) had at least one risk factor for growth. Seven naevi (36%) were associated with three to four of the eight known high risk characteristics for growth, three naevi with one to two characteristics, and one patient had no high risk characteristics: seven tumours did not have areas of adjacent retinal pigment epithelial changes, six had orange pigment, five had subretinal fluid, five patients had visual symptoms, tumour height was over 2 mm in three eyes, drusen were absent from three tumours, one tumour touched the optic disc, and the largest basal diameter was over 12 mm in one case.
The median LBD of the presumed naevus at first examination was 6.0 mm, height 1.0 mm, and volume 19 mm3. When uveal melanoma was diagnosed, the median LBD had increased by 1.7 times to 10 mm, the height by 3.5 times to 3.5 mm, and the volume by 7.5 times to 142 mm3.
Number of visits and delay times
The median number of visits before treatment was four (range, 2–23) including a treatment planning visit to the ocular oncology service. When an ophthalmologist was the first contact, the median number of visits was three (range 2–23), typically including a visit to a regional hospital to rule out other malignancies and metastases. When it was an optician or a non-ophthalmologist, the median number of visits was four (range 3–11), typically including a visit to an ophthalmologist who referred the patient to hospital.
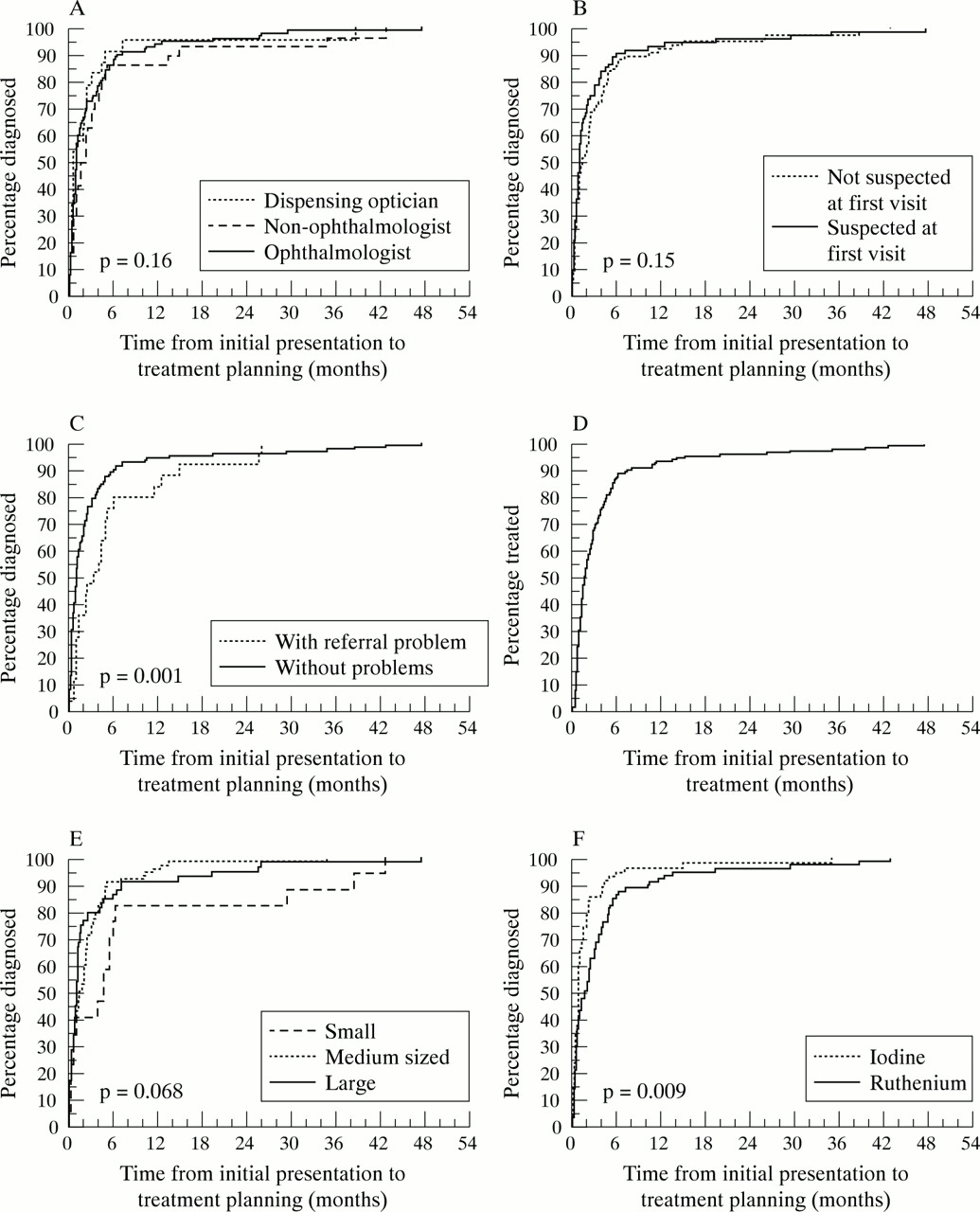
The median time from initial presentation to treatment planning was 35 days (range 0–1426). When the first contact was a dispensing optician the median was 22 days (range 1–1156), when a non-ophthalmologist was contacted it was 68 days (range 0–1283), and when an ophthalmologist was consulted, the median delay was 34 days (range 1–1426). The differences in delays were not statistically significant (Fig 2A, p = 0.16, Kruskal-Wallis test).

{kind=link}
{kind=link}
Cumulative frequency plots of time from the initial presentation to treatment planning in the national ocular oncology service according to (A) (Mann-Whitney U test) the healthcare professional seen (one patient referred by a school nurse is omitted), (B) whether or not the tumour was suspected at first visit, (C) whether or not misdiagnoses or administrative problems occurred in the referral process. Cumulative frequency plot of time from the initial presentation to treatment (D). Cumulative frequency plots of time from the initial presentation to treatment planning according to categorised tumour size (E) (Kruskal-Wallis test), and the type of brachytherapy (F) (Mann-Whitney U test).
Whether the tumour was suspected during the first visit or not did not statistically significantly affect the delay before treatment planning (Fig 2B; 77 patients v 82 patients, median, 34 day v 49 days, p = 0.15 Mann-Whitney U test). The 16 (10%; 95% CI 6 to 16) patients who were not referred after the first visit (one by an optician, four by a non-ophthalmologist, and 11 by an ophthalmologist) were subject to a statistically significant delay in treatment (median, 140 days v 34 days, p<0.001).
Of the 159 patients, 25 (16%; 95% CI 10 to 22) were identified to have been misdiagnosed or to have administrative problems related to their referral. The delay before treatment planning for these 25 patients was statistically significantly longer than that of patients who had not experienced such a problem (Fig 2C; median 101 days v 34 days, p = 0.001).
Tumour dimensions and treatment
The median time from initial presentation to the treatment was 57 days (mean 126 days; range 6–1435). Of the 159 patients, eight (5%) were treated within 2 weeks from the initial presentation and the delay was longer than 20 weeks in 33 (21%) instances (Fig 2D).
The median time from treatment planning to treatment was 11 days (mean 16 days; range 0–126). Of the 159 patients, 100 (63%) were treated within 2 weeks and 126 (79%) within 3 weeks. Delays less than 3 weeks were related to waiting for the appropriate plaque to be ready from previous treatment. Delays longer than 3 weeks occurred when an indeterminate tumour was first observed for growth, vitreous haemorrhage initially made the diagnosis uncertain, further investigations to rule out metastasis were needed, and when required by the patient because of intercurrent disease, personal reasons, or need for second opinion.
None of the patients had clinical metastases at diagnosis. The median height of the melanoma was 6.0 mm (mean 6.4 mm; range 1.0–17.0), LBD was 11.0 mm (mean 11.3 mm; range 2.5–22.0), and volume 286 mm3 (mean 484 mm3; range 5–3686). The presence of tumour symptoms (p = 0.16; Mann-Whitney U test) and tumour volume (r = −0.89; p = 0.29; Spearman's rank correlation) were not statistically associated with the delay but a tendency of large and medium sized melanomas being diagnosed earlier than small ones was present when compared according to categorised tumour sizes (Fig 2E, p= 0.068; Kruskal-Wallis test).
Brachytherapy with ruthenium and iodine plaques was given to 81 (51%) and 63 (40%) patients, respectively. The involved eye was enucleated from 11 (7%) patients and four tumours were treated with local resection. A statistically significant association was found between the delay and type of brachytherapy. The median delay was 59 days (range 4 days to 3 years 6 months) for patients who underwent ruthenium plaque therapy and 33 days (range 0 days to 2 years 10 months) for those who underwent iodine brachytherapy (Fig 2F; p = 0.009; Mann-Whitney U test).
DISCUSSION
This retrospective survey of referral to treatment of patients with primary uveal melanoma identified several differences compared with a previous prospective analysis conducted in the United Kingdom.2–8 Because of its retrospective nature, our study was liable to missing and erroneously recalled data. Checking the data against patient charts and other legal documents has minimised this problem. The number of patients was small, but this is compensated for by the fact that the present series was population based, consecutive, and had a high inclusion rate. We believe that the results reflect the current referral for uveal melanoma in Finland reasonably well.
In Finland, two thirds of patients with uveal melanoma seek help from an ophthalmologist regardless of whether they have symptoms or not. Their chance of being immediately referred and correctly diagnosed at first visit was 88% and 71%, respectively. One fifth consulted family practitioners and other non-ophthalmologists, and one sixth saw a dispensing optician. They had 88% and 87% chance of being immediately referred, respectively, and 13% of those referred by a non-ophthalmologist were diagnosed correctly. The dispensing opticians do not give diagnoses. In Britain, 59% of patients saw first an ophthalmic optician, and only 14% an ophthalmologist.8 It seemed that the choice of a healthcare professional was dictated by availability and personal preference rather than concern related to symptoms (Table 1). Uveal melanomas are rare and it is likely that the patients did not know that the symptoms might be serious.
Roughly one in 10 uveal melanomas in this population based study developed from a known presumed naevus. Most but not all had been regularly reviewed by ophthalmoscopy.
The proportion who had a previous naevus was roughly the same, three of 50 patients in the British study.2 This is likely to be an underestimate, because a third of our patients had not seen an ophthalmologist before and because naevi in the peripheral fundus may escape attention. Several high risk characteristics have been identified as a useful aid to predict growth of small choroidal melanocytic tumours—presence of symptoms and subretinal fluid, tumour thickness greater than 2 mm, orange lipofuscin pigment over the tumour, and tumour margin touching the optic disc.9,10 The Collaborative Ocular Melanoma Study Group reported three additional features associated with growth: larger basal diameter, absence of drusen, and absence of retinal pigment epithelial change adjacent to the tumour.11 It is of note that 10 of the 11 presumed naevi that developed a melanoma were initially associated with at least one of the eight known high risk characteristics for growth. In particular, eight had developed symptoms since last review.
Review of presumed naevi is ideally based on fundus photographs and, when the naevus is elevated, on ultrasonographic measurements. The smaller the naevus the more difficult it is to observe growth only by ophthalmoscopy, and this applies particularly to change in tumour height. Thus, the tumours in our study were on average almost twice as large by LBD at diagnosis of uveal melanoma than initially, but their median volume was seven times bigger. Earlier growth was thus probably missed or disregarded which emphasises the importance of referring small suspicious tumours for a second opinion at an early stage and of following them with photography and ultrasonography, especially as tumour doubling times suggest that micrometastasis may take place 1–5 years before diagnosis of primary tumour in two thirds of patients with metastases. 14 Patients with naevi should also be told to return immediately if any visual symptoms develop.
Of the 159 patients, 45 (28%) had seen an ophthalmologist for reasons unrelated to the tumour less than 2 years before the initial presentation. It is possible that an appropriate dilated fundus examination may not have been carried out in every instance.
One eighth (13%; 95% CI 8 to 19) of our patients was asymptomatic and the tumour was diagnosed during a routine visit. The proportion of asymptomatic patients was one third of that in the British studies, in which 30–45% of patients were asymptomatic.4,8 This difference suggests that ophthalmic opticians in United Kingdom who perform ophthalmoscopy may be better accessible than ophthalmologists in Finland. The British might also be better informed about the advantages of routine ocular check ups, or presence of symptoms may have been coded differently. Indeed, the mean age of the patients (59.7 v 60.6 years), mean LBD of the tumour (11.6 v 11.3 mm), and mean duration of symptoms before first contact (2.2 v 3.1 months) in the British and Finnish series, respectively, were comparable and do not suggest a systematic difference in accessibility to treatment.3,8 The larger mean tumour thickness of Finnish patients (4.9 v 6.4 mm) remains unexplained because both values were based on basically identical ultrasonographic measurements.
This British study identified avoidable delay in referral in 42% (95% CI 28 to 57) of 50 patients.2 Based on the same categorisation, 16% (95% CI 10 to 22) of our patients experienced a similar delay in referral. In Finland the specialist at the receiving unit decides the urgency of the referred patient based on the information in the letter. The British study speculated that reassurance that symptoms are not serious leads to late diagnosis,2 but Finnish patients usually searched rapidly for a new consultation when symptoms persisted.
It is alarming that an intraocular tumour apparently was missed by an ophthalmologist in 29% (95% CI 20 to 39) of patients during the first visit, even though most of them were nevertheless referred because of secondary effects of the tumour. The proportion was comparable in the British study, in which misdiagnosis occurred in four of 16 patients (25%; 95% CI 7 to 52) seen by an ophthalmologist.8 Misdiagnosis rate was 15% when patients presented first to an ophthalmic optician in the United Kingdom.4 Moreover, some of our patients had shortly before seen an ophthalmologist for unrelated reasons without the tumour being diagnosed. This seems to indicate a need for further education as regards signs and symptoms of intraocular tumours and emphasises the importance of dilated fundus examination by indirect ophthalmoscopy, which may not have been carried out in every instance.
In Britain, patients who were promptly referred were more likely to be treated with eye and vision conserving methods.2 In Finland, no such difference emerged partly because of much more frequent use of iodine plaque radiotherapy instead of enucleation for large tumours. However, an unexpected difference was noticed between the two modes of brachytherapy. Ruthenium brachytherapy, used for smaller melanomas, was paradoxically associated with longer delays than iodine brachytherapy, given to patients who have larger tumours. Even though we did not find statistically significant differences in delay according to tumour size this finding suggests that larger melanomas caused more symptoms and were easier to diagnose and were thus also treated faster.
Patients feel most distressed during the interval from suspicion of a tumour to eventual treatment after which the stress diminishes.15 One cause of delay in our study was the waiting time to imaging of the liver in regional hospitals which are financial gatekeepers as regards referral to the ocular oncology service. Waiting for special investigations also caused delay in Britain, where the most important delay was referral to an ophthalmologist via a general practitioner,3,8 also a financial gatekeeper.
We did not find difference in delays whether or not the patient was seen first by an ophthalmologist or other healthcare professional, and whether or not a tumour was immediately suspected. Considering that micrometastasis may take place between 1 and 5 years before diagnosis,14,16,17 a median delay of less than 4 months from the onset of symptoms to treatment may not always represent a serious hazard to life, but a shorter delay could potentially salvage more useful vision and perhaps prevent some metastases from developing. These findings also seem to indicate that an earlier diagnosis in several instances might be possible if routine dilated fundus examinations were performed without exception. Routine referral of patients with suspicious naevi for second opinion could also reduce delay in a subgroup of patients. The incapability of modern chemotherapy to notably improve prognosis after metastasis18,19 calls for efforts to help the immune system to fight micrometastasis at an early stage and to develop other adjuvant therapies to be used at the time of the treatment of the primary tumour.
Acknowledgments
Supported by grants from the Emil Aaltonen Foundation, the Eye and Tissue Bank Foundation, the Finnish Medical Foundation, and the Friends of The Blind.
No proprietary interest.
Presented in part in the European Vision and Eye Research (EVER) Meeting, 4–7 October 2000, Palma de Mallorca, Spain.