Article Text

Abstract
Aims: To analyse the visual and angiographic results of photodynamic therapy (PDT) with verteporfin in highly myopic patients with subfoveal choroidal neovascularisation (CNV).
Methods: PDT was performed on highly myopic patients with subfoveal CNV. The patient population was divided into two groups according to age at onset of CNV (group 1 aged ≤ 55 and group 2 aged >55 years old). Best corrected visual acuity (BCVA) and angiographic findings were considered.
Results: At the end of follow up group 2 had worse BCVA than group 1. 76% of patients in both groups showed a complete closure of CNV at the end of follow up.
Conclusion: Visual prognosis of myopic CNV treated by PDT is influenced by age at onset.
- myopia
- choroidal neovascularisation
- photodynamic therapy
Statistics from Altmetric.com
High myopia is a major cause of legal blindness in many developed countries.1 It affects approximately 2% of general population2 and 27–33%3 of myopic eyes. It is defined by an elongation of the anterioposterior axis of the eyeball and is commonly associated with a spherical equivalent higher than 26 mm. Frequently degenerative changes in the sclera, choroid, and retina also appear such as posterior staphyloma, chorioretinal atrophy, ruptures in Bruch’s membrane (so called lacquer cracks), subretinal haemorrhages, and choroidal neovascularisation (CNV).4 Myopic maculopathy, consisting of chorioretinal atrophy and macular CNV, is the most common cause of vision loss in highly myopic patients.5 It is often bilateral and irreversible, affecting individuals during their productive years, thus causing an average of 17 years of legal blindness.6
Different therapeutic approaches have been tried on myopic maculopathy, starting from thermal laser photocoagulation,7,8 radiotherapy,9 and different surgical procedures,10–14 to more recently photodynamic therapy (PDT) following the good results achieved by the VIP 1 study.15
In this study we investigated the visual and angiographic outcome of highly myopic patients treated by verteporfin PDT, 1 year after treatment was started, and its relation with age and chorioretinal atrophy.
PATIENTS AND METHODS
Thirty two consecutive patients (33 eyes) with high myopia and subfoveal CNV were recruited from the retina unit at the Instituto Oftalmológico de Alicante (Spain) from June 2000 to February 2001. Informed consent was obtained from all patients.
Inclusion criteria for this study were: (1) refractive error of −6 dioptres (D) or more, and/or fundus changes characteristic of pathological myopia such as chorioretinal atrophy, lacquer cracks, posterior staphyloma, and atrophic patches; (2) presentation within 6 months of loss of visual acuity; (3) fluorescein angiographic documentation of CNV; (4) no previous macular laser; (5) no intraocular surgery in the previous 2 months; (6) best corrected visual acuity (BCVA) less than 20/40; (7) no other ocular disorders, such as angioid streaks or age related macular degeneration (ARMD) that might cause subfoveal CNV. Pregnant or nursing patients, and patients with diabetic retinopathy, or other causes of visual loss not related to myopic maculopathy were excluded. Patients who were not amenable to undergo PDT were also excluded from the study.
The 32 patients were divided into two groups according to their age at the initial visit: group 1 (≤ 55 years old) and group 2 (>55 years old). The initial evaluation included refraction, BCVA performed with the ETDRS charts (Lighthouse International, NY, USA), slit lamp examination, tonometry, fundus examination using indirect ophthalmoscopy and fluorescein angiography, and it was repeated on a 3 months schedule.
Eyes were also classified according to the degree of chorioretinal atrophy following Avila’s classification5 in M1 (choroidal pallor, tessellation and posterior staphyloma, with no ophthalmoscopic evidence of lacquer cracks), M2 (macular lacquer cracks), M3 (macular atrophic patches), and M4 (large geographic areas of chorioretinal atrophy in the macula).
Verteporfin (Visudyne, Novartis AG, Bülach, Switzerland) PDT was performed as described previously.15 Patients received further treatments with PDT only if CNV activity was angiographically demonstrated, and it was performed not earlier than 3 months after the last session, and not later than 1 week after the last angiography.
Response to PDT was classified in three categories depending on the fluorescein angiographic results: “good,” if the CNV was completely closed after PDT; “partial,” if the area of CNV was smaller than previous to PDT; and “lack of response,” if the area of CNV was equal or bigger than previous. The presence of a fibrotic scar at the end of follow up was also considered.
The number of PDT sessions needed for the closure of the CNV was also considered, as well as the intake of oral antioxidants.
RESULTS
We have followed 33 eyes from 32 highly myopic patients with subfoveal CNV treated with verteporfin PDT. Two patients (two eyes), one from each group, were lost to follow up after 6 months, and 31 eyes (11 right, 20 left) from 30 patients, (10 male and 20 female) completed 1 year follow up.
Patients who completed follow up were divided into two groups according to their age: group 1 with patients aged ≤ 55 years old (18 eyes) and group 2 with patients aged >55 years old (13 eyes). Mean age in the whole group of patients was 54.9 (SD 14.0) years; it was 44.9 (8.1) for group 1 and 68.7 (6.4) years for group 2.
Mean spherical equivalent for the whole group was −14.1 (SD 5.3) D (−14.8 (5.0) D for group 1 and −13.0 (5.8) D for group 2).
Mean CNV diameter at baseline was 1796.7 (771.2) μm for group 1 and 1547.8 (807.0) μm for group 2. CNV diameter decreased after treatment in both groups, as described in Table 1.
Evolution of choroidal neovascularisation (CNV) diameter (μm) after treatment with photodynamic therapy
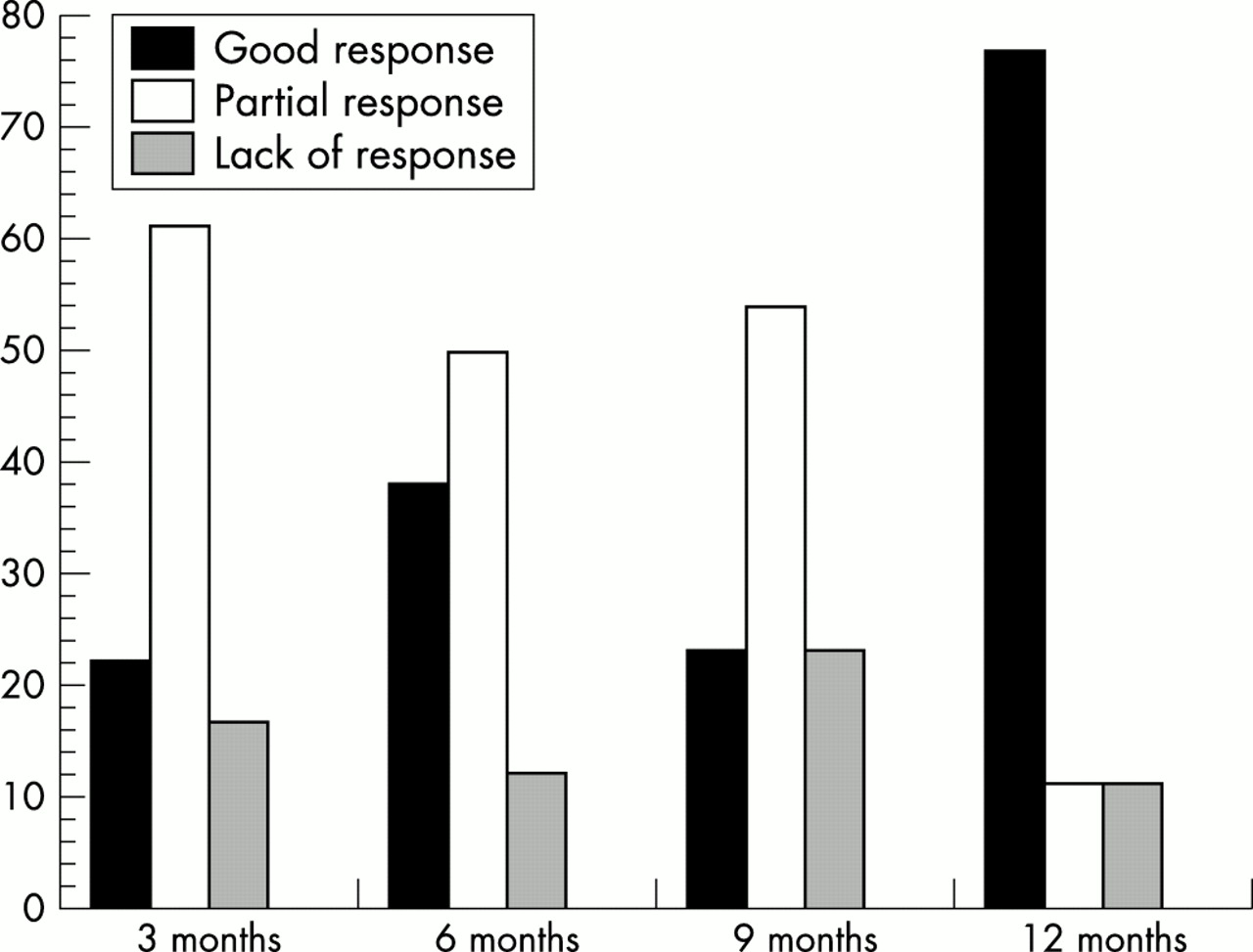
According to the response to treatment at month 3, group 1 showed four good responses (22%), 11 partial ones (61%), and three lacks of response (17%), and in group 2 there were five (38%), six (46%), and two (16%) respectively. The response to treatment along with follow up is described in Figures 1 and 2.
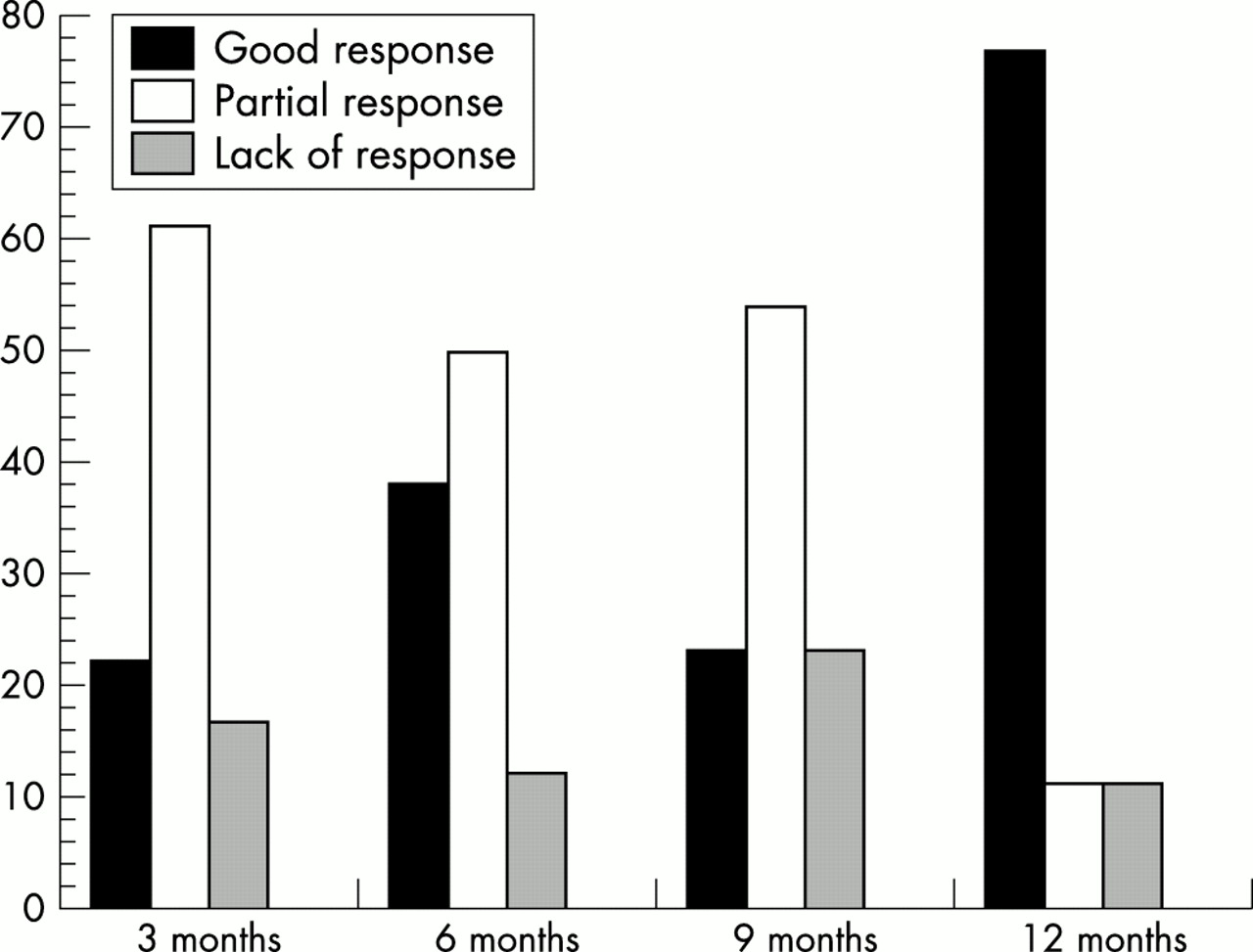
Angiographic response to treatment in group 1 along with follow up.

Angiographic response to treatment in group 2 along with follow up.
Mean BCVA at baseline was 0.22 (0.17) for the whole group and 0.19 (0.14) for group 1 and 0.25 (0.21) for group 2. At month 3 mean BCVA was 0.30 (0.18) for group 1 and 0.25 (0.23) for group 2, and at month 6 it was 0.35 (0.20) and 0.21 (0.21) respectively. At month 12 BCVA was 0.26 (0.20) for the whole group; 0.30 (0.24) for group 1 and 0.21 (0.15) for group 2. In group 1 seven eyes (39%) showed an improvement of four to seven lines, four eyes (22%) of two to three lines, two eyes (11%) showed no changes (one or none lines, won or lost), three eyes (17%) lost two to three lines, and two eyes (11%) lost four to seven lines. In group 2 six eyes (46%) improved two to three lines, six (46%) lost two to three lines, and one (8%) lost four to seven lines. There were no statistically significant improvement in BCVA for either group though it was close to significance in group 1 (p=0.07 for group 1 and p=0.24 for group 2, Student’s t test for paired data).
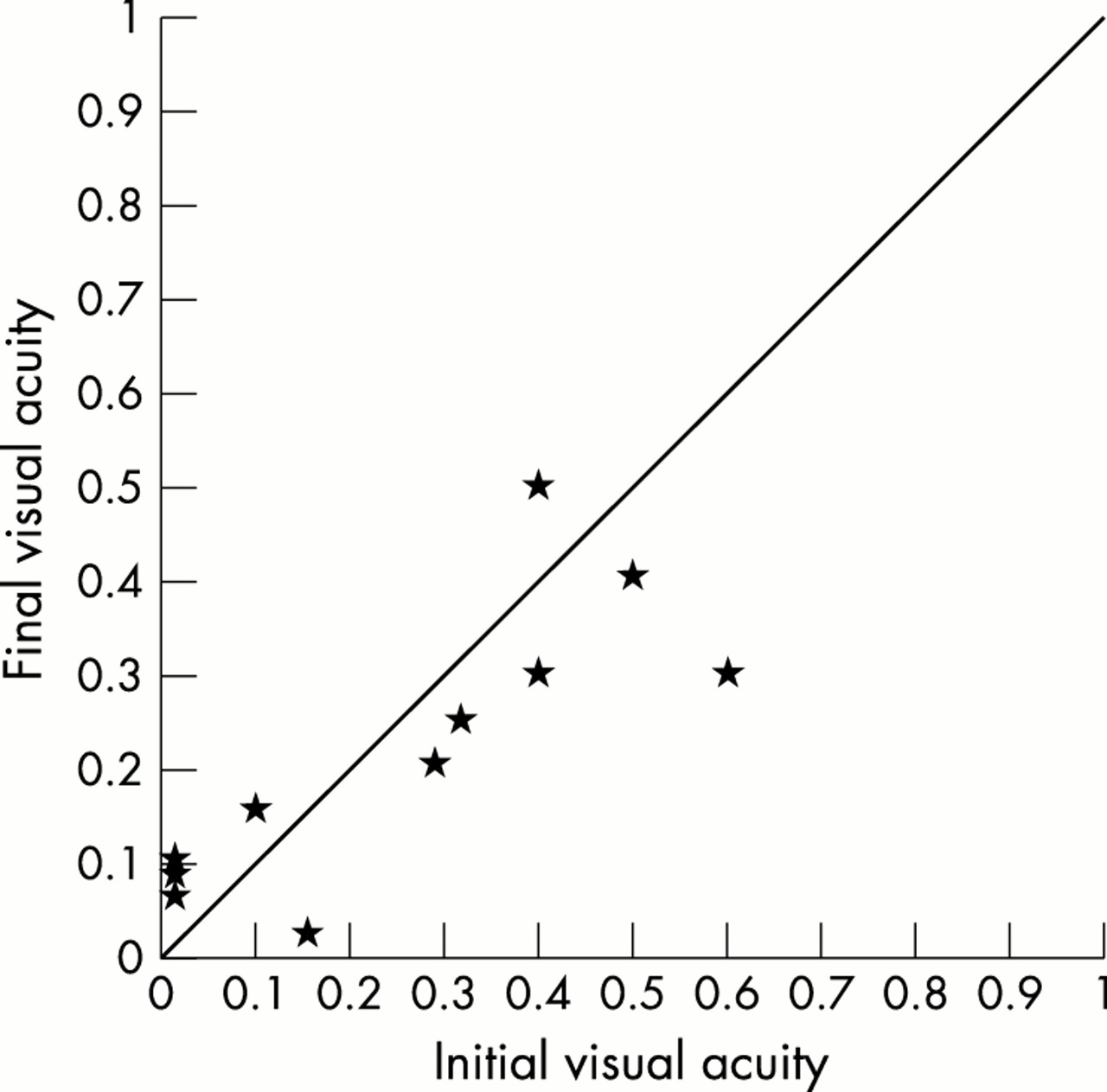
Figures 3 and 4 show the distribution of initial and final visual acuity in both groups. In group 1 (Fig 3) more patients had an improvement in BCVA than in group 2 (Fig 4) during the follow up period.

Initial and final visual acuity in group 1. Points above the line indicate improvement in visual acuity, and points under the line indicate worsening.
Initial and final visual acuity in group 2. Points above the line indicate improvement in visual acuity, and points under the line indicate worsening.
Chorioretinal atrophy was graded as M1–M2 in 14 eyes (78%) and as M3–M4 in four eyes (22%) in group 1, and as M1–M2 in five eyes (38%) and as M3–M4 in eight eyes (62%) in group 2. Retinal fibrosis was observed in 55% of eyes in group 1 and 30% in group 2.
In group 1 four eyes (22%) showed a total closure of the CNV after one session of PDT, four eyes (22%) needed two sessions, three eyes (17%) needed three sessions, and seven eyes (39%) needed four sessions. In group 2 three eyes (23%) showed a total closure of the CNV after one session, five eyes (39%) needed two sessions, one eye (7%) needed three sessions, and four eyes (31%) needed four sessions.
Fourteen patients of 30 were taking antioxidants of different brands. No statistically significant difference in the visual outcome was noticed between patients on antioxidants and those who were not taking them.
CASE REPORTS
Patient 1
A 52 year old man with a spherical equivalent of −10 D and a M3 degree of chorioretinal atrophy was initially seen with a decreased BCVA of hand movements in his right eye. Fluorescein angiography was performed, which showed a CNV 1782 μm wide (Fig 5A). PDT was performed and after 3 months BCVA was 0.3 with a reduction in the size of the CNV to 1525 μm. The patient received a new session of PDT resulting in a BCVA of 0.4 with a total closure of the CNV at month 6 and a fibrotic response. No changes in visual acuity or activity of the CNV were noticed at months 9 and 12 (Fig 5B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Fluorescein angiogram (FA) of patient 1 before treatment. A subfoveal classical CNV 1782 μm wide can be seen. (B) FA of the same patient at month 12 after two sessions of PDT. The activity of the CNV has disappeared and a residual late stain of the fibrotic scar can be seen. (C) FA of patient 2 before treatment. A 945 μm wide subfoveal CNV can be seen in an atrophic fundus. (D) FA of the same patient 9 months later. The CNV is closed and BCVA has stabilised.
Patient 2
A 67 year old woman with medical history of high blood pressure and having treatment with systemic antioxidants, was initially seen with a decrease of BCVA to 0.4 in her left eye. Her spherical equivalent was −8D and showed a M4 degree of chorioretinal atrophy. She showed a 945 μm wide CNV (Fig 5C) which was treated with PDT, achieving 3 months later a BCVA of 0.62 with a total closure of the CNV (Fig 5D), which remained inactive for the rest of the follow up. BCVA acuity decreased to 0.2 at month 6 and was stable at month 9 and 12 at 0.3.
DISCUSSION
High myopia is the second most frequent cause of CNV after ARMD, and the seventh cause of legal blindness in United States16 causing up to 8.8% of blindness in Europe.17 Direct laser photocoagulation is no longer advisable for subfoveal CNV since it causes full thickness burns in the retina which give way to irreversible scotomas.7,8 Surgical removal of the CNV, though achieving good anatomical results, often causes loss in retinal pigment epithelium cells and poor final visual acuity.10,11 Surgical macular translocation is a procedure which was first performed in eyes with ARMD, though the smaller size of myopic CNV makes these latter more suitable for treatment.12–14 Radiotherapy has also been advocated by Kobayashi,9 with some good results, but the risk of malignancy in younger patients makes it unsuitable for the treatment of myopic maculopathy.
Though the frequency of high myopia has been described as similar in both sexes, we have found a higher frequency of women among patients with myopic CNV, which has also been described by other authors.5,7,18 A small number of patients under 45 years has also been found (five of 30).
No relation between spherical equivalent and the evolution of the CNV or the visual outcome has been found. The mean spherical equivalent was similar to those published in other series.15
We have not considered the possibility of a control group since the results published by the VIP1 study proved the good effects of PDT on highly myopic CNV,15 and we did not consider it ethically admissible to leave patients untreated.
In this study we have divided the patients into two groups according to their age, in order to evaluate the possible influence of ARMD in the evolution of highly myopic CNV.19 The mean age in our study was 52, and 65% of patients were aged 50 or more, compared to 51 and 56% respectively in VIP 1. This allows us to compare our results with those of VIP 1, and to some extent, to consider the outcome of their control group as a control for ours.
This study shows that verteporfin PDT can increase the chance of stabilising or improving vision for at least 1 year in highly myopic patients with CNV, especially if they are under 56 years of age. With a mean baseline BCVA of approximately 0.22 for the whole group and 0.19 for group 1 and 0.25 for group 2, small improvements in BCVA were noticed. These were more noticeable in group 1, in which 60% of patients improved their BCVA after 1 year, and 28% showed a decrease in BCVA. In group 2 most of the patients (90%) showed stabilisation or a slight increase or decrease (plus or minus three lines) in BCVA, results which agree with those published by the VIP 1 study. 54% of placebo treated patients in VIP 1 study showed a worsening in BCVA and only 20% showed a spontaneous improvement in BCVA after 1 year.
The results published earlier by other authors on the spontaneous outcome of highly myopic CNV1,5,7 show a poor evolution of BCVA in these patients.
Recently Yoshida et al20 have published results on spontaneous visual outcome after at least 3 years of follow up on patients with myopic CNV. These authors have found a better spontaneous visual outcome in younger patients, finding that 27% of patients ≤ 40 years old improved their BCVA, and 19% of them showed a decrease in BCVA by the end of the follow up. In comparison, 17% of patients >40 years old improved and 51% of them had a worsening in BCVA. In spite of the different periods of follow up, and the higher ages of the patients in our study, the results of treated patients in our series are better than those of untreated patients in Yoshida’s study.
Among other therapeutic approaches, only macular translocation has shown good results. Fujikado13 has achieved improvements in eight of 11 patients, though other series have not shown such good results. This technique is not only difficult to perform, making it unavailable for most of patients, but also presents many complications such as retinal detachments, epiretinal membranes, and macular holes.21
CNV response to treatment was better in group 2, with 38% good responses at month 3 and 54% at month 6, compared to 22% and 38% respectively in group 1. Yet at the end of the year both groups showed 76% of good responses with total closure of the CNV, and both groups needed a similar number of PDT sessions (2.7 in group 1 and 2.4 in group 2).
Chorioretinal atrophy was more severe in group 2. This difference was statistically significant (χ2 test p<0.05) and could be related both to the age related systemic vascular atrophy and to the longer evolution of myopic atrophy. According to Avila, higher degrees of chorioretinal atrophy are related to less aggressive forms of CNV with a lesser degree of fluorescein leakage.5 We have found a better early response to treatment in group 2 (38% closures at month 3 in group 2, 22% in group 1) which may be related to a lower vitality of the CNV due to a weaker vascular network and a smaller capability of maintaining or reforming the CNV. Yet this higher chorioretinal atrophy is also related to a worse visual prognosis.5
In all, 76% of the CNV were closed at the end of follow up, 11 of them after four sessions of PDT. A similar rate of closure was achieved by the end of follow up in both groups of patients.
The good results in terms of BCVA and CNV closure in the patients treated compared to the results of the control group of other series, especially that of the VIP 1 study which is in demographic terms similar to ours, lead us to recommend verteporfin PDT in the treatment of highly myopic patients with subfoveal CNV. These results are better especially in patients under 56 years of age, and with lower degrees of chorioretinal atrophy.