Article Text

Abstract
Aim: To report the short and medium term outcome of a prospective series of sutureless manual extracapsular cataract extractions (ECCE) at a high volume surgical centre in Nepal.
Methods: Cataract surgery was carried out, on eyes with no co-existing diseases, in 500 consecutive patients who were likely to return for follow up. The technique involved sclerocorneal tunnel, capsulotomy, hydrodissection, nucleus extraction with a bent needle tip hook, and posterior chamber intraocular lens (PC-IOL) implantation according to biometry findings. Surgical complications, visual acuity at discharge, 6 weeks, and 1 year follow up, and surgically induced astigmatism are reported.
Results: The uncorrected visual acuity at discharge was 6/18 or better in 76.8% of eyes, and declined to 70.5% at 6 weeks’ follow up, and 64.9% at 1 year. The best corrected visual acuity was 6/18 or better in 96.2% of eyes at 6 weeks and in 95.9% at 1 year. Poor visual outcome (<6/60) occurred in less than 2%. Intraoperative complications included 47 (9.4%) eyes with hyphaema, and one eye (0.2%) with posterior capsule rupture and vitreous in the anterior chamber. Surgery led to an increase in against the rule astigmatism, which was the major cause of uncorrected visual acuity less than 6/18. Six weeks postoperatively, 85.5% of eyes had against the rule astigmatism, with a mean induced cylinder of 1.41 D (SD 0.8). There was a further small increase in against the rule astigmatism of 0.66 D (SD 0.41) between 6 weeks and 1 year. The mean duration of surgery was 4 minutes and the average cost of consumables, including the IOL, was less than $10.
Conclusion: Rapid recovery of good vision can be achieved with sutureless manual ECCE at low cost in areas where there is a need for high volume cataract surgery. Further work is required to reduce significant postoperative astigmatism, which was the major cause of uncorrected acuity less than 6/18.
- cataract surgery
- extracapsular cataract extraction
- Nepal
- astigmatism
Statistics from Altmetric.com
Age related cataract remains the major cause of blindness throughout the world.1–3 Phacoemulsification has become the routine procedure for cataract extraction in industrialised countries, as it offers faster visual recovery, and better uncorrected visual acuity than sutured manual extracapsular cataract extraction (ECCE).4 In developing countries there has been a shift to surgery with an intraocular lens (IOL), but phacoemulsification has had a limited role, owing to the expense of equipment and consumables, and the high proportion of eyes with dense nuclei and mature cataracts. In order to obtain the advantages of a self sealing sutureless incision at low cost, developing world ophthalmologists are considering alternatives to phacoemulsification.
Several methods have been described and various names given—for example, manual small incision cataract surgery (SICS), mini-nuc technique, manual phaco—for sutureless manual ECCE,5–9 a procedure in which the entire nucleus is removed through a sclerocorneal tunnel. However, these techniques have been superseded by phacoemulsification in most industrialised countries. Recently, there has been renewed interest in their application in the Third World,10 where this type of surgery may be most useful.
Studies of the outcome of cataract extraction in Asia have shown that presenting acuity following surgery is less than 6/60 in 15–20% of eyes.11–14 Many of the poor outcomes are due to uncorrected refractive error. This can be reduced by the use of IOL, but residual refractive error, particularly postoperative astigmatism, remains a problem.15,16
Lahan Eye Hospital in Nepal has conducted more than 100 000 sutureless cataract surgeries in the past 4 years. The technique used is evaluated and reported in this prospective study.
MATERIALS AND METHODS
Participants
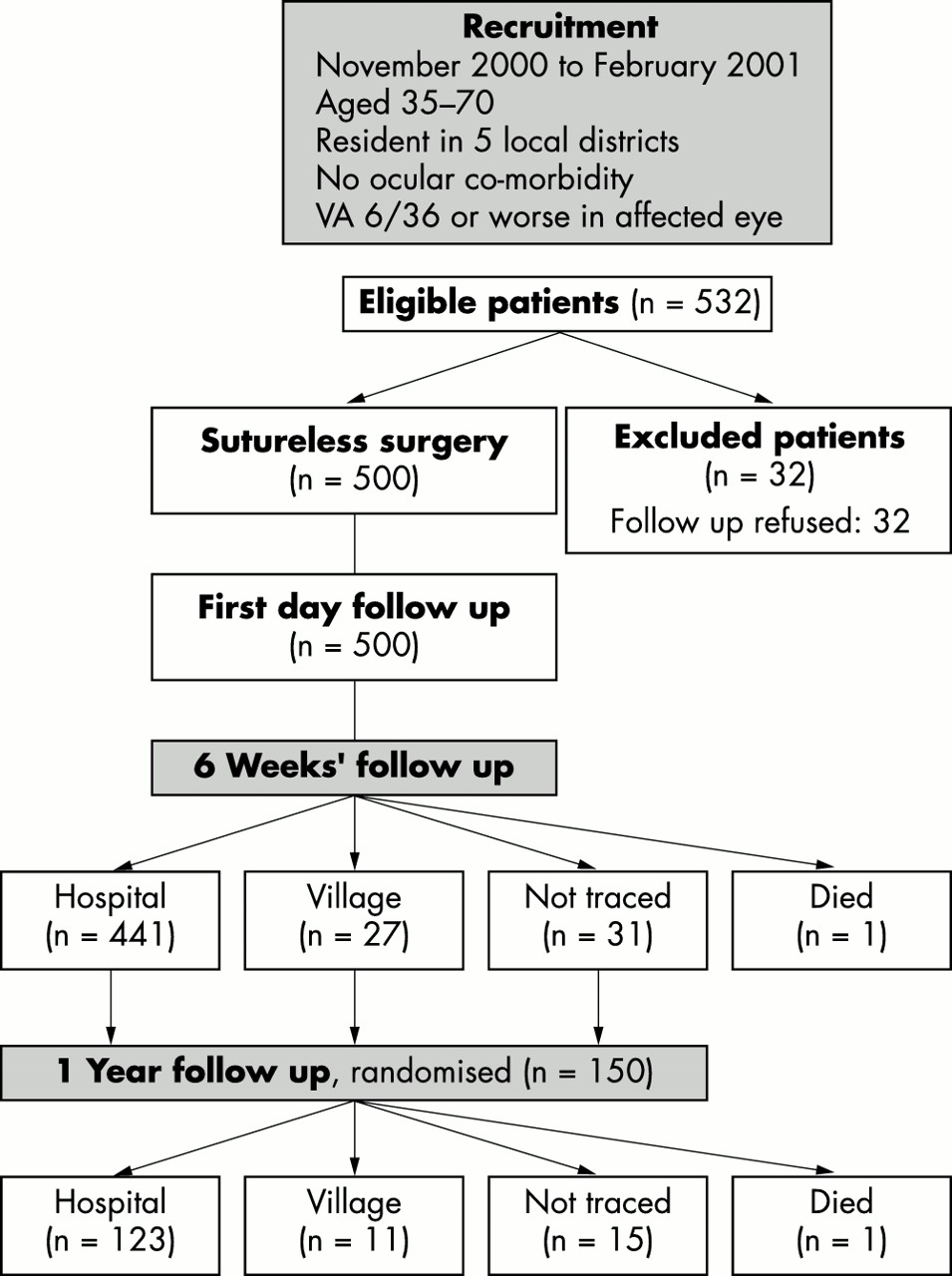
Between November 2000 and February 2001, 14 500 cataract operations were carried out at Lahan. Of these, 532 patients came from one of the five districts close to the hospital, were aged 35–70 years, had a visual acuity of 6/36 or less as a result of cataract, and had no known co-existing eye disease; 32 patients were excluded as they were unable to return for follow up (Fig 1). Standard clinical examination included visual acuity testing with Snellen chart, slit lamp biomicroscopy, and funduscopy.

Patient selection and follow up.
IOL power was calculated according to contact A-scan biometry. Keratometry was performed before surgery, and at 6 weeks and 1 year after surgery, using a hand held automatic refract-keratometer (Retinomax, Nikon, Japan).
Surgical method
An ophthalmic assistant performed a retrobulbar anaesthetic block outside the operating theatre. The patient then walked into the operating theatre to one of the four tables used in rotation. A trained assistant prepared the eye for surgery by placing a superior rectus suture, preparing a fornix based conjunctival flap at the 12 o’clock position, and cauterising scleral blood vessels. Surgery was performed by one experienced ophthalmologist (AH), in a standing position, maintaining a no-touch technique, and using a 5× prism loupe magnification (Carl Zeiss, Germany).
A diamond knife was used for the following four steps: frown incision, sclerocorneal tunnel, opening of the anterior chamber (AC), and linear capsulotomy. The central frown incision was at least 2 mm behind the limbus and the external width of the incision was 6–8 mm according to the expected size of the nucleus (see Fig 2). The internal opening was wider, in order to facilitate nucleus delivery. A horizontal linear incision was made in the anterior capsule.

Wound construction. The internal opening of the scleral tunnel is wider than the external opening.
After hydrodissection the nucleus was mobilised within the capsular bag. Hydrodelineation was not used. Viscoelastic was injected between posterior capsule and nucleus and into the anterior chamber.
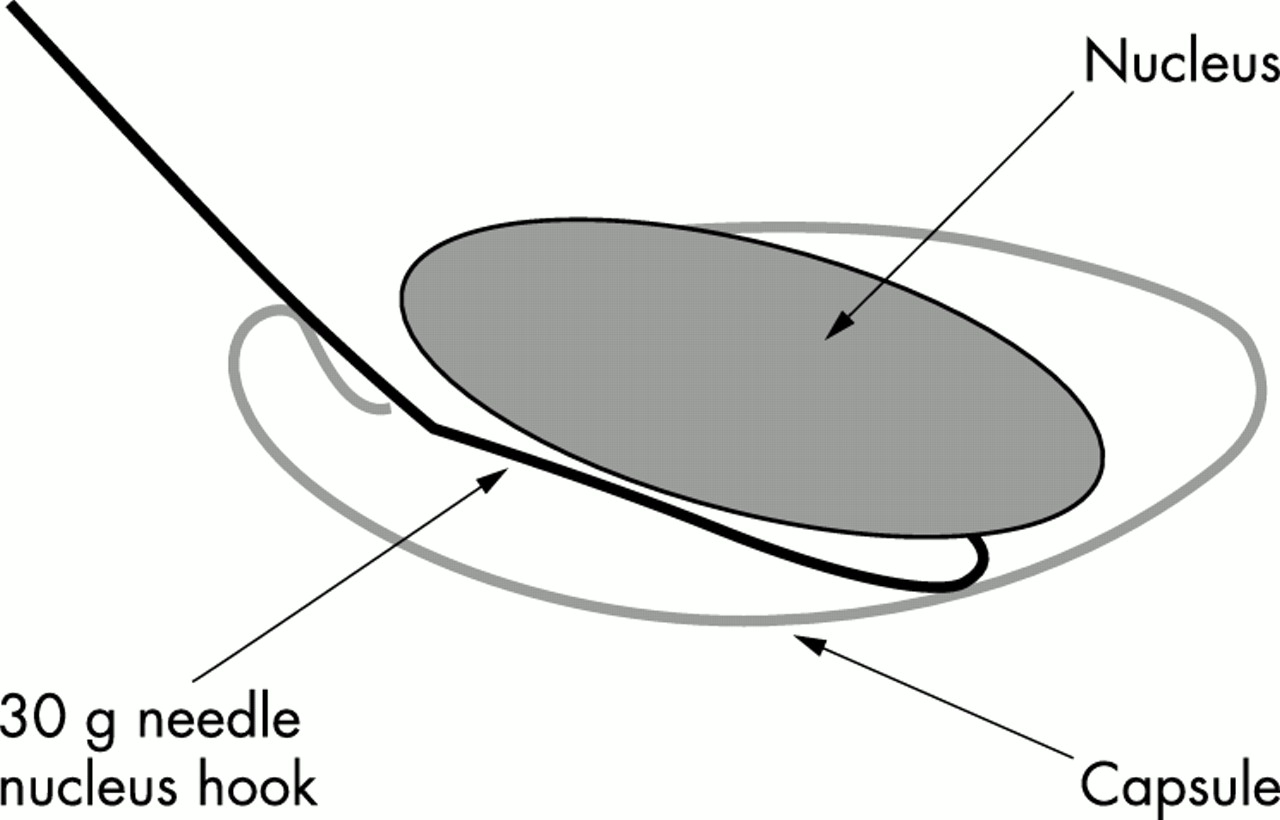
The bent tip of a 30 gauge needle (made into a hook), was inserted between nucleus and posterior capsule (see Fig 3) and the nucleus was extracted through the tunnel using gentle traction with the hook. The remaining cortex was aspirated using a Simcoe cannula.

{kind=link}
{kind=link}
{kind=link}
Nucleus extraction. The hook is inserted between the nucleus and the posterior capsule, with the sharp tip horizontal. Then the tip is turned upwards. As the hook is withdrawn, it engages the nucleus, and delivers it from the eye.
A single piece poly(methyl methacrylate) posterior chamber IOL (PMMA, FH 106, manufactured by Fred Hollows IOL Laboratories, Kathmandu, Nepal) was inserted into the capsular bag, and the remaining anterior capsule was removed with a Simcoe cannula. The assistant closed the conjunctiva with one 8-0 silk suture and injected gentamicin 20 mg and dexamethasone 4 mg in the lower fornix as well as depot steroid in the upper fornix. The patient walked back to the ward with assistance.
Follow up
On the first postoperative day the uncorrected visual acuity and best spherical equivalent were recorded, and the eye was examined by an ophthalmologist. Acuities were analysed according to the WHO definitions of good (6/18 or better), borderline (less than 6/18–6/60), or poor (less than 6/60) outcomes.
The next day, patients were discharged and were requested to return for follow up examination after 6 weeks. Reminder cards were sent to anyone who did not attend at 6 weeks. Travel and food expenses were reimbursed. For the 1 year follow up 150 patients were randomly selected and asked to come to the hospital (see Fig 1).
At 6 weeks and at 1 year the visual acuity was recorded with no correction, best sphere correction, and best correction. Keratometry was performed, and induced astigmatism was calculated by Holladay’s method.17 In addition, the keratometric astigmatism score was determined as with the rule, against the rule, and oblique according to Morlet et al.18
At follow up visits, patients were examined by an ophthalmologist, who identified the cause of any uncorrected vision less than 6/18.
Patients who did not attend the hospital were examined in their villages by an experienced ophthalmic assistant. Uncorrected visual acuity and best spherical equivalent were taken and the reasons for uncorrected visual acuity less than 6/18 recorded.
RESULTS
Study group
Of the 500 patients entering the study, 54.2% were female, 42.6% were between 51–60 years old, and 25.8% between 61–70.
Characteristics of surgery
Sutureless sclerocorneal tunnel and nucleus extraction was performed in all cases. The cataract was classified as “immature or mature” in 72.8%, “intumescent” in 8.0%, “hypermature” in 3.6%, and “large nucleus” in 15.6%.
Peroperative posterior capsule plaques were noted in 121 (24.2%), out of which 80 (16.0%) were in the optical centre.
The powers of the implanted IOLs following biometry are shown in Table 1. No lenses of less than 18D or greater than 24.5D were required, as patients with high ametropia were excluded from the study.
Power of IOL required to achieve emmetropia according to biometry
Peroperative complications
The surgery was uneventful in 452 (90.4%). In 9.4% there was bleeding from the tunnel into the AC at the end of the surgery. The patient left the operating theatre only after the bleeding had stopped and the blood was removed from the AC. In one patient vitreous was seen in the AC during slit lamp examination on first postoperative day, indicating posterior capsule rupture.
Postoperative complications
Six eyes (1.2%) required a second operation, four to remove blood from the AC, one for lens matter aspiration, and one for IOL repositioning. A total of 469 patients (93.8%) were discharged on the second postoperative day; 24 patients were discharged on the third postoperative day as a result of hyphaema in 19, uveitis in two, and corneal oedema, IOL repositioning, or lens matter aspiration in one case each. Seven patients were discharged on the fourth postoperative day because of hyphaema in six and uveitis in one.
Two eyes had a visual acuity of less than 6/18 owing to persistent corneal oedema 6 weeks postoperatively.
Three eyes out of 134 (2.2%) developed posterior capsule opacification reducing the vision below 6/18 by 1 year (see Table 3).
Visual acuity
The visual acuities at discharge, at 6 weeks, and at 1 year after surgery are shown in Table 2.
Visual acuity in 500 operated eyes undergoing sutureless ECCE and PC-IOL
Uncorrected visual acuity was 6/18 or better in 76.8% of eyes at discharge, and in 70.5% at 6 weeks’ follow up (χ2=4.62, p=0.03). At 1 year 64.9% had 6/18 or better without correction, which is not significantly different from the proportion achieving 6/18 unaided at 6 weeks (χ2=1.32, p=0.25). There was no change in the proportion of eyes achieving a best corrected visual acuity of 6/18 or better at 6 weeks (96.2%) and 1 year (95.9%). Poor visual outcome (best corrected visual acuity less than 6/60) was 0.2% at 6 weeks and 0.0% at 1 year.
The commonest cause of an uncorrected vision of less than 6/18 was astigmatism (Table 3).
Causes of uncorrected visual acuity <6/18 at 6 weeks and at 1 year follow up, after sutureless ECCE and PC-IOL
Astigmatism
Preoperative keratometric astigmatism is shown in Table 4. The majority (65.4%) had against the rule astigmatism. Only 338 eyes are included. In 162 eyes the cataract was so dense that patients were unable to fixate on the target in the automated keratometer. In these patients an approximate mean K value was obtained from the other eye for biometry. The mean astigmatism score was 3.64 (SD 2.30).
Astigmatism
Keratometry was carried out on 442 eyes at 6 weeks after surgery, and the results are shown in Table 4. In these eyes, 85.5% had against the rule astigmatism. The mean astigmatism score was 6.08 (SD 2.60).
In 297 eyes that had keratometry preoperatively and at 6 weeks, the mean change in astigmatism score was 2.28 (95% CI 1.90 to 2.55, Student’s t = 11.67, p<0.001). Analysis of the surgically induced refractive change showed that the mean induced astigmatism was −1.41D (SD 0.80), at a mean axis of 103 (SD 37.50). An against the rule shift was seen in 60.9%, and an oblique shift in 21.8%. The induced astigmatism was greater than 2D in 20.1% and less than 1D in 32.2%.
In 114 eyes that had keratometry at both 6 weeks and 1 year after surgery, the mean change in astigmatism score was 0.23 (95% CI −0.43 to 0.89, p=0.5). Analysis of induced refractive change showed that the mean induced astigmatism was −0.66 (SD 0.41), at a mean angle of 97 (SD 50.8). The induced astigmatism was less than 1D in 80.9% and greater than 2D in 1.7%.
Cost and time
The cost of consumables per cataract operation including IOL, all medicines used before, during and after surgery, anaesthesia, viscoelastics, irrigation solution, disinfectants, and eye pads is approximately US$6.50. This calculation is based on figures for the year 2001. The median duration of surgery was 4 minutes.
DISCUSSION
Many patients travel considerable distances to obtain treatment at Lahan, and they usually cannot return for postoperative examinations. In order to obtain adequate follow up in such difficult circumstances, only 500 patients from closer districts out of a total of 14 500 were selected. All patients with known pre-existing eye disease were excluded. The authors believe that the selection of local patients has not biased the results, as there is no evidence that district of residence influences the outcome of cataract surgery.
Surgical outcome
Sutureless cataract surgery is more difficult than conventional sutured ECCE and PC-IOL. The preparation of a relatively long and narrow sclerocorneal tunnel, handling the instruments, and removing the entire nucleus all require good surgical skills and additional training. However, once the technique is mastered the surgery is faster and less expensive, because no sutures are required. When performed by an experienced surgeon, the complication rate is low—there was only one posterior capsule rupture in this study. In Japan, posterior capsule rupture occurred in 5.9% of eyes, and this was thought to be the result of learning the new technique.9
Bleeding from the wound into the AC occurred in 9.4% of operations, which prolonged the surgery by another 5 minutes. Hyphaema was the most common complication resulting in four additional intraocular procedures and 36 additional patient days in hospital.
Two eyes suffered persistent corneal oedema. Removal of the nucleus through a scleral tunnel can be traumatic. Endothelial damage can be minimised by nucleus extraction from within the capsular bag rather than displacing the nucleus into the AC. This reduces manipulation in the AC, and avoids contact between the nucleus and the endothelium. Endothelial trauma can be reduced further by the use of intracameral viscoelastics before extraction of the nucleus.19
Eighty (16.0%) of cases had pre-existing central posterior capsule plaques; however, only 10 of the 80 cases had an acuity less than 6/18 at discharge attributable to the plaque. The frequency and location of this type of posterior capsule opacification corresponds with a previous histopathological study on human crystalline lenses from our centre.20
Visual outcome
Before surgery nearly all eyes (96.8%) were severely visual impaired or blind. This was reduced to less than 1% by discharge.
In comparison with sutured manual ECCE and PC-IOL, sutureless surgery provides fast visual recovery. In our patients, 76.8% had an unaided acuity of 6/18 or better at discharge (Table 2). By comparison, in a randomised controlled trial of standard ECCE and PC-IOL and intracapsular cataract extraction and aphakic glasses, only 57.5% of the ECCE and PC-IOL eyes achieved an unaided acuity of 6/18 or better by 2 months after surgery.15 However, another study of sutureless ECCE in Nepal showed that only 58.3% of eyes obtained an uncorrected vision of 6/18 or better at 8 weeks.10
The low incidence of poor visual outcome (less than 6/60) is due to the low rate of operative complications, and to the exclusion of eyes with known comorbidity.
There was a statistically significant reduction (6.3%) in the number of eyes achieving 6/18 or better without correction between discharge and 6 weeks’ follow up. A further slight decrease (5.6%) between 6 weeks and 1 year was not significant. The most likely cause for the worsening uncorrected acuity is an increase in surgically induced astigmatism (Table 4).
In another study of sutured ECCE and PC-IOL, the proportion of eyes with an uncorrected vision of 6/18 or better increased from 57.5% at 2 months to 83.7% by 1 year.15
Although keratometry was not performed at discharge, it seems likely that the worsening of unaided acuity is the result of increasing against the rule astigmatism. Between 6 weeks and 1 year, the increase in astigmatism and the corresponding decrease in unaided visual acuity is small, suggesting that, in most cases, the wound is stable by 6 weeks after surgery.
In nearly two thirds of the eyes with an unaided acuity less than 6/18, the cause of reduced vision was astigmatism. We tried to limit the astigmatism by placing the incision as far behind the limbus as possible, and by keeping the width of the sclerocorneal tunnel to a minimum. However, in eyes with large nuclei, the incision had to be 8 mm wide in order to extract the nucleus. Even these larger tunnel openings remained self sealing without sutures.
The mean induced astigmatism of 1.4D is similar to other reports from industrialised countries.9,19
It is known that uncorrected refractive error is a common cause of poor outcome following cataract surgery in developing countries. The cost of glasses, and, in some countries, the lack of expertise to prescribe and manufacture high quality spectacles, limits their use. If the outcome of cataract surgery globally is to improve, it is imperative to find means of improving uncorrected postoperative visual acuity, as well as best corrected vision. We believe that the technique of sutureless ECCE may help to increase the number of patients with good uncorrected vision.
Refinements in the surgical technique may further reduce refractive error as a cause of poor vision after this type of surgery. For example, a single radial stitch may reduce against the rule astigmatism in sutureless ECCE.21 Alternatively, a temporal or oblique incision may be performed in eyes that have against the rule astigmatism preoperatively. In this study, 65.4% of eyes had against the rule astigmatism before surgery (Table 4).
Keratometry and A-scan
For keratometry we used an automated keratometer, which requires the patient’s cooperation to fixate on an illuminated target. Many patients with advanced cataract were unable to focus on this symbol, making it difficult to obtain reproducible keratometer readings. In such cases we performed keratometry on 162 fellow eyes with less cataract, and assumed that the average corneal power was similar in both eyes.
The time required for preoperative biometry was greater than for the surgery itself. In this population axial ametropia appears to be relatively uncommon, although patients with known high myopia were excluded. At least 78% of eyes would have been within 1D of emmetropia with a 22D lens. Further study is required to weigh the visual benefits of biometry against the extra costs and time required in rural settings with a high surgical volume.
Cost of surgery
It has been shown that, in Europe, phacoemulsification with a foldable IOL is less costly than manual ECCE and IOL.4 However, this analysis did not include the capital cost of a phacoemulsifier, and used a PMMA IOL costing £38.00. In developing countries, high quality, locally made IOLs can be purchased for less than £3.00, but high quality foldable IOLs must be imported, and are much more expensive. The use of locally produced consumables minimises the cost of surgery. Until phacoemulsification consumables, and foldable IOLs, can be manufactured in developing countries, phacoemulsification will be too costly for the majority of cataract patients.
This study shows that sutureless manual cataract surgery can be a safe and effective technique in the hands of an experienced surgeon in areas with a high demand for cataract surgery, including advanced cataract with large nuclei.
The surgical technique is more demanding than sutured ECCE and PC-IOL and requires additional surgical training. However, once this technique is mastered it provides a good visual outcome and fast visual recovery. Further work is required to reduce the incidence of peroperative hyphaema and postoperative astigmatism.
REFERENCES
Footnotes
Series editors: W V Good and S Ruit
Linked Articles
- BJO at a glance