Article Text

Abstract
Background/aim: There are two theories on the pathogenesis of polypoidal choroidal vasculopathy (PCV): variants in choroidal neovascularisation (CNV) and inner choroidal vessel abnormalities. On indocyanine green angiography (IGA) with a video camera system, PCV has a characteristic appearance, but inadequate image quality has made detailed interpretation difficult. This study aims to improve imaging, using confocal scanning laser ophthalmoscopy (SLO), to elucidate the pathogenesis of PCV.
Methods: High speed IGA with confocal SLO of 45 eyes (44 patients) showed typical PCV findings of a branching vascular network and polypoidal lesions.
Results: Vessels comprising branching networks began to fill simultaneously with the surrounding choroidal arteries in 38 eyes. Small numbers of vessels filling within a branching network, in the arterial and arteriovenous phases of IGA, showed focal dilatation, constriction, and tortuousity. Vessel abnormalities, corresponding to polypoidal lesions, existed within a network in eight eyes and included loops similar in calibre to network vessels, and numerous microaneurysmal dilatations of small vessels. Vessel pulsation was seen in 24 eyes.
Conclusion: PCV is caused by inner choroidal vessel abnormalities, not CNV.
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- IGA, indocyanine green angiography
- OCT, optical coherence tomography
- PCV, polypoidal choroidal vasculopathy
- RPE, retinal pigment epithelium
- SLO, scanning laser ophthalmoscopy
- confocal scanning laser ophthalmoscopy
- high speed indocyanine green angiography
- polypoidal choroidal vasculopathy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- IGA, indocyanine green angiography
- OCT, optical coherence tomography
- PCV, polypoidal choroidal vasculopathy
- RPE, retinal pigment epithelium
- SLO, scanning laser ophthalmoscopy
- confocal scanning laser ophthalmoscopy
- high speed indocyanine green angiography
- polypoidal choroidal vasculopathy
Statistics from Altmetric.com
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- IGA, indocyanine green angiography
- OCT, optical coherence tomography
- PCV, polypoidal choroidal vasculopathy
- RPE, retinal pigment epithelium
- SLO, scanning laser ophthalmoscopy
- confocal scanning laser ophthalmoscopy
- high speed indocyanine green angiography
- polypoidal choroidal vasculopathy
- AMD, age related macular degeneration
- CNV, choroidal neovascularisation
- IGA, indocyanine green angiography
- OCT, optical coherence tomography
- PCV, polypoidal choroidal vasculopathy
- RPE, retinal pigment epithelium
- SLO, scanning laser ophthalmoscopy
- confocal scanning laser ophthalmoscopy
- high speed indocyanine green angiography
- polypoidal choroidal vasculopathy
Polypoidal choroidal vasculopathy (PCV), first described by Yanuzzi,1 consists of a branching vascular network, with polypoidal lesions at its edge, under the retinal pigment epithelium (RPE).2 Patients may experience recurrent subretinal haemorrhages and exudates, and RPE detachments.1 Presumptive PCV diagnosis is based on ophthalmoscopic identification of subretinal reddish-orange spheroidal lesions arising from choroidal vessels.1 Indocyanine green angiography (IGA) provides definitive diagnosis and greater detail.1,2 However, neither video fundus photography, which has low image contrast, nor non-confocal scanning laser ophthalmoscopy (SLO) yields detailed IGA findings of PCV.
Confocal SLO has a small aperture in front of a photodetector. Light scattered at a point outside the focus plane, or coming from a point situated off the optical axis, is blocked by the aperture, enhancing image contrast.3–5 This modality visualises the choroidal circulation.5 We used confocal SLO with >20 images/second—that is, high speed IGA, to obtain detailed findings and clarify PCV pathophysiology.
SUBJECTS AND METHODS
We examined 45 eyes (44 patients; 40 males, four females, average age 65 years, range 53–81 years) with typical PCV features—that is, serous and haemorrhagic detachments of the RPE and/or neurosensory retina. Other major features were branching vascular networks and polypoidal lesions in the posterior pole, on IGA with confocal SLO (Heidelberg retina angiograph, Heidelberg Engineering, Germany). Eyes also showing classic choroidal neovascularisation (CNV) were excluded.
The 45 eyes underwent fundus photography, fluorescein angiography and IGA. For IGA, indocyanine green dye (25 mg in 1 ml balanced saline) was injected into the cubital vein. IGA images were obtained for the initial 20 seconds, then at intervals, until 30 minutes had elapsed. We assessed when network vessels began to fill, their filling state, and the mechanisms of hypofluorescence in early and hyperfluorescence in late phase IGA, in and around network vessels. We observed the locations, architecture, and late phase IGA conditions of polypoidal lesions. Pulsation in branching vessels and/or polypoidal lesions was also determined.
RESULTS
In all 45 eyes, IGA showed arteries of branching vascular networks to overlie large choroidal vessels. These arteries began to fill simultaneously with the surrounding choroidal arteries in 38 eyes. Filling of individual arteries could not be confirmed in seven eyes because of small vessel calibre, rapid dye filling, or blocked fluorescence in part of the network, as a result of RPE detachment or haemorrhage. In 30 eyes, the area within and adjacent to the surrounding network hypofluoresced, in both the arterial and arteriovenous phases of IGA, because of vessel paucity (figs 1A, 2A 3A). Vessels comprising networks varied in size (figs 1–6) and showed focal dilatation, constriction (figs 2, 3), tortuousity (figs 2–5), and unusual courses (figs 2–5). Filling was slow in 20 eyes (fig 3).

Indocyanine green angiography. Few arteries follow tortuous courses (A, 25 seconds). Large calibre vessels, apparently veins, hyperfluoresce (B, 32 seconds).

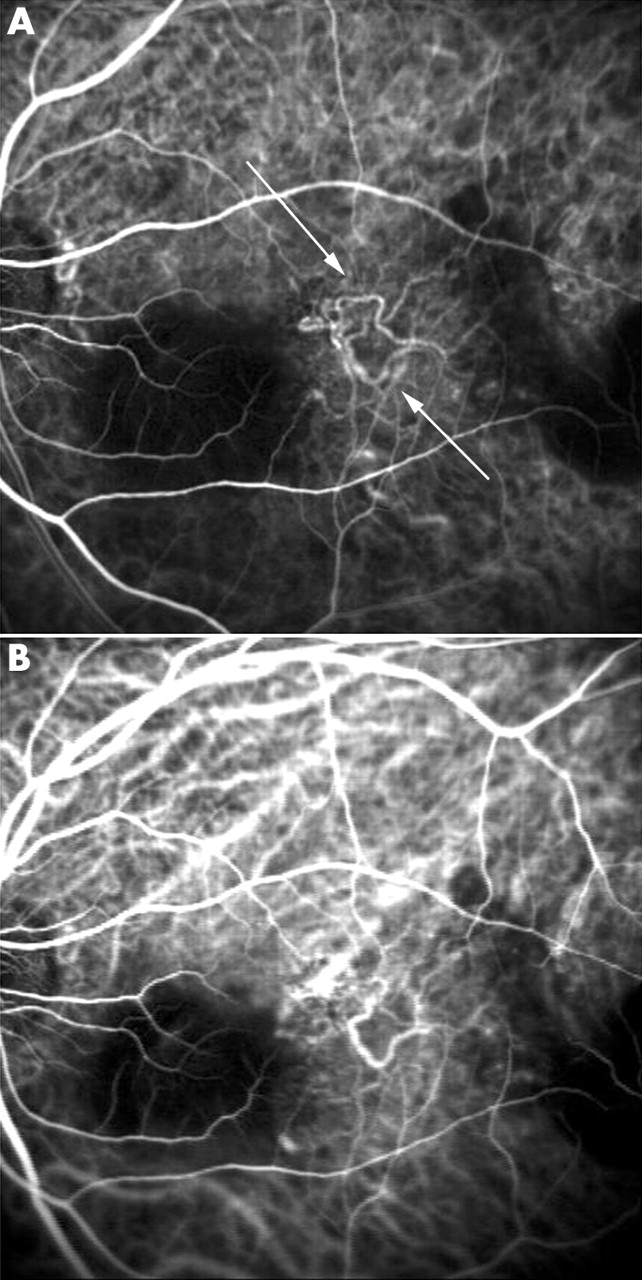
Indocyanine green angiography. Arteries follow tortuous paths, flowing towards the macula. Large branching vessels radiate upwards (A, 28 seconds). An abnormal course of a vessel shows a vascular loop (arrow) (B, 36 seconds). Looped vessel showing leakage, apparently constituting a large polypoidal lesion (C, 73 seconds). Area corresponding to abnormal vessels and polypoidal lesion hyperfluoresces (D, 1566 seconds).

Indocyanine green angiography. Few hyperfluorescent vessels are surrounded by hypofluorescence (arrow). Area in and around arteries hypofluoresces because of vessel paucity (A, 23 seconds). Vessel, with constriction and dilatation, filled slowly (arrow) (B, 29 seconds). Dilatation is more prominent (arrows) (C, 32 seconds).
Indocyanine green angiography. Vessels with abnormal courses appear to be arteries (arrows) (A, 17 seconds), other vessels veins (B, 28 seconds).

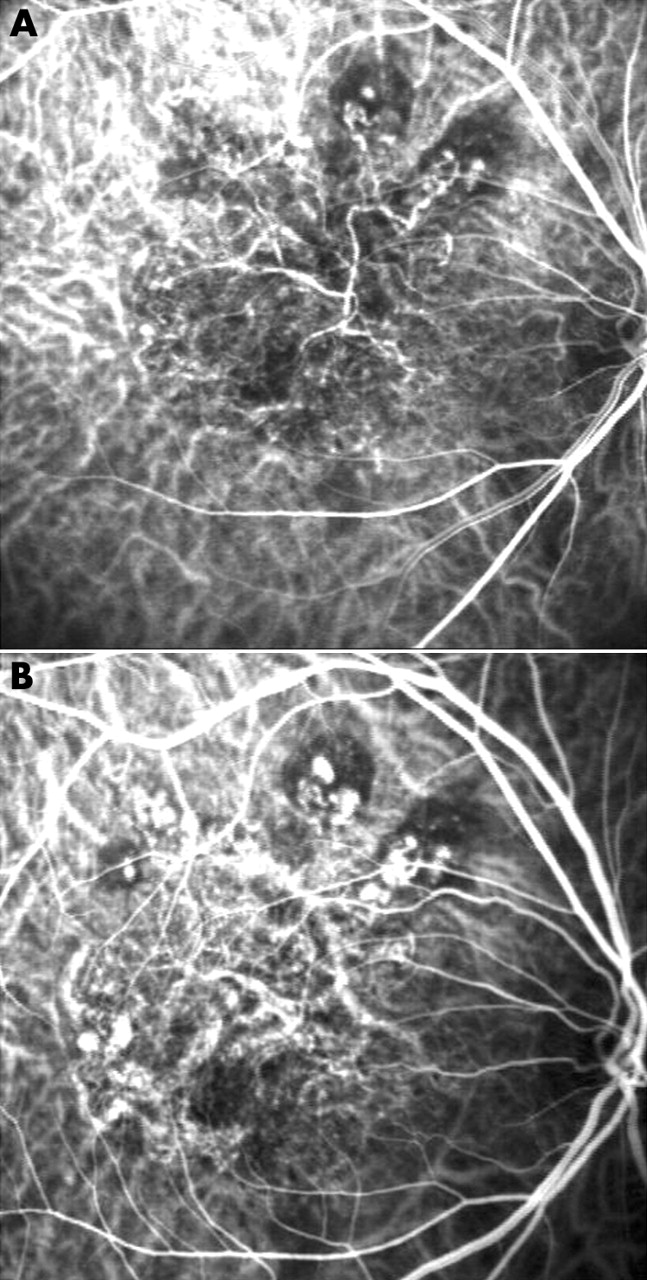
Indocyanine green angiography. Large vessel branching into smaller vessels, with large loops (arrow) (A, 20 seconds); more numerous within hypofluorescent area (B, 24 seconds). Numerous hyperfluorescent dots apparently represent cluster of polypoidal lesions. Area corresponding to large vessel also hyperfluoresces (C, 36 seconds).
The area of hypofluorescence including the network and immediately adjacent areas changed to hyperfluorescence late in IGA (figs 2D, 6B) in 37 eyes but was similar to that in the surrounding area in eight. Hyperfluorescence existed above the network, indicating leakage from network vessels, in 26 of 30 eyes examined stereoscopically.

Indocyanine green angiography. Faint discernible network vessels (A, 24 seconds); hyperfluorescence corresponds to network and polypoidal lesions (B, 533 seconds).
Polypoidal lesions were at the network border in all 45 eyes, but also within it in eight (fig 7). The internal IGA findings of polypoidal lesions were classified into: (1) dense clusters of numerous small hyperfluorescent dots resembling microaneurysmal dilatations (fig 8A); (2) polypoidal lesion consisting of relatively large aneurysmal dilatations, occasionally resembling grape clusters (fig 8B); (3) characteristic large vessel deformations—for example, loop or coil-like configurations, constrictions, and dilatations (fig 8C). The calibre of vessels with unusual configurations is sometimes similar to that of network vessels (fig 2). Uniform or non-uniform hyperfluorescence late in IGA, corresponding to most polypoidal lesions, was attributed to leakage from focal or global abnormalities of vessels entering polypoidal lesions (fig 9). Ring of hyperfluorescence (18 eyes) was attributed to looped vessel leakage at the polypoidal lesion base (fig 10).

Indocyanine green angiography. A polypoidal lesion is seen within abnormal vessel area comprising a vascular network (arrows) (A, 81 seconds, B, 631 seconds).

(A–C) Internal polypoidal lesion structure.

Internal polypoidal lesion structure. Two large vessels, within a polypoidal lesion, show dilatation and constriction. Small vessels apparently form bridge between the two large vessels (A, 14 seconds). Dye leaked from dilated portions of large vessels (B, 27 seconds) accumulates in upper half of the polypoidal lesion (C, 208 seconds).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Four months after fundus photographs in figure 9. Indocyanine green angiography shows disappearance of small bridging vessels (A, 33 seconds). Leakage from dilated portions of looped vessels (B, 35 seconds); consists of ring of hyperfluorescence (C, 1680 seconds).
Pulsation was detected in 24 eyes; in only network vessels in 14, in only polypoidal lesions in five, and in both in five.
DISCUSSION
PCV pathogenesis remains controversial. One proposed mechanism involves CNV, another development of choroidal vasculature abnormalities. We examined the possible contributions of both mechanisms to PCV.
Yanuzzi et al noted that late phase staining characteristic of CNV was not seen in PCV vascular lesions and concluded that branching vascular networks with bordering polypoidal lesions are unique to PCV.6 Moorthy et al concluded that dilated PCV vessels arise from the choroidal vasculature rather than classic CNV.7 Yanuzzi et al also described PCV as a primary abnormality of the choroid.1,8
PCV is not rare in Japan.9–16 As biomicroscopy and ophthalmoscopy indicated PCV vascular abnormalities to lie between the RPE and Bruch’s membrane, Uyama et al concluded that in Japanese patients PCV is a peculiar form of CNV.12 They described lesions termed polypoidal CNV.12 Tateiwa et al described a large vessel variant, expanding across the vascular arcade, in 12 (20%) eyes in a PCV series.13 The dilated vessel network spread radially. Six eyes had subretinal CNV. This large vessel variant appeared to represent CNV, with a worse prognosis than smaller PCV lesions. In a study of 110 PCV eyes, Sho et al noted slow progression of vascular abnormalities and little subretinal fibrovascular proliferation, indicating that PCV has little association with classic CNV.14
Otsuji et al used optical coherence tomography (OCT) to study PCV.15 OCT did not reveal branching vascular network origins, indicating that abnormal vessels in PCV are due to CNV with polypoidal vascular dilatations. They consider PCV to be a type of age related macular degeneration (AMD) with peculiar vascular formations. Iijima et al, using OCT on two PCV eyes, observed polypoidal structures protruding from the inner choroid and speculated that these lesions cause serosanguineous RPE detachments via damage to the overlying Bruch’s membrane and/or RPE, and even adhesion between the two.16
Studying two macular translocation specimens using a light microscope, Terasaki et al identified a fibrovascular membrane within Bruch’s membrane in one eye with PCV.17 Clusters of thin walled dilated vessels correlated with polypoidal structures on ophthalmoscopy and IGA, indicating that the fibrovascular complex was subretinal CNV. However, this eye had previously undergone radiation for a subretinal neovascular membrane, making radiation associated choroidal neovasculopathy a possibility.18
A fibrovascular sub-RPE lesion described by Lafaut et al was also within Bruch’s membrane but beneath the diffuse drusen, contained inflammatory cells and dilated, thin walled vessels, some with very large lumens, suggesting PCV to represent an AMD variant.19 The reliability of surgical specimen studies is often limited by disease severity and/or coexisting disorders.19–21 Secondary histopathological changes cannot be ruled out.
Sub-RPE and intra-Bruch’s membrane choroidal neovascularisation was shown in the peripopillary lesion of an enucleated eye because of angle closure glaucoma.22
Okubo et al used light and electron microscopy, on a surgically excised macular PCV lesion, to identify a degenerated RPE-Bruch’s membrane-choriocapillaris complex.23 An unusually dilated, tortuous venule adjacent to a sclerotic arteriole and two native inner choroid vessels appearing to form an arteriovenous crossing, suggested hyperpermeability, haemorrhage, and sclerosis, at the crossing site, to promote oedema and tissue degeneration. Histopathological similarities with branched vein retinal occlusion were noted. A venule with stasis might become fragile, leading to the beaded or polypoidal configurations of PCV. Vessel pulsation suggested arterial involvement. These findings suggest PCV polypoidal lesions to be inner choroidal vasculature abnormalities.
High speed video IGA with confocal SLO is useful for investigating early vessel filling because high speed images with enhanced contrast show fluid dynamics clearly. With diminished light scattering, detailed internal polypoidal lesion architecture is visualised. We showed network vessel filling begins simultaneously with that of adjacent choroidal arteries. Branching vessels do not represent CNV, based on observation of polypoidal lesions within branching vascular networks. Vessels within networks had tortuous courses, often with constriction and dilatation. Arteries and veins took unusual courses, apparently as a result of disappearing and anastomosing with other vessels. Our findings mirror Yanuzzi et al’s who noted marked morphological variability in abnormal vessels of PCV.24
Pulsation, seen in normal and shunt vessels, is not a feature of CNV, instead indicating arterial involvement and increased intravascular pressure. Pulsation suggests branching network vessels arising from the inner choroidal vasculature. Vessels persisting in networks showed focal dilatation, constriction, and tortuousity. Slow filling early in and dye leakage late in IGA indicated stasis and exudation from branching network vessels. However, there was no late phase hyperfluorescence in eight eyes—that is, leakage from network vessels stops in some cases. Although this probably involves mature vessels, differences between networks with and without hyperfluorescence merit further study.
We observed marked differences in vessel calibre among patients. Yanuzzi et al reported the portion of the choroidal vasculature evolving into PCV networks to vary among patients,6 indicating network vessels to lie at various levels within the choroid.
Polypoidal lesions also presented a spectrum of abnormalities and involved different sized vessels. Clusters of microaneurysmal hyperfluorescent dots indicate small deformed vessels. Polypoidal lesions, apparently resulting from build ups of large deformed vessels, comprised dilated portions of larger tortuous venules. Unusual configurations of vessels the same size as those in branching networks included vascular loops and bead strings. None of our polypoidal lesions showed dilatations at termini of branching network vessels. Like Iijima et al,16 we observed, ophthalmoscopically, reddish orange lesions—that is, polypoidal lesions apparently resulting from serosanguineous RPE detachment caused by exudation from dilated abnormal vessels protruding from the inner choroid.
Lesions with hypofluorescent cores and surrounding hyperfluorescent walls, late in IGA, represent rings of hyperfluorescence.2 Spaide considered dye initially collecting in the polypoidal lesion core and then becoming relatively hypofluorescent with a surrounding hyperfluorescent ring late in IGA, to represent polypoidal lesions resulting from terminal expansion of branching network vessels.2 Kwok et al described the lesion core as becoming hypofluorescent with washout of dye producing a ring silhouette of stained polyps.25 We attributed this finding to morphological abnormalities of polypoidal lesion vessels. As dye intensity fades, leakage from a looped vessel becomes visible as a ring of hyperfluorescence.
Our observations of eyes with typical features suggest that inner choroidal vessel abnormalities may be the pathogenesis of PCV. Taken together, our results and others suggest that PCV is classifiable into three groups. The most common type involves choroidal vasculature abnormalities, in the present narrow sense. A second type is polypoidal CNV, expanding rapidly under the RPE, ultimately with polypoidal lesions developing at vessel termini. Radiation associated choroidal neovasculopathy is the third type.
REFERENCES
Linked Articles
- BJO at a glance