Article Text

Abstract
Aim: To describe the characteristics of babies treated for severe retinopathy of prematurity (ROP) in a tertiary referral unit in China, to provide information to assist in determining screening criteria.
Methods: Information on consecutive babies referred to one eye department for treatment of stage 3 (prethreshold and threshold disease), and stages 4 and 5 ROP between January 2001 and May 2005 were retrieved from medical records.
Results: Data from 114 babies were analysed. The number of babies treated increased from nine in 2001 to 52 in 2004. The numbers of infants in each stage of ROP were as follows: stage 3, 40 babies; stage 4, 19 babies, and stage 5, 55 cases. The mean gestational age (GA) was 29.8 (SD 1.9) weeks (range 26–34 weeks) and the mean birth weight (BW) was 1432 (319) g (range 760–2500 g). 31 babies had BWs more than 1500 g (27.2%). 10 cases (8.8%) had GAs more than 32 weeks, and 82 (71.9%) had GAs more than 28 weeks. Overall, 18 (16.2%) infants exceeded UK screening criteria, and 34 (30.4%) exceeded the criteria used in the United States. The median age at presentation was 5.5 months (range 1–72 months).
Conclusion: Comprehensive screening programmes for ROP are urgently needed in China. Screening criteria recommended by the American Academy of Pediatric Ophthalmology and Strabismus and the Royal College of Ophthalmologists, United Kingdom, may not be suitable for China where bigger, more mature babies are developing severe disease.
- BW, birth weight
- GA, gestational age
- NICU, neonatal intensive care unit
- ROP, retinopathy of prematurity
- retinopathy of prematurity
- gestational age
- birth weight
- infants
- China
- BW, birth weight
- GA, gestational age
- NICU, neonatal intensive care unit
- ROP, retinopathy of prematurity
- retinopathy of prematurity
- gestational age
- birth weight
- infants
- China
Statistics from Altmetric.com
- BW, birth weight
- GA, gestational age
- NICU, neonatal intensive care unit
- ROP, retinopathy of prematurity
- retinopathy of prematurity
- gestational age
- birth weight
- infants
- China
- BW, birth weight
- GA, gestational age
- NICU, neonatal intensive care unit
- ROP, retinopathy of prematurity
- retinopathy of prematurity
- gestational age
- birth weight
- infants
- China
Retinopathy of prematurity (ROP) was a leading cause of blindness in children in North America and Europe during the late 1940s and 1950s.1–4 There is evidence that ROP is currently an important cause of blindness in middle income countries, and is reported from some cities in Asia.5,6 For example, in Thailand and Philippines, ROP was not reported in rural areas but caused 15% of visual loss in cities where better facilities for premature babies are available.7
China is a developing country and neonatal care is expanding and improving. However, the use of unmonitored supplemental oxygen is common, and some babies receive oxygen unnecessarily as they are stable without it. This situation is occurring despite the existence of guidelines on oxygenation policies and practices that were issued by the Ministry of Health in 2004, as a result of lobbying by paediatricians, ophthalmologists, and obstetricians. Oxygen is not used in China to treat ROP. In China parents either pay for neonatal care themselves or the costs are covered by employers.
The importance of screening was only brought to the attention of the medical profession and government in 2004 as a result of lawsuits bought by parents of infants blind from ROP. Before this the majority of paediatricians did not know about ROP, as they seldom saw young children with ROP, and paediatric textbooks usually only mention ROP and do not go into details of prevention or management. Screening programmes are being developed, and training is now available, but screening is not universal owing to lack of skilled personnel.
In industrialised countries screening criteria have been developed based on the characteristics of babies developing ROP who need treatment, and these continue to be reviewed and revised as the population of babies at risk changes over time.8,9 In industrialised countries the mean birth weight (BW) of babies developing severe ROP is in the range 750–800 g, and the mean gestational age (GA) is 25–26 weeks.6 However, there is evidence that babies developing severe ROP in middle income countries have a wider range of BWs and GAs than in industrialised countries, and that screening criteria developed in settings where neonatal care is of high quality may not apply universally.6 There are currently no evidence based guidelines for ROP screening programmes in China, and this retrospective study was undertaken to provide some preliminary data.
Methods and study population
The study was conducted in the People Eye Center, People’s Hospital of Peking University, which is one of the most prestigious eye departments in China. The department is a tertiary referral centre, receiving patients from all over China The department has subspecialty ophthalmology, including paediatrics and vitreoretinal surgery. Data were retrieved on all babies treated for severe ROP between January 2001 and May 2005. In this study, we use the term “severe ROP” to encompass patients treated for prethreshold and threshold stage 3 disease as well as those presenting with stages 4 and 5 ROP. Their medical histories were reviewed and additional information on past medial history and family history was obtained from parents. Data recorded included single or multiple birth, BW, GA, sex, age at attendance at the hospital, and the number of days in oxygen. More detailed information on oxygenation was not available, as these data are not routinely or uniformly collected. The stage of ROP at first operation was recorded: if eyes had a different stage of ROP, the more advanced stage was recorded as stage for the infant. Classification of ROP was done according to the international classification.10
Patients were divided into three groups: group A, threshold and prethreshold ROP; group B, stage 4 ROP; group C, stage 5 ROP. The distribution of BW and GA was analysed for the whole study population and by group. Differences in oxygen exposure, BW, and GA among the three groups were analysed using one way ANOVA analysis. Differences in age at presentation among the three stages were analysed using the Kruskal-Wallis test, and the proportions of the different stages by year were compared by χ2 test. The data were analysed using SPSS, version 10.0.
RESULTS
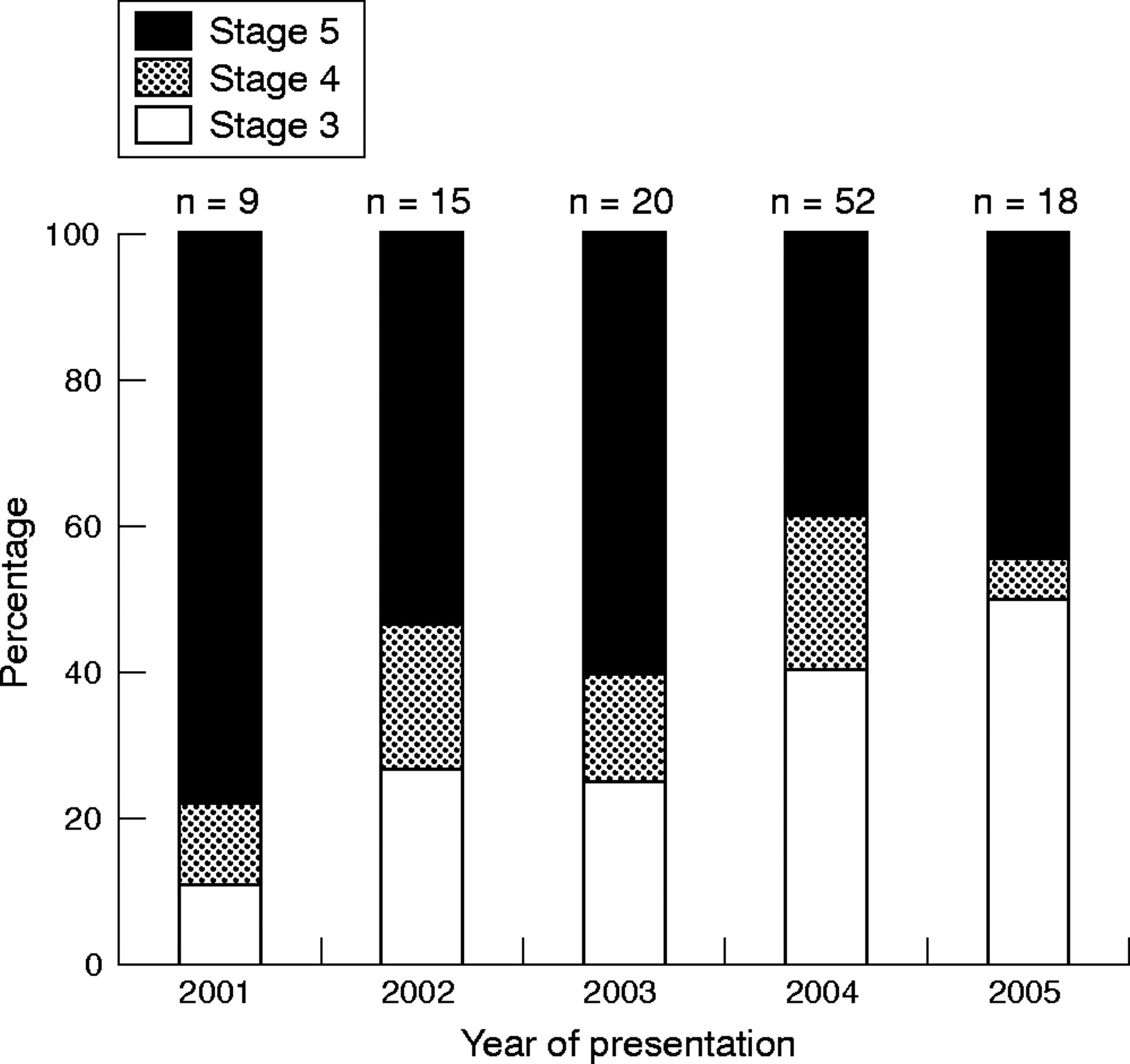
A total of 114 infants were included in the study, 33 of whom were born or cared for in Beijing, and 81 who came from outside Beijing. Only 27 babies had been screened for ROP when still in the neonatal intensive care unit (NICU); 42 of the cases were female (36.8%), 22 were twins (19.3%), and three (2.6%) were triplets. The number of infants and the proportion of the different stage of ROP are shown in figure 1 and table 1. The number of infants presenting increased from nine in 2001 to 52 in 2004, but the proportion with stage 5 shows a non-statistically significant decline over time (table 1). The mean GA was 29.8 (SD 1.9) weeks (range 26–34 weeks) (fig 2). Thirty six infants (31.6%) had GAs of 28 weeks or less, with only four babies having GA of 26 weeks: none had a GA of less than 26 weeks. The BW was unknown in three babies. The mean BW of 111 infants was 1454 (SD 322.8) g (range 760–2500 g) (fig 3). Only seven infants had BWs of less than 1000 g (6.3%): six had BWs in the range 900–999 g, and only one was less than 900 g (760 g). The biggest, most mature baby weighed 2500 g at birth and had a GA of 33 weeks.
The number and percentage of stages 3, 4, and 5 ROP patients in different years

Proportion of different stages of ROP in infants presenting to the People Eye Centre between 2001 and 2005.

Distribution of gestation age in infants with severe retinopathy of prematurity presenting to the People Eye Centre between 2001 and 2005.

Distribution of birth weight in infants with severe retinopathy of prematurity presenting to the People Eye Centre between 2001 and 2005.
Figure 4 shows BW plotted against GA for the 111 babies with BW data. Eighteen babies (16.2%) had BW and GAs exceeding those recommended for screening by the Royal College of Ophthalmologists, United Kingdom (BW<1500 g and/or GA <32 weeks), and 34 babies (30.4%) had BW and GAs exceeding those recommended for screening by the American Academy of Pediatric Ophthalmology and Strabismus11,12 (BW<1500 g and/or GA<28 weeks).

Birth weight and gestational age of infants with severe ROP presenting to the People Eye Centre between 2001 and 2005. Solid lines represent boundary of birth weight and gestational age of screening criteria of Royal College of Ophthalmologists, United Kingdom.
Use of supplemental oxygen was very common (data not available for six infants): only two babies did not receive supplemental oxygen. The mean duration of exposure to oxygen was 19.3 (19.5) days (range 0–120 days). One way ANOVA analysis results showed there was no significant differences in BW, GA, and oxygen use between groups A, B, and C. The median age when patients first visited our hospital was 5.5 months (range 1–72 months) (fig 5). Later presentation was significantly associated with more advanced ROP.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box plot of age of patients with stage 3, 4, and 5 ROP. The difference of age is significant among different stages.
DISCUSSION
This is a hospital based, retrospective study, and there are limitations and biases inherent in studies of this nature. For example, different methods of assessing GA may have been used, but most paediatricians use the last menstrual period, which can be unreliable. The BW data are, however, more likely to be reliable. The People Eye Centre is a tertiary referral centre that receives patients from all over the country, and those presenting to the unit in Beijing may not be representative of all babies with severe ROP in China. Very premature babies may have been too sick to travel to the unit, which would bias the data in favour of more mature babies. Most infants presented because parents noticed leucocoria, or realised that their child could not see well: there are almost certainly other infants and children blind from ROP who have not been identified, and whose BA and GA is therefore not known. However, we believe that the findings of this study provide important indicative information. A prospective, multicentre study is currently under way in which babies will be screened in eight neonatal intensive care units in Beijing. The screening criteria have deliberately been set wide (<34 weeks GA or BW <2000 g), and additional data on risk factors are being collected. Data from this study will be available in 2006.
According to data from blind school studies undertaken in China in 1998 and 2001, ROP currently accounts for only 2–3% of blindness in children in China.13,14 However, as neonatal intensive care services have expanded rapidly since 1992,15 with increasingly premature babies surviving, the incidence of severe ROP is predicted to increase unless comprehensive screening and treatment programmes can be established, covering all units admitting babies at risk. Survival rates of babies in units in 17 provinces of China are currently 43% in babies with BW <1000 g, and 75% in those with BWs of 1000–1500 g.15
Data from a screening programme in the best NICUs in China, in Beijing, have recently reported that approximately 17% of babies who fulfilled the screening criteria outlined above developed different stages of ROP.16,17 Four babies needed treatment; their BWs and GAs were as follows: 29 weeks and 1000 g; 30 weeks and 1130 g; 30 weeks and 1300 g, and 32 weeks and 1380 g. In another unit in Beijing three babies were treated: their BWs and GAs were 29 weeks and 1290 g, and two babies had GAs of 30 weeks and BWs of 1800 g.
In Canada, United States, and United Kingdom, the mean BW and GA of babies with severe ROP is around 750 g and 25 weeks.6 In our study the mean BW and GA is greater than this at 1430 g and 30 weeks, respectively. Our data suggest that the population of babies at risk also differs from babies affected in the middle income countries of Latin America, where an epidemic of ROP blindness is taking place. In these middle income counties the epidemic has been described as the “third epidemic” as the population of babies affected has characteristics of both the first18,19 and second epidemics,20–22 with mean GAs in the range of 26.3–33.5 weeks, and mean BWs in the range of 903–1527 g. The very low number of babies in our study with BWs <1000 g and GAs of <28 weeks suggests a picture more like the first epidemic, when the mean BW of babies with retrolental fibroplasia was 1350 g. There may be many reasons for this first epidemic picture in China, but lack of meticulous monitoring of blood oxygen levels, and high mortality rates in very low BW babies are likely explanations.
The findings of our study have important implications for ROP screening programmes in China, as the criteria from AAPOS11 and the United Kingdom12 almost certainly do not apply, in China bigger, more mature babies are also at risk. In China the screening criteria need to be wider, but this will greatly increase the number of babies requiring examination. The results of the ETROP trial also suggest more frequent examinations of babies with certain stages of prethresold disease, and earlier treatment,23 which will have important resource implications.
After the government issued guidelines on oxygen use awareness of ROP increased and screening is being promoted. Paediatricians are required to use oxygen according to the guidelines, and to inform parents about the need for an eye examination by an ophthalmologist. If screening programmes can be widely implemented, and appropriate criteria adopted, there is the hope that an epidemic of ROP blindness can be averted in China.
Acknowledgments
We gratefully acknowledge the invaluable help of Dr Clare Gilbert (International Centre for Eye Health, Clinical Research Unit, London School of Hygiene and Tropical Medicine) for critically reading and revising this manuscript.
REFERENCES
Footnotes
-
This research is supported by National Basic Research Program of China under the project number 2005CB724307.
-
Competing interests: none declared
Linked Articles
- BJO at a glance
- Editorial