Article Text

Abstract
Aim: To investigate the prevalence of reticular pseudodrusen (RPD) in eyes of patients presenting with newly diagnosed choroidal neovascularisation (CNV) in age-related macular degeneration (AMD), and to analyse the association between RPD, age-related maculopathy (ARM) and AMD.
Method: Two observational consecutive prospective series. In series 1, patients with AMD with newly diagnosed CNV were sampled to determine the incidence of RPD. Eyes with and without RPD were compared by the Mann–Whitney non-parametric test and Fisher’s exact test for age, sex of patients, the eye involved and type of CNV. Series 2 comprised 100 patients referred for fundus photography, fluorescein and/or indocyanine green angiography, for whom pictures showed RPD. This second cohort was then selected from a larger group of patients.
Results: Patients with newly diagnosed CNV in series 1 comprised 67 women and 33 men, aged 57–96 years (mean 79.5). CNV was “classic” (32 eyes), “occult” (41) or exhibited vascularised pigment epithelial detachment (PED, 11), retinal angiomatous proliferation (RAP) with or without PED (13), or haemorrhagic or fibrovascular scarring (3). In all, 24 (24%) eyes had RPD. The prevalence of RAP was significantly higher in eyes with RPD than in those without (p = 0.0128), despite the small number of patients with RAP. In series 2, 100 patients with RPD were enrolled in 3 months, and corresponded to 8% of the overall cases referred to our centre (Centre Ophtalmologique d’Imagerie et de Laser, Paris, France). There were 77 women and 23 men, aged 54–93 years (mean 79.2). Eyes with RPD (n = 155) usually exhibited signs of ARM or AMD, including soft drusen (101 eyes) and/or retinal pigment epithelium abnormalities (70), geographical atrophy (27) and/or CNV (61). In both studies, examination of blue-light fundus pictures was extremely helpful in diagnosing RPD.
Conclusion: RPD have a high prevalence among patients with AMD with newly diagnosed CNV (24% of cases). RPD were commonly associated with ARM or AMD. This study suggests that eyes with RPD could be classified as a phenotype of ARM.
- AMD, age-related macular degeneration
- ARM, age-related maculopathy
- CNV, choroidal neovascularisation
- ICG, indocyanine green
- PED, pigment epithelial detachment
- RAP, retinal angiomatous proliferation
- RPD, reticular pseudodrusen
Statistics from Altmetric.com
- AMD, age-related macular degeneration
- ARM, age-related maculopathy
- CNV, choroidal neovascularisation
- ICG, indocyanine green
- PED, pigment epithelial detachment
- RAP, retinal angiomatous proliferation
- RPD, reticular pseudodrusen
In 1990, Soubrane described a particular yellowish pattern in the fundus of patients with age-related macular degeneration (AMD) and noted that this pattern was clearest on red-free or blue-light fundus pictures (fig 1).1,2 The pattern was termed “les pseudodrusen visibles en lumière bleue”, meaning “pseudodrusen visible with blue light”. The Beaver Dam Eye Study by Klein et al3 included this pattern in its age-related maculopathy (ARM) grading system under the name “reticular drusen”. The most important clinical and histological study specifically concerning reticular pseudodrusen (RPD) was published in 1995 by Arnold et al.4 In this study, RPD were attributed to changes in the choroid, thus the term “pseudodrusen” has been used in most studies. Furthermore, pseudodrusen were considered a risk factor for AMD. This latter assertion was controversial because there was no control group in the study by Arnold et al.5 The known data can be summarised as follows: RPD are usually associated with ARM4 and usually bilateral.6 In some series, they were found mixed with soft indistinct drusen and were considered to be often complicated by choroidal neovascularisation (CNV).7,8 RPD are undetectable (silent) by fluorescein angiography, except for an uneven choroidal filling, and are hypofluorescent on midphase and late-phase indocyanine green (ICG) angiography using scanning laser ophthalmoscopy.9 However, despite these studies, they are an under-reported retinal phenotype, and have not been recognised specifically in the international classification of AMD.10 Furthermore, to date, there is no histological study suggesting exactly to which lesion the typical clinical pattern of RPD corresponds.

Reticular pseudodrusen (RPD). Colour (A), red-free (B) and blue filter (C) fundus photographs; early (D) and late (E) frames of the fluorescein angiography of a patient with age-related maculopathy characterised by macular pigmentary changes. RPD are barely visible on the colour picture (A), more clearly visible on the red-free picture (B) and clear on the blue filter picture (C), on which they form a lacy pattern located outside the macula, near the temporal vessels. On fluorescein angiography, a patchy choroidal filling is present (D), but RPD are silent (D,E).
This study was undertaken to define the prevalence of RPD among patients with AMD with newly diagnosed CNV, and to analyse the relationships between RPD and various characteristics of ARM and AMD.
PATIENTS AND METHODS
Two series of 100 patients each were recruited in a tertiary care centre (Centre Ophtalmologique d’Imagerie et de Laser, Paris, France) specialising in the diagnosis and treatment of AMD. Institutional review board and ethics committee approval was obtained. Two studies (one for each series) were conducted simultaneously.
The first study consisted of the prospective collection of data and fundus photographs for 100 consecutive patients referred for AMD complicated by CNV. All patients had 50° red-free and blue-light pictures of the fundus. In France, these pictures are part of routine fluorescein or ICG angiography.11,12 Blue-light pictures are obtained using the blue excitation filter without the barrier filter of the fundus camera. All pictures were taken with a 50IA fundus camera (Topcon, Tokyo, Japan) and processed with the Ledioph 2k2 image processing system (Lheritier, Cergy-Pontoise, France). The analysis of pictures was performed by two independent medical retina specialists (SYC and GQ). There was no formal grading of the number or surface of the drusen. The analysis was limited to the presence or absence of soft drusen, RPD, geographical atrophy (>0.5 disc diameter) and the type of CNV. In cases of disagreement, the pictures were reviewed by both observers for discussion and final classification. After the series had been constituted, the 100 cases were divided into two groups, respectively, with and without RPD. The groups were compared for age, sex, eye involved and type of CNV by the Mann–Whitney non-parametric test and Fisher’s exact test.
The second study consisted of the prospective collection of 100 patients with various pathologies, referred for fundus photography, fluorescein and/or ICG angiography, for which pictures showed RPD. This second cohort was then selected from a larger group of patients, corresponding to patients referred to our centre. In France, fluorescein angiography is performed for exudative AMD and follow-up of eyes treated by laser or photodynamic therapy, and diagnosis of vascular, inflammatory, degenerative or tumoral disorders of choroids and retina. Management of diabetic retinopathy is also often based on results of fluorescein angiography. No attempt was made to analyse the cohort of patients referred to our centre during this study. Pictures were taken with a 50IA fundus camera (Topcon) and processed with a Ledioph 2k2 image processing system (Lheritier). After the series had been constituted, demographic characteristics were recorded, and fundus findings such as presence of soft drusen, retinal pigment epithelium pigmentary abnormalities, geographical atrophy and CNV, related to ARM and AMD, were given by two assessors, as described above. No attempt was made to record demographic data that could be associated with AMD, such as smoking or body mass index.
RESULTS
Series 1
The patients with AMD with newly diagnosed CNV comprised 67 women and 33 men, aged 57–96 years (mean 79.5). Results are expressed as mean (standard deviation (SD)). The Mann–Whitney non-parametric test was used to compare the statistical distribution of parameters measured. Fisher’s exact test was used for categorical variables. No significant difference was noted between patients with and without RPD with regard to age, sex or eye involved (table 1).
Series 1: comparison between patients with and without reticular pseudodrusen
The types of CNV were “classic” or “predominantly classic” for 32 eyes, “occult” or “minimally classic” for 41, characterised by vascularised pigment epithelial detachment (PED) for 11 eyes, by retinal angiomatous proliferation (RAP) with or without associated PED for 13, and by a haemorrhagic or fibrovascular scar for 3. In all, 24 (24%) of the 100 eyes presented with RPD (table 2).
Series 1: subtypes of CNV and other conditions in eyes with and without reticular pseudodrusen
In eyes with RPD, CNV was “classic” or “predominantly classic” for 7 eyes (fig 2), and “occult” or “minimally classic” for 9. Other conditions were vascularised PED for 1 eye (fig 3), and RAP with or without associated PED for 7 eyes (fig 4). In eyes without RPD, CNV was “classic” or “predominantly classic” for 25 eyes, and “occult” or “minimally classic” for 32. Other conditions were vascularised PED for 10 eyes, RAP with or without associated PED for 6, and haemorrhagic or fibrovascular scar for 3.
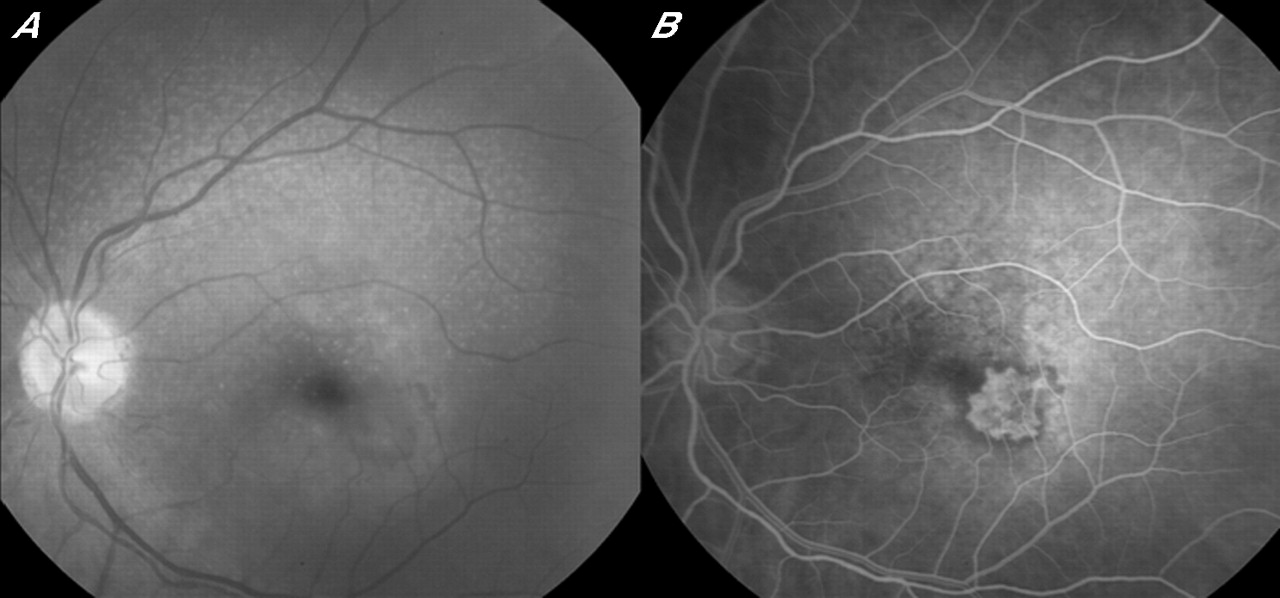
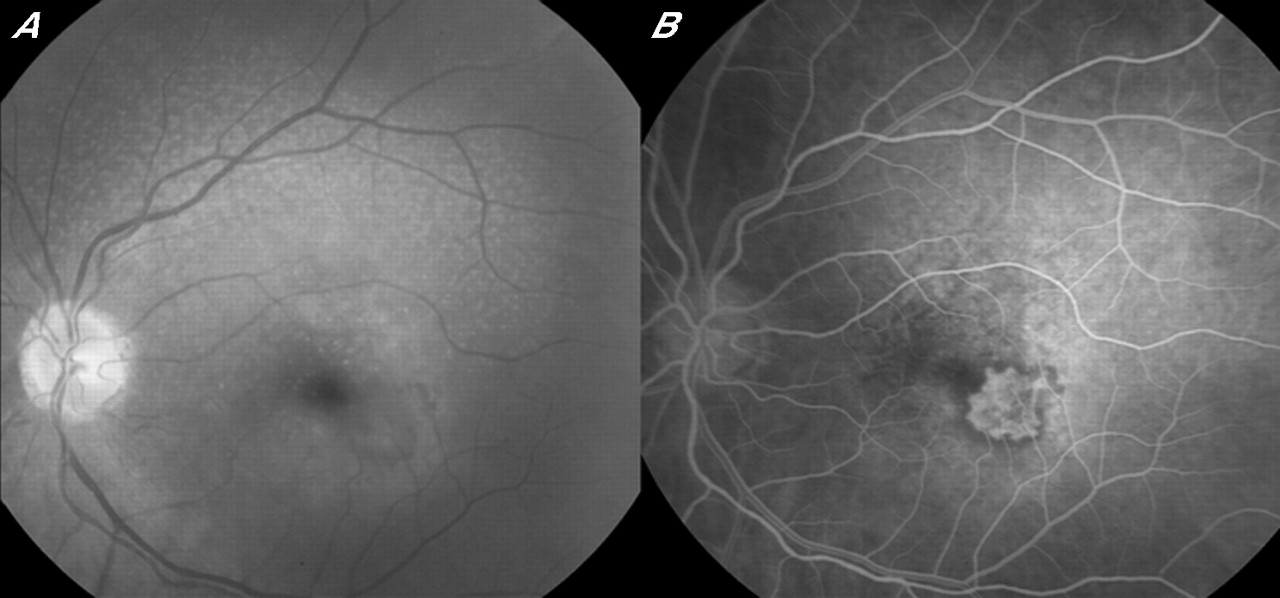
Reticular pseudodrusen (RPD) associated with classic choroidal neovascularisation. Blue filter fundus photograph (A) and fluorescein angiogram (B). The lacy pattern is clearly visible on blue filter photograph (A). Juxtafoveal classic neovscularisation (B). The presence of RPD cannot be detected on the fluorescein angiogram.

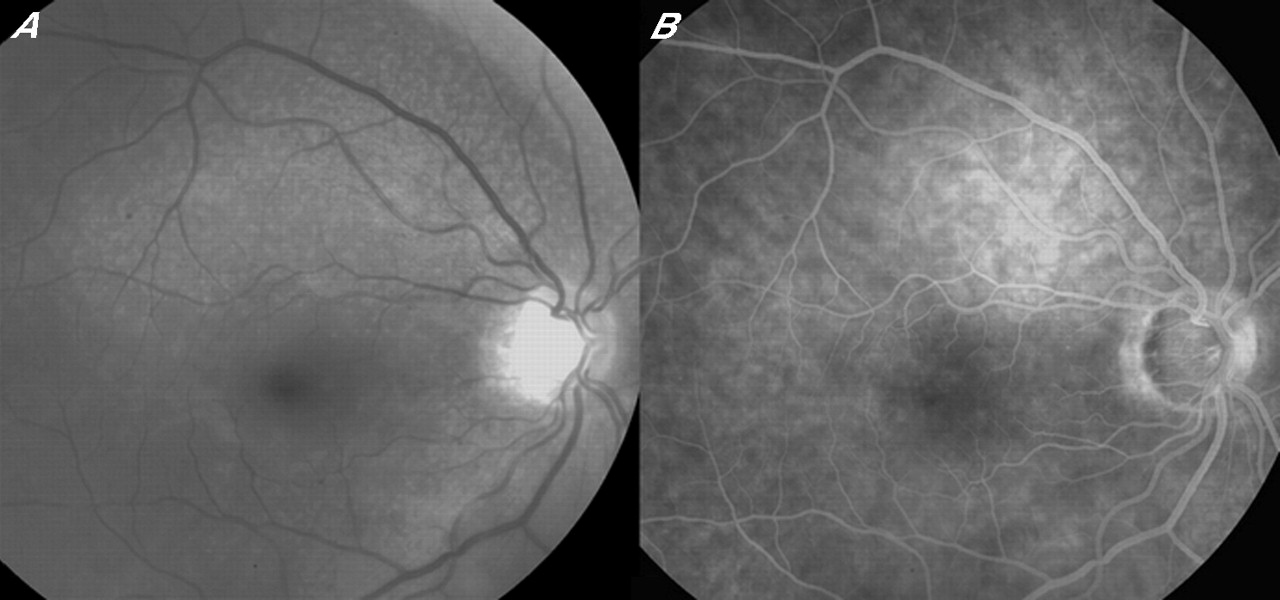
Reticular pseudodrusen (RPD) associated with vascularised pigment epithelial detachment (PED). Blue filter fundus photograph (A) and fluorescein angiogram (B). Note the presence of an area of RPD around the superior temporal vessels (arrows). Fluorescein angiography shows macular choroidal neovascularisation with a temporal PED.

Reticular pseudodrusen (RPD) associated with retinal choroidal anastomosis or retinal angiomatous proliferation (RAP). Blue filter fundus photograph (A) and fluorescein angiogram (B). RPD are visible in the upper part of the macula (A). On the fluorescein angiogram (B), the temporal haemorrhage (A) corresponds to RAP, located in the temporal part of the macula (arrow).
The prevalence of RAP in eyes with RPD was significantly higher than in eyes without.
Series 2
The 100 patients with RPD were recruited in a 3-month period. During this period, 1874 patients were examined by fundus photography, fluorescein angiography and/or ICG angiography, for various reasons. The 100 patients comprised 77 women and 23 men, aged 54–93 years (mean 79.2). RPD was observed in one eye in 45 patients, and in both eyes in 55 others. Thus, 155 eyes with RPD were studied. Signs of ARM or AMD were observed in 144 (92.9%) of these eyes. More precisely, soft drusen were observed in 101 eyes, retinal pigment epithelium pigmentary abnormalities in 70, geographical atrophy in 27 (fig 5) and exudative AMD in 61. Five eyes exhibited deposits similar to those occurring in vitelliform macular dystrophy. Six eyes (3.8%) exhibited no signs of ARM, AMD or macular deposits (fig 6). One eye exhibited collateral vessels suggestive of previous branch vein occlusion.

Reticular pseudodrusen (RPD) associated with geographical atrophy. Blue filter fundus photograph (A) and fluorescein angiogram (B). RPD are associated with soft calcified drusen (A). Geographical atrophy can be seen around the fovea (B).

Isolated reticular pseudodrusen (RPD). Blue filter fundus photograph (A) and fluorescein angiogram (B). In some eyes, RPD were observed without any signs suggestive of ARM or AMD.
DISCUSSION
There are many classifications of drusen.13–15 In this paper, ARM and AMD were defined as suggested by the International ARM Epidemiological Study Group.10 RPD have not been included in all the epidemiological studies of ARM and AMD. Furthermore, they are not specifically recognised in the international classification of AMD.10 In an important epidemiological study,3 drusen were classified as reticular when they formed ill-defined networks of broad interlacing ribbons. This type was classified as a specific kind of drusen, graded separately from soft drusen, whether distinct or indistinct. However, in a subsequent study by the same authors, corresponding to the 5-year analysis of their study, they were mixed with indistinct soft drusen.7 According to its authors, eyes with soft indistinct drusen were more likely to develop late AMD than those without AMD (6.5% v 0.1%). In the Blue Mountains Eye Study, eyes with indistinct soft or reticular drusen were more likely to develop neovascular or atrophic AMD lesions (23.2% v 0.4%), and the relative risk was 9.9.8 However, the specific risk of reticular drusen was not reported in either of these studies. Moreover, in the Choroidal Neovascularization Prevention Trial, RPD were specifically investigated but were rare, as they were observed in only 3 three of 121 eyes with CNV. Thus, in this study, RPD were not considered to be a major determinant in the development of CNV.16
The present study was specifically designed to explore RPD. They were frequent in eyes with newly diagnosed CNV (24% of cases). All types of CNV were found, but the prevalence of retinal choroidal anastomosis or RAP was higher than for other types. The results of the statistical analysis should be taken with caution, because we have undertaken multiple analyses on the same dataset. Furthermore, the number of patients with RAP is probably too small for definite conclusion because the significance level becomes dependent on the classification of RPD in one or two patients. The pathogenesis of RAP is controversial, particularly in its early stages. Intraretinal proliferation followed by retinal choroidal anastomosis has been suggested by some authors, 17,18 but was challenged by others.19,20 Our study was not designed to answer this question. On the basis of present knowledge, we have no explanation for the high incidence of RAP in patients with RPD. We can only suggest that in future studies of RAP, red-free or blue-light pictures should be carefully examined for the presence of RPD.
In the study by Arnold et al,4 3 years were needed for the retrospective collection of 100 RPD cases, whereas only 3 months were needed in this study. The difference is probably due to systematic taking of red-free and blue-light fundus pictures before fluorescein or ICG angiography advocated in France.11 The study of blue-light pictures has been considered very useful for examining the retinovitreal interface.21,23 RPD were more clearly visible in blue-light than in red-free or colour pictures, which may have caused their underestimation in studies in which these pictures were not taken. In fact, RPD may not be visible on colour pictures, but might be obvious on blue-light pictures (fig 7), as reported when they were first described.1,2 The examination of blue-light pictures has probably improved the rate of diagnosis. Fundus autofluorescence performed with confocal scanning laser ophthalmoscopy may be of value in diagnosis of RPD. Lois et al reported a reticular pattern of autofluorescence outside the macula, near the temporal vessels, which could correspond to RPD, but their study did not include red-free or blue-light pictures of the fundus.24 We suggest that future studies on RPD use colour, red-free, blue-light pictures and also autofluorescence to improve their diagnosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Colour (A) and blue filter fundus photograph (B). RPD may be missed on the colour photograph, but are obvious on the blue filter fundus photograph (arrows).
Another possible explanation for underestimation of pseudodrusen is that, in many studies, the Wisconsin 9-field grid3 was used to grade drusen, but RPD are often located outside the outer fields of the grid, near the temporal vessels. This may explain why RPD have been previously considered as rare in patients with CNV.16
Signs of ARM or AMD are usually present with RPD, as observed in 92.9% of our cases. They were constantly present in the study by Arnold et al.4 Because RPD are often observed in patients with newly diagnosed CNV complicating AMD and may occur without any other signs of ARM, our results suggest that they could be classified as a phenotype of ARM. However, a prospective follow-up of eyes with RPD without other signs of ARM is needed to assess whether these eyes are at risk of CNV or geographical atrophy.
REFERENCES
Footnotes
-
Published Online First 13 September 2006
-
Competing interests: None.
-
Presented in part at the Macula Society 29th Annual Meeting, San Diego, California, USA, February 2006, and at the American Academy Annual Meeting, Las Vegas, Nevada, USA, November 2006.