Article Text

Abstract
Background/aims: This is a long-term follow-up report investigating primary transpupillary thermal therapy (TTT) for choroidal melanoma.
Methods: Retrospective case series of 135 patients harbouring choroidal melanoma treated with primary TTT. Patient demographics, tumour characteristics, treatment responses and complications, visual acuity outcomes and mortality data were captured and reported. A statistical analysis was performed for predictors of treatment failure.
Results: Successful tumour regression was achieved in 76% of patients. Of the 32 patients who failed, 12 had enucleation, and 20 had irradiation. Metastatic disease has occurred in three patients, and two patients have died (3/135, or 2%). Multivariate analysis determined that tumour diameter, tumour thickness greater than 3 mm and tumours exhibiting high-risk characteristics were significant predictors of failure. Patient age, gender, number of treatments and proximity of the tumour to the disc or fovea were not predictive of failure. Kaplan–Meier cumulative probability predicted a 19% 5-year treatment failure and 33% 10-year treatment failure. Treatment failure occurred as late as 99 months. Final visual acuity was 20/40 or better in 50% of patients; 32% had a final visual acuity of 20/200 or worse. Thirty-two per cent of patients developed one or more complications as a result of the TTT, the most concerning of which was intra- or extrascleral extension of tumour (occurring in 11 patients).
Conclusions: Though not as successful as radiation therapy, TTT successfully induced regression in 76% of patients. TTT may still have a role in our treatment paradigm but should probably be reserved for specific cases, such as monocular patients with tumours near critical visual structures, surgically unstable patients or patients with advanced diabetic retinopathy. All patients considering TTT as monotherapy for choroidal melanoma must be selected, counselled and followed appropriately.
Statistics from Altmetric.com
With a yearly incidence of 4.9–7.6 cases per million people, uveal melanoma will be diagnosed in approximately 1500 Americans annually.1 Treatment options depend on factors such as the affected eye’s visual acuity and intraocular pressure, the tumour location, size and growth rate, the patient’s age and general health, and the status of the fellow eye.2 Depending on these factors, today clinicians have a variety of treatments to offer patients, including observation, laser photocoagulation, thermal therapy, radiation, local excision and enucleation.
Infrared laser thermal therapy has been coined transpupillary thermal therapy (TTT). It may be particularly useful for tumours within 5 mm of the fovea or optic disc, where radiation would result in potential vision loss. Experimental studies show that thermal penetration of the tumour reaches a maximum of 4 mm in depth, thereby making it a potentially ideal treatment option for small choroidal melanomas.3 TTT as a treatment alternative for small choroidal melanoma was used extensively in the mid- and late 1990s, but gradually appears to be falling from favour due to treatment failures. However, there are few studies that report long-term outcomes in patients treated with primary TTT. The purpose of this report is to describe our experience with TTT for choroidal melanoma beginning in 1996.
METHODS
This is a retrospective case series conducted on all patients managed with primary transpupillary thermotherapy for choroidal melanoma at the Emory Eye Center from 1996 to 2002 and at Associated Retinal Consultants from 2001 to 2005. With appropriate IRB approval, ultrasound and laser log records and ICD-9 coding were used to identify eligible patients. Patients were only included in this analysis when the primary intention was to treat the choroidal lesion with thermal therapy alone. Any patient treated with combination thermotherapy and radiation therapy was excluded. All eligible patients had a baseline exam performed with clinical assessment, diagnostic ocular echography and fundus photography. The treatment method (TTT, radiation therapy or enucleation) was discussed with the patient preoperatively. Using the information available at the time of the discussion regarding treatment success and short- and long-term complications, a collective decision was made with the patient as to which treatment option to pursue.
The data collected for this review included patient demographics, tumour parameters, tumour location and characteristics, pretreatment and final best corrected Snellen visual acuity, indications for treatment, number of treatments, treatment complications, tumour response to treatment/failures, length of follow-up, time to treatment failure, and all-cause mortality and tumour-related mortality. The patient demographics included patient age, sex and race. Indications for treatment were based on high-risk characteristics (thickness >2 mm, subretinal fluid, orange pigment, symptoms or tumour at the disc margin), expanding lesions documented by clinical photographs or ultrasound, or lesions greater than 3 mm. Using the Collaborative Ocular Melanoma trial’s initial standards, a tumour greater than 3 mm was considered to be a medium-sized melanoma, and tumours 3 mm or less were considered small. Tumour response to treatment was a flat chorioretinal scar or a stable regressed tumour with minimal elevation. Failure was defined as tumour recurrence (documented expansion of tumour base or thickness) requiring enucleation or radiation treatment. The mean and standard deviation are reported as mean (SD). The cumulative probability of failure as a function of time from laser treatment was determined using the Kaplan–Meier method. The relationship between time to failure and patient characteristics was assessed using Cox proportional hazards regression. The percentages of patients with final vision better than 20/200 were compared among categories for each of the patient characteristics using a chi-square test with pairwise comparison done using the Tukey procedure.
Transpupillary thermal therapy was performed with an 810 nm wavelength laser delivered via a slit-lamp biomicroscope. The eye was anaesthetisised with a retrobulbar or peribulbar block. Laser was applied using a fundus contact lens. Each spot was 2–3 mm in diameter and 1–2 min in duration. Power began at 500 mW and was either incrementally increased or decreased until the optimal power level was achieved. The optimal power level resulted in opacification of the tumour and overlying retina beginning at 40 s into a 1 min treatment spot, and ended with modest whitening at the conclusion of 1 min. Overlapping confluent spots were placed over the entire tumour and extended 500–1000 µm into normal choroid.
Patients were seen every 2 months after treatment until a flat chorioretinal scar was achieved. All follow-up, visits included clinical examination, echography and photography. If regression was confirmed, no further treatment was performed. Once a flat chorioretinal scar was achieved, patients were seen every 4 months for 1 year, and then every 6 months. Tumours failing to achieve a flat chorioretinal scar were treated with additional thermotherapy at the discretion of the treating physician.
If recent follow-up was not documented in the patient chart, the patient, a family member or the referring physician was contacted for follow-up information. Mortality data were collected through the chart review.
RESULTS
One hundred and thirty-five patients with choroidal tumours felt to represent melanoma were treated; 78 female (58%) and 57 male (42%). The mean age was 60.2 (14.0) years (range 20 to 89 years). Of the 135 eyes, 70 were right (54%), and 65 were left (46%). The mean tumour thickness was 2.2 (0.9) mm (range 0.25 to 6.6 mm). Eighty-eight per cent (119) of tumours were small melanomas, and 12% (16) were medium melanomas (fig 1). The mean maximum base diameter was 8.5 mm (range 2.8 to 13.8 mm). The mean thickness was 2.3 mm (range 0.25 to 6.6 mm). The mean number of TTT treatment sessions was 1.8 (range 1 to 7), with 69 patients (51%) receiving one treatment, 40 patients (30%) receiving two treatments and 26 patients (19%) receiving three to seven treatments. Indication for treatment was documented growth in 73 patients (54%), tumour thickness greater than 3 mm in 17 patients (13%) and high-risk characteristics (including subretinal fluid, orange pigmentation and a tumour thickness of ⩾2 mm) in 29 patients (21%). Sixteen patients (12%) did not have a defined indication for treatment. The mean time from TTT to treatment failure or last follow-up was 4.7 (3.3) years (range 2 months to 14.9 years).

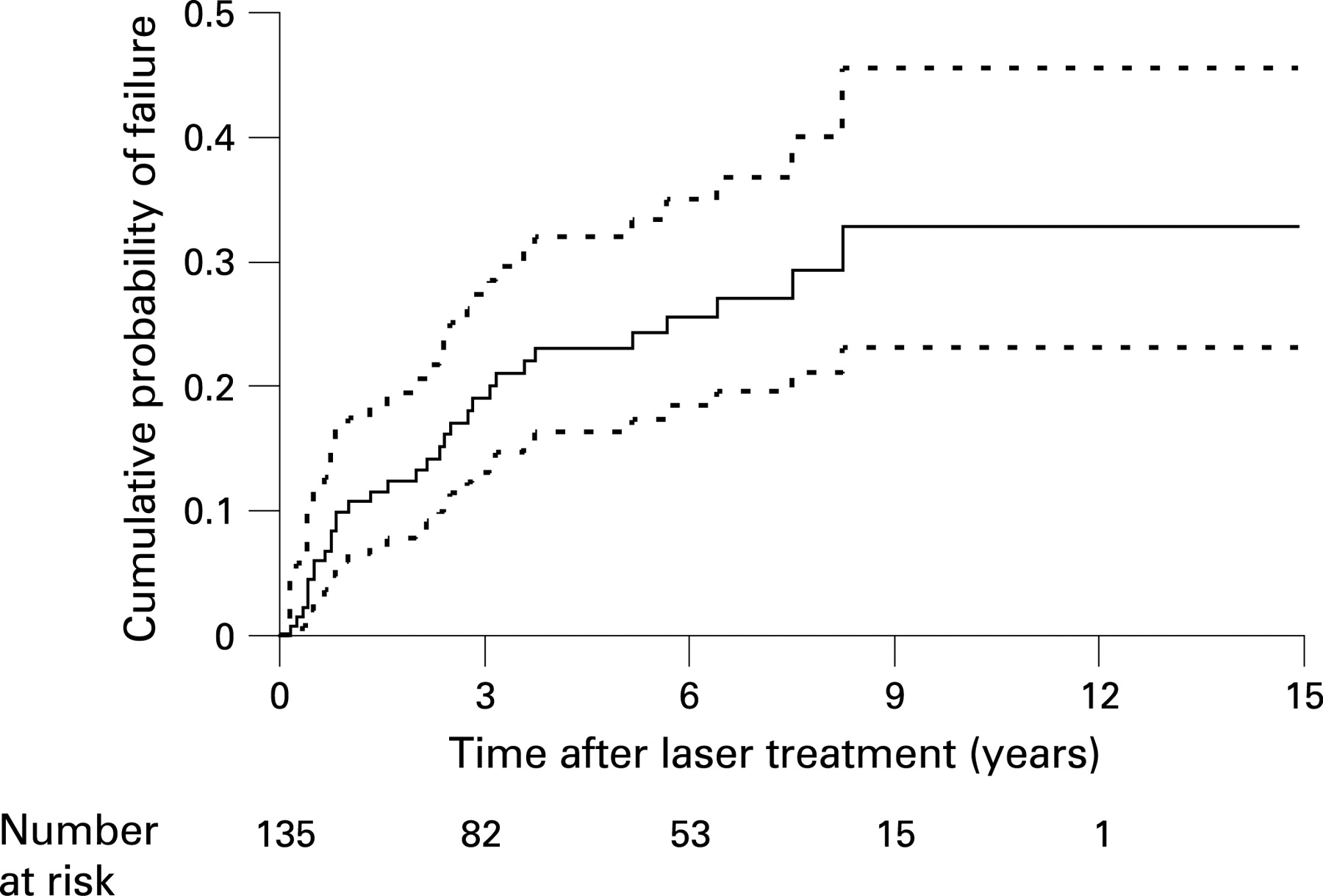
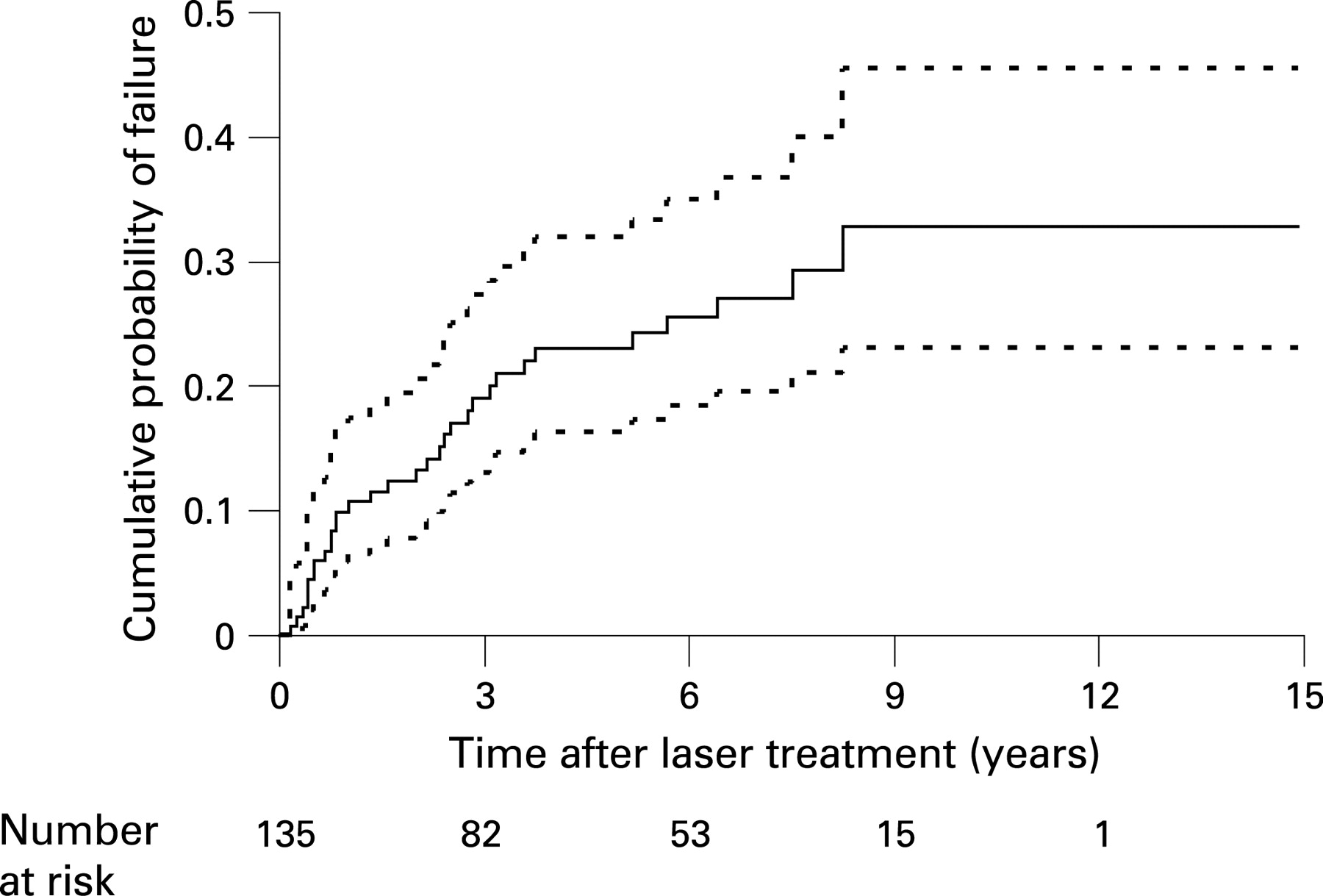
Successful tumour regression was achieved in 103/135 patients (76%). Of these 103 patients, 70 (68%) had flat chorioretinal scars, and 33 (32%) had minimally elevated stable tumours. Of the 32 patients (24%) that failed primary TTT, 12 were treated with enucleation, 19 underwent brachytherapy, and one underwent proton beam irradiation. The chance of treatment failure was 11% at 1 year, 23% at 5 years and 33% at 9 years (fig 2). Treatment failure occurred as long as 8.25 years after TTT.
A univariate analysis using Cox proportional hazards regression showed that patient age, gender and number of TTT treatments did not differ significantly between successful and failed treatment groups. However, the maximum tumour base diameter at initial presentation greater than 10 mm, tumour thickness on initial presentation greater than 3 mm, tumours exhibiting high-risk characteristics and tumours touching the optic disc were shown to be significant predictors of failure (p<0.05) (table 1).
Interestingly, if tumour height on initial presentation is analysed at ⩽2 mm, the failed and successful treatment groups are not significant, but there is a strong trend toward significance. Twelve (18%) of the 67 patients with tumour height on initial presentation less than 2 cm failed, compared with 20 (29%) of the 68 patients who presented with a tumour height greater than 2 mm (hazard ratio = 2.0, p = 0.052).
A multivariate Cox proportional hazards regression model showed high-risk characteristics (hazard ratio = 3.9, 95% CI = 1.9 to 8.1, p = 0.0002) and tumour base maximum greater than 10 mm on initial presentation (hazard ratio = 2.9, 95% CI = 1.4 to 6.0, p = 0.005) to be significant predictors for failure with a trend toward significance for tumour height on presentation greater than 2 mm (hazard ratio = 1.9, 95% CI = 0.9 to 4.0, p = 0.082), but contact with the optic disc was not significant.
Since some groups might have a lower rate of failure because they were observed for a shorter duration of time, the follow-up time among the indication for treatment groups was evaluated. The length of follow-up time for patients who had not failed among the four indication-for-treatment groups was compared. The results are shown in table 2. The group with the lowest failure rate, observed growth 14%, had the longest mean length of follow-up for patients who had not failed. Therefore, the reason for a lower failure rate in that group cannot be that the patients were followed for a shorter duration of time.
The p value for an F test based on an analysis of variance model which compares the mean time among all four groups = 0.029, indicating that the means of at least two of the groups are statistically significantly different. The Tukey multiple comparison procedure suggests that the mean times for the growth and >3 mm groups are significantly different.
The all-cause mortality in this series was 9% (12/135 patients). Two patients have died with metastatic melanoma, and one patient is alive with metastatic disease; a melanoma-specific mortality of 2% with a mean of 4.7 years of follow-up. Of the three patients in our series with metastatic disease, one patient had TTT once, was considered a failure and was enucleated 10 months later. The second patient had TTT twice, was last seen in August 2001 with a tumour measuring 1.2 mm in thickness, never returned for follow-up and died in April of 2006. The third patient had TTT four times, was deemed a failure and plaqued 34 months after initial TTT. This patient was diagnosed as having metastatic melanoma 6 years later.
Of the 135 patients, the initial visual acuity was 20/40 or better in 103 patients (76%) and 20/200 or worse in 11 patients (8%) (table 3).
Of 132 patients with a final visual acuity available, 67 (51%) were 20/40 or better, and 43 (32%) were 20/200 or worse, including all the patients who were enucleated. A statistical analysis was performed, comparing the percentage of patients who achieved better than 20/200 acuity per characteristic listed in table 1. The results tabulated in table 4 demonstrate that the location of a tumour touching or involving the fovea has a statistically significant higher number of patients with vision 20/200 or worse (p<0.0001). Pairwise comparisons showed that the observed growth group and the high-risk group were also significantly different (p<0.05).
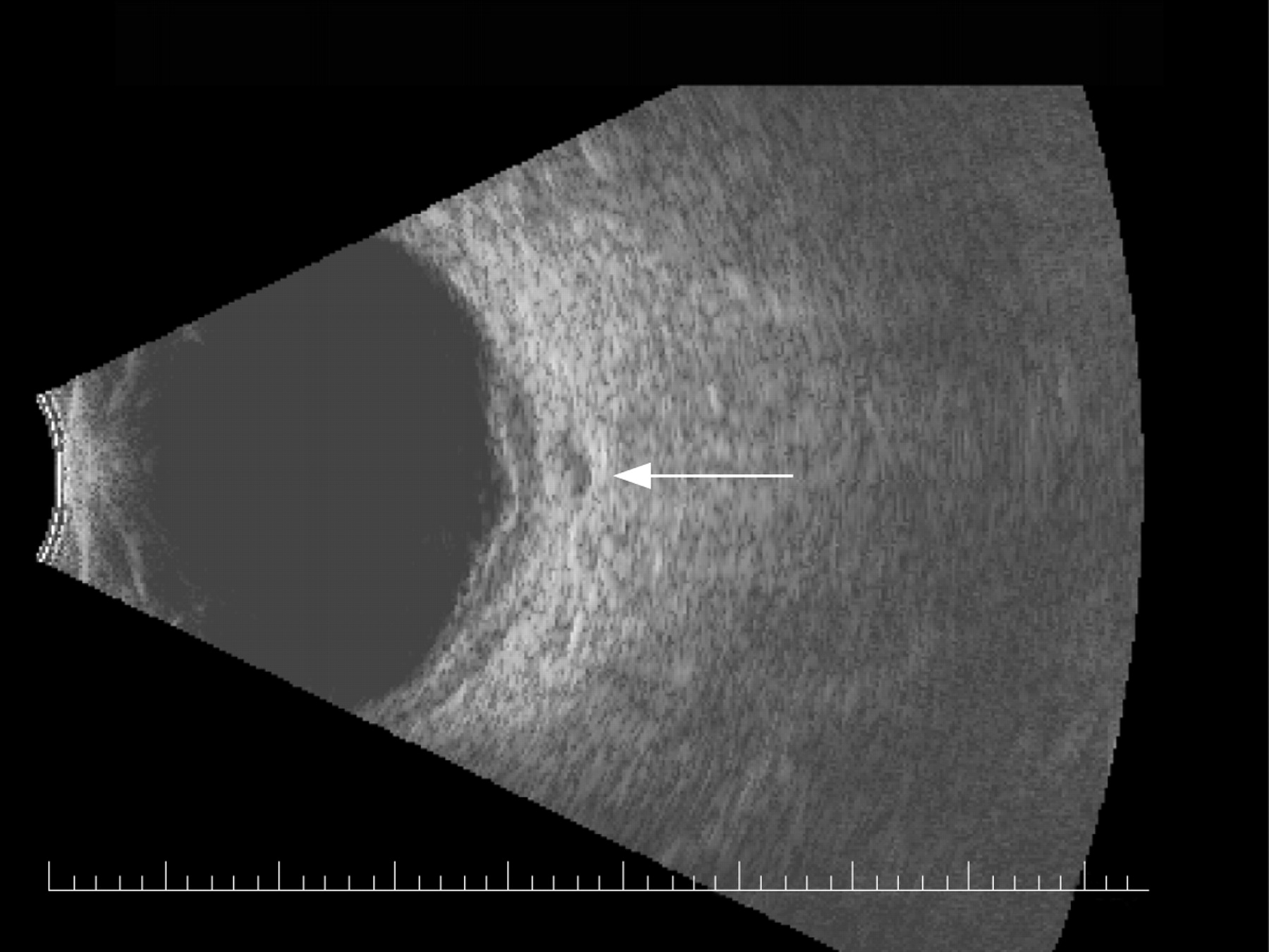
Forty-three of the 135 (32%) patients experience at least one complication. Thirty-four patients had one complication, and nine patients had two complications. A macular pucker occurred in 15 patients, a vascular occlusion occurred in 13 patients, cystoid macular oedema (refractory to topical medications, subtenons triamcinolone or intravitreal triamcinolone) occurred in seven patients, a macular hole developed in two, a vitreous haemorrhage developed in two, a rhegmatogenous retinal detachment developed in one, and an exudative retinal detachment developed in one patient. Seven patients developed intra-scleral tumour extension, and four developed extra-scleral tumour extension typically along emissary canals (fig 3).
DISCUSSION
Reported choroidal malignant melanoma response rates after primary TTT range from 91% to 97%.4–8 Shields et al reported their experience in 256 patients treated with primary TTT for choroidal tumours.4 These choroidal tumours were felt to be choroidal melanoma based on growth (45%) or high-risk features for growth (55%). Of these patients, 232/256 (91%) achieved complete tumour control with a mean follow-up of 19 months (range 2 to 52 months). Two patients (1%) developed metastatic melanoma. One of these had complete tumour regression after TTT alone, and the other had diffuse choroidal melanoma and local tumour margin recurrence. Given that the mean time to recurrence (22 months) was greater than the mean follow-up period (19 months), Kaplan–Meier estimates were calculated to predict long-term tumour recurrence rates. This statistical analysis predicted a 22% recurrence rate at 3 years. Win et al reported their results in 40 patients with small choroidal melanocytic tumours treated with TTT and followed on average for 42 months.9 No recurrences were noted in 77.5% of patients. The mean interval between TTT and failure was again 22 months, ranging from 7 to 30 months. One eye developed an extrascleral extension. No metastatic disease was reported.
This study corroborates earlier reports, and illustrates several important findings. Twenty-four per cent of patients were considered primary TTT failures, requiring enucleation or irradiation, within a mean follow-up period of 4.7 years (range 2 months to 14.9 years). In 76% of cases, TTT successfully induced tumour regression. However, of those 103 patients, only 68% achieved a flat chorioretinal scar (52% of the entire cohort). The remaining 32% regressed but had residual stable tumours. Stable residual tumours may represent successful regression, or these tumours may be viable but have yet to expand sufficiently for detection. We are concerned that these 33 cases represent the latter. This concern is supported by the number of late recurrences that have occurred. On average, the time from initial TTT to recurrence was 29 months and occurred as late as 8.25 years after initial TTT (fig 4A–C).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tumour recurrence occurred primarily along the treatment margin, or within the sclera. Prior radiation studies have clearly demonstrated that recurrent tumour growth is a predictor for metastatic disease.10–12 One would anticipate similar results in TTT patients. So, are we exposing our patients to an increased risk of metastatic disease? With a mean of 4.7 years of follow-up, the all-cause mortality in this series was 8%, and the melanoma-specific mortality was 2%. This rate of melanoma-specific mortality is similar to reports of patients harbouring small tumours treated with irradiation. For example, in a 2005 report, Sobrin and colleagues had a 5-year melanoma-specific mortality of 3.9% in 45 patients with small choroidal melanoma who were followed for growth or development of orange pigmentation and subsequently plaqued.13 Nevertheless, all three cases of metastatic disease that occurred in this study had either persistent or TTT resistant melanoma. This suggests that persistent tumour after TTT poses a risk for metastatic disease, as has been the case in eyes that have failed irradiation.
This study also demonstrates that TTT is not an innocuous treatment. Thirty-two per cent of cases developed a complication, often with visual consequences. For example, 5% of eyes developed chronic cystoid macular oedema, which was refractory to measures such as topical medications, and subtenons or intravitreal triamcinolone. Other visually significant complications occurring in this series as well as those reported in the literature include retinal vascular occlusions, retinal traction from tumour bed contraction or epiretinal membrane formation, neovascularisation of the choroid or retina, visual field cuts, iris atrophy and synechiae, focal cataracts, vitritis, vitreous haemorrhage, macular holes, peripheral retinal holes and retinal detachments.4–8 The most concerning complication was intra- and extrascleral extension of tumour. Eight per cent of our patients had extension detected on ultrasound or histological examination of the enucleated eye. Consequently, even flat chorioretinal scars require ultrasonography to rule out intra- or extrascleral extension of the tumour. Zaldivar et al highlighted the necessity for continued clinical exam and diagnostic ultrasonography in a clinicopathological report of seven eyes with choroidal melanoma that failed TTT and were subsequently enucleated.14 In that series, while ultrasonography detected extrascleral extension in only one eye, ophthalmoscopy detected evidence of tumour expansion (which tended to grow laterally rather than in thickness) in five more eyes. These five eyes were subsequently found to have histological evidence of extrascleral extension. The results from Zaldivar, and from this current series, underscore the need for lifetime surveillance, with clinical exam, fundus photography, and ultrasonography.
Although the complication rate was high, visual acuity was generally maintained in these patients. The vision largely depended on the location of the tumour. As expected, tumours involving the fovea resulted in poor visual acuity, while extramacular tumours retained excellent vision (p<0.0001). Tumours with observed growth had better final visual acuity when compared with those treated for high-risk features (p = 0.013). The size of the tumour, relationship to the optic disc, patient age, patient gender and number of treatment sessions were not associated with vision loss. As mentioned above, laser-related complications also affected visual outcome. Final visual acuity was 20/40 or better in 50% of patients.
It is difficult to ascribe successful tumour control to cases of choroidal melanoma treated with laser without histopathological evidence of true melanoma. Some of these tumours may have been benign nevi or may not have been melanocytic lesions at all. The most accurate assessment of efficacy then relies on case selection and proper reporting. For example, most investigators will agree that an expanding lesion is likely a neoplasm rather than a nevus. While certain high-risk features are predictive of an expanding tumour, the presence of these features does not confirm future growth. In fact, even five high-risk features may only predict expansion in half of cases.15 16 Consequently, reports investigating treatments of choroidal melanoma must be read with a critical eye. Are the investigators treating growing melanocytic lesions, or are they treating tumours at high risk for becoming a growing lesion? In this series, like those reported in the past, not all patients had expanding lesions. While 54% of our patients had documented evidence of expansion, and 13% were ⩾3 mm in thickness, 21% were treated on the basis of high-risk features, and 12% were treated without a clear indication. Interestingly, the highest number of failures occurred in the patients with high-risk features followed by patients with a tumour size greater than 3 mm, followed by “no indication for treatment” and finally documented growth (45%, 29%, 25%, and 14% failure rate, respectively).
Treating all high-risk melanocytic tumours with TTT might save the lives of a few individuals, but the visual cost would be great. It has become clear to physicians using this mode of treatment that a minimally invasive laser procedure does not translate into a risk-free or even low-risk procedure. This fact must be made clear to the patient. It is the responsibility of the treating physician to discuss thoroughly all treatment options, as well as potential complications, treatment failure and the impact on vision, globe preservation and mortality. The treatment decision is then ultimately up to the patient.
Transpupillary thermotherapy may still have a role in the therapeutic arsenal for choroidal melanoma. Patients medically unstable for invasive surgery, those with advanced diabetic retinopathy, monocular patients with small tumours near critical visual areas, or small margin recurrences after irradiation may benefit from TTT. However, in this study, TTT as monotherapy was insufficient in 24% of patients. Consequently, all patients considering TTT as primary therapy must be selected carefully, counselled appropriately and followed indefinitely.
REFERENCES
Footnotes
Funding: This publication was in part supported by the core grant to the Department of Ophthalmology, Emory University School of Medicine from the National Eye Institute P30-EY06360.
Competing interests: None.
Ethics approval: Ethics approval was obtained.