Article Text

Abstract
Objectives: To evaluate pathological changes of retinal pigment epithelium (RPE) by polarisation-sensitive optical coherence tomography (PS-OCT).
Methods: Forty-four eyes (22 patients) with significant pathologies of the RPE were evaluated using PS-OCT. A transversal scanning time domain OCT system was used for two-dimensional cross-sectional imaging of retinal polarisation properties.
Results: The RPE scrambles the polarisation state of backscattered light (ie, acts as a depolarising layer), while the polarisation state of transmitted light is maintained. In patients with RPE pathologies irregularity, elevation, thickening or absence of the RPE is readily visualised by exploiting the depolarisation information. Polarisation scrambling in the sensory retina can be found in cases with advanced dry age-related macular degeneration. Sclera and fibrosis show characteristic birefringence in PS-OCT.
Conclusion: PS-OCT allows tissue identification based on polarisation scrambling and birefringence, providing additional information on RPE pathologies. It is a promising new tool for diagnosis, disease follow-up and evaluation of new treatment strategies.
Statistics from Altmetric.com
Over the last decade, optical coherence tomography (OCT) has emerged as a most valuable non-invasive imaging tool in ophthalmology.1–5
However, current OCT systems still have one drawback: they only measure the intensity of the light backscattered from tissue, which does not allow a direct differentiation of tissue types.6 Of special importance with respect to diagnostics would be a direct identification of the retinal pigment epithelium (RPE), allowing judgments on its integrity or any disturbances.
The polarisation state of backscattered light can provide the required information. Polarisation measurements in the retina are already widely used to measure the thickness of the birefringent retinal nerve fibre layer (RNFL) for glaucoma diagnostics.7 8 The current technology is the scanning laser polarimetry (SLP),9 which maps the transverse distribution of polarisation changes introduced by the retina, but does not provide depth resolution.
Polarisation-sensitive OCT (PS-OCT) provides the required depth-resolved information on the polarising properties of tissue.10 Several polarisation changing structures in the human ocular fundus can be identified:6 11 birefringent structures like the RNFL, Henle’s fibre layer, the sclera, and a polarisation scrambling layer (PSL). Based on clinical correlation, the PSL was identified as the RPE.6
It is the purpose of this paper to demonstrate the clinical relevance of directly imaging the RPE by PS-OCT.
PATIENTS AND METHODS
The study followed the tenets of the Helsinki agreement, and was approved by the ethics committee of the Medical University of Vienna.
Forty-four eyes (22 patients) were imaged using the PS-OCT system. All patients showed diseases affecting the RPE.
The principle of the PS-OCT system used is published elsewhere.11 12 The instrument is operated with a light source emitting at 841 nm and 4.5 μm depth resolution. Each frame (B-scan) consisted of 3400 (x)×500 (z) pixels (area of ∼3.4×1 mm2) and was recorded in 0.5 s. Three parameters are imaged by the PS-OCT system simultaneously (requiring only one measurement per sample location): intensity (as in conventional OCT), retardation and optic axis orientation (PS-OCT modes). Three tissue types can be differentiated with the additional polarisation sensitive information: polarisation-preserving tissue, birefringent tissue and polarisation-scrambling tissue.
Polarisation-preserving tissue can be recognised in PS-OCT images by constant retardation and axis orientation values with depth. Birefringence manifests itself by an increase in retardation values with depth, while the axis orientation is constant or varies on a scale considerably larger than the speckle size. Polarisation- scrambling tissue can be identified in PS-OCT images by completely random retardation and axis orientation values obtained from speckle to speckle.6 11 All polarisation-sensitive images presented here are displayed in a colour-coded map. Retardation values range from blue (0° retardation) to red (90° retardation), and axis orientation values range from blue (−90° axis orientation) to red (90° axis orientation). Values below a certain intensity threshold are displayed in grey.
RESULTS
RPE atrophy
Figure 1 shows an example for RPE atrophy imaged by the PS-OCT system. In the conventional, intensity-based OCT image (obtained with the PS-OCT system) structural changes such as RPE-band irregularity and thickening (mostly subfoveal) are observed. A bright linear structure that possibly corresponds to Bruch’s membrane is visible as soon as the overlying RPE is absent (red arrow in fig 1A). Increased depth penetration is expected to be observed in areas of absent RPE (cf, area left of yellow arrow in fig 1A), and the sensory retina is thinner where there is no underlying RPE.

Figure 1B,C (retardation and axis orientation) outlines clearly the polarisation-scrambling layer (PSL)—that is, the RPE (white arrow in fig 1B,C). In the present case, the PSL just reaches beyond the foveal depression (yellow arrow in fig 1), thus explaining a visual acuity of ∼20/32. Moreover, images obtained in PS-OCT mode clearly show that only part of the RPE band thickening seen in conventional OCT images refers to the RPE/PSL.
Birefringence is best observed in the retardation images because it causes an increase in retardation, while the axis orientation stays rather constant (depending on the orientation of the birefringent tissue). In areas where the overlying RPE is missing, the enhanced penetration into tissue enables the observation of an increase in retardation which is caused by the birefringent sclera (dotted arrow fig 1B) and could be used to estimate the choroidal thickness. The images in fig 2 are obtained from another eye with RPE atrophy. In the intensity image (cf, fig 2A), localisation of remnants of the RPE is rather difficult. The retardation image clearly confirms a few RPE islands (arrows in fig 2B) and an almost complete absence of the RPE/PSL-layer. Some of the remaining RPE islands appear to extend into the sensory retina (cf, inset in fig 2B). The lumen of vessels in the choroid as well as the underlying birefringent sclera can be detected.

RPE tear
RPE tears have characteristic features in conventional OCT imaging.13 As shown in fig 3C, an RPE band elevation with a flat and a steep slope are commonly seen. The RPE band is thickened and sometimes wavy. Next to the steep slope of the RPE elevation, the RPE band seems to be missing, and an increased depth penetration as described with RPE atrophy is observed. However, the association of the bright elevated structure (rectangle in fig 3C) with a histological structure is very difficult. The magnified retardation image (rectangle in fig 3D) reveals that this structure can be associated with the RPE. Because of the enhanced contrast in the PS-OCT images, the wavy and elevated RPE/PSL and the RPE tear can be easily visualised. Figure 4 refers to the same eye but images an area just next to the RPE tear. In fig 4A, a highly backscattering area above the RPE can be observed (marked with a rectangle). However, it is not clear if the RPE below this area is continuous. The retardation image (cf, fig 4B) shows that the RPE is continuous in this region and that the highly backscattering area scrambles the polarisation state.


Drusen
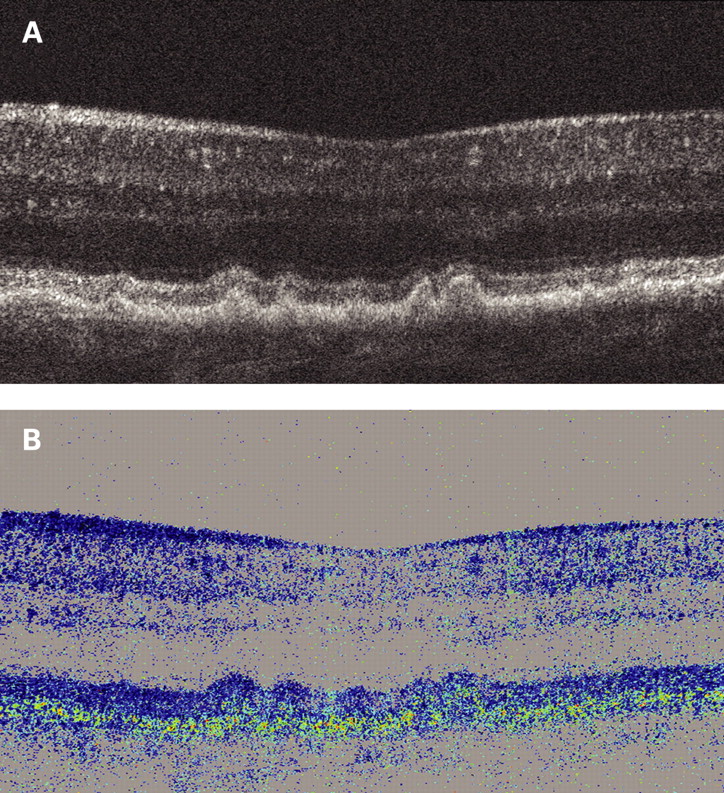
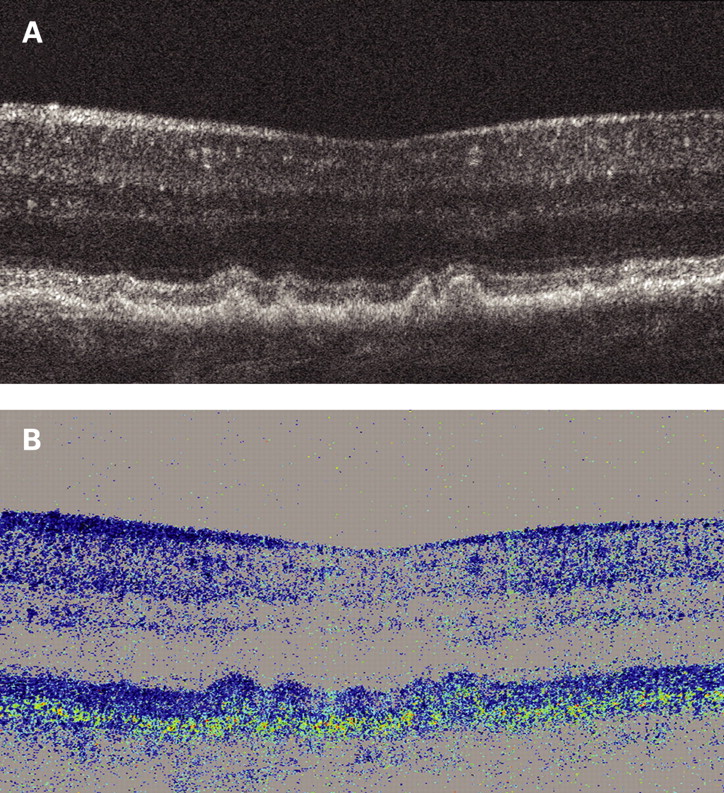
Soft drusen show in conventional and PS-OCT mode a focal elevation of the RPE/PSL, as shown in fig 5. In areas of drusen, the RPE band as seen by “conventional” OCT imaging appears elevated but continuous and regular. However, in the PS-OCT mode, the RPE/PSL is irregular with very small focal interruptions, indicating the RPE to be attenuated. Drusen themselves do not show characteristic features such as birefringence or polarisation scrambling in PS-OCT imaging.
In more advanced cases of drusen maculopathy such as fig 6, “conventional” OCT imaging still shows a wavy but continuous RPE band. In contrast, the PS-OCT mode indicates a very irregular and interrupted RPE/PSL (arrow in fig 6B). Rectangles in Fig 6A indicate focal spots in the sensory retina with increased signal intensity. PS-OCT reveals that the focal spots of area 3 probably correspond to blood vessels (no polarisation scrambling), whereas focal spots of areas 1 and 2 can be associated with fragments of the RPE.

Adult-onset foveomacular vitelliform pattern dystrophy
In contrast to the drusen described above, lesions of adult-onset foveomacular vitelliform dystrophy show no elevation of the RPE/PSL (cf, fig 7A). The RPE appears unaffected next to the pseudovitelliform lesion; however, centrally under the lesion an accumulation of tissue with increased reflectivity is observed, the nature of which is unclear from the intensity image. PS-OCT (cf, fig 7B) reveals that this tissue is polarisation-scrambled and therefore could potentially consist of RPE cells.

Fibrosis
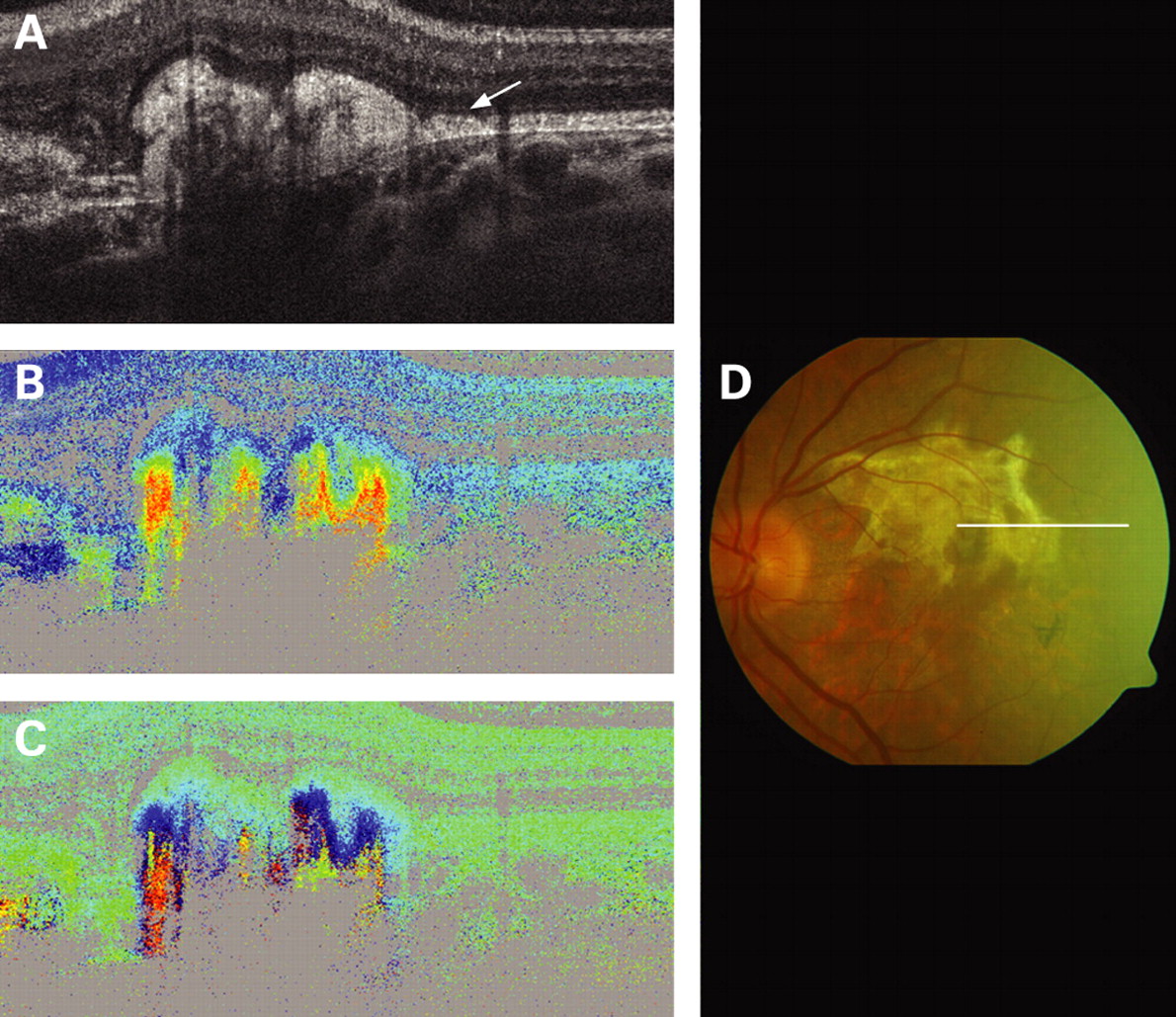
Figure 8A shows fibrosis as an endstage in neovascular AMD in conventional OCT with an unspecific thickening of the former RPE photoreceptor band. However, the intensity image does not allow tissue identification. The PS-OCT images (cf, fig 8B,C) reveal that the highly scattering area is birefringent (increasing retardation, axis orientation varies on a scale much larger than the speckle size; cf, birefringent sclera in fig 2) and that the RPE is missing. Note that steep colour changes in depth within the retardation image indicate highly birefringent areas. Form birefringence caused by a rather regular arrangement of collagen fibres within the fibrosis might be an explanation for the observed birefringence. Note that the amount of retardation/birefringence varies within the corresponding hyperreflective area; this might be explained by an inhomogeneous arrangement of the fibres.

Central serous chorioretinopathy
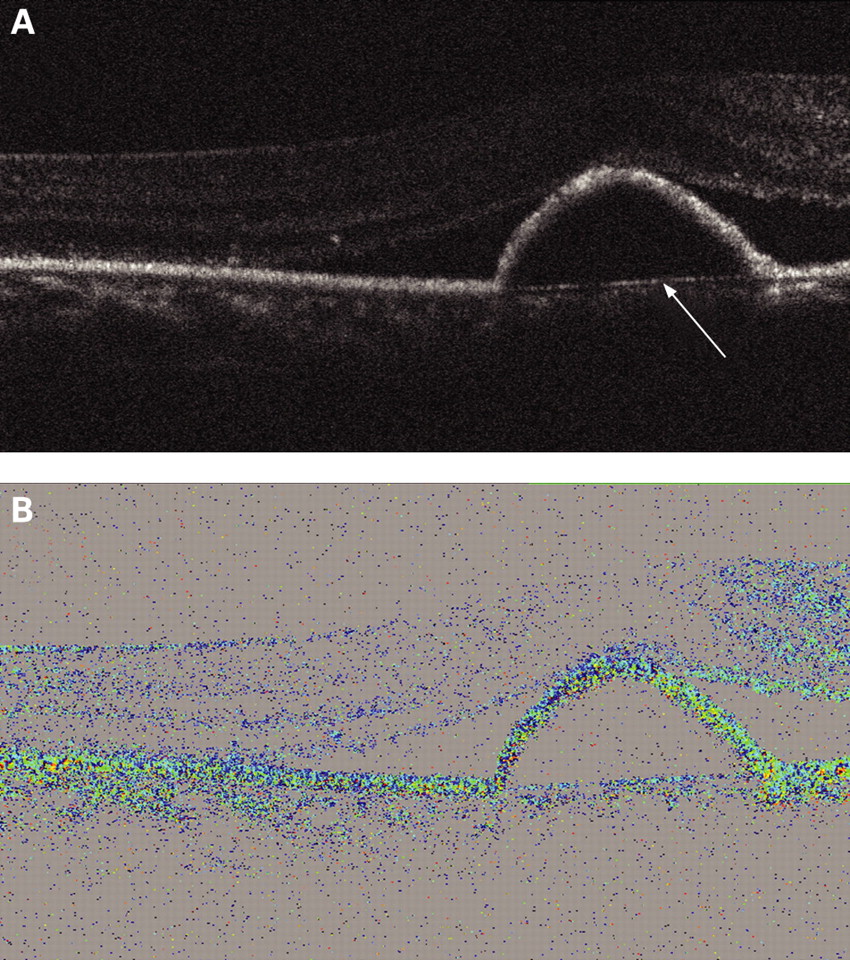
In central serous chorioretinopathy (CSC), a pigment epithelial detachment (PED) and subretinal fluid are commonly seen in close proximity. PS-OCT allows clear differentiation of PED and subretinal fluid. Figure 9 shows the B-scan of a patient with CSC. The PED is imaged by an elevation of the PSL. The fluid is located between PSL and the assumed Bruch membrane (bright layer marked with an arrow).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Conventional, intensity based OCT is frequently unable to directly differentiate between different types of tissue in the ocular fundus. PS-OCT is a functional extension of OCT which overcomes this limitation by measuring an additional physical property of light, its polarisation state.
PS-OCT exploits the fact that some ocular tissues change the light’s polarisation state in a very characteristic way.6 11 Birefringent tissues like the RNFL, Henle’s fibre layer, the sclera or fibrotic tissue increase the phase retardation of light with depth. Depolarising tissues like the RPE generate a random orientation of the polarisation state of backscattered light on a very small scale, whereby the polarisation state varies from speckle to speckle. This effect is also referred to as polarisation scrambling, and the RPE is identified as a polarisation scrambling layer (PSL). However, other so far not investigated tissues might show polarisation scrambling as well. Light that is transmitted through the RPE essentially maintains the polarisation state, as can be observed by the same blue colour (ie, the same degree of retardation) within the retardation images below as well as above the RPE layer (cf, figs 1, 5, 6, 9).
Several clinical aspects have further strengthened the conclusion that the observed PSL is the RPE. In areas of RPE atrophy, no PSL can be detected (figs 1 and 2) and in contrast to serous retinal detachments the PSL is elevated in PED (fig 9) and drusen (figs 5 and 6). Clearly identifying and differentiating the RPE using a non-invasive imaging technique is of great value. This allows the assessment of the extent and the degree of RPE damage in certain diseases, monitoring RPE disease progression and differentiating pathologies such as serous retinal detachments versus PED or drusenoid PEDs versus adult-onset foveomacular vitelliform dystrophy. Currently it is unclear which RPE properties lead to the polarisation scrambling phenomenon. Intracellular melanosomes or the RPE cell digitations embedding the photoreceptors could contribute to polarisation scrambling. Polarisation scrambling within the sensory retina, corresponding to pigmentary changes on funduscopy, could correlate with migrated RPE cells or pigment-loaded macrophages. Further investigation, especially in vitro models, is warranted. Polarisation scrambling in the retina might become a valuable prognostic factor. Inflammation, especially that driven by macrophages, is considered an essential part in the pathogenesis of AMD.14 Clinically visible hyperpigmentation, most likely correlating to the reported focal polarisation scrambling in the sensory retina, is a strong indicator for progression to neovascular AMD.15 16
The identification of the RPE by the characteristic polarisation scrambling might also be of great value in measuring retinal thickness. The inability to clearly identify the RPE in intensity-based OCT images makes it rather difficult to create a reliable algorithm for automated retinal thickness measurements. Current algorithms measure retinal thickness incorrectly in up to 92% of scans.17 Algorithms using PS-OCT images might provide more reliable retinal thickness measurements.
A further valuable finding in PS-OCT is the birefringence of fibrotic tissue and of the sclera. Fibrosis is a limiting factor for functional outcomes in several retinal and choroidal diseases. Identifying an unspecific thickening of the RPE-Band in intensity-based OCT as fibrosis by PS-OCT imaging is of significant value with regard to functional prognosis and potential treatment. New therapeutic strategies aim for reducing fibrosis,18 and PS-OCT might become a valuable tool not only by identifying fibrotic tissue but also by quantitative assessment.
A major advantage of the system is the simultaneous acquisition of polarisation-sensitive and conventional OCT images. Direct comparison of the different OCT modalities on exactly the same location provides the most valuable clinical insight.
PS-OCT is a promising new imaging technology for diagnosis, and prognosis as well as for evaluation of progression and treatment of different diseases affecting the RPE. Correlation with other established imaging modalities such as fluorescein angiography or autofluorescence imaging is warranted.19 20 Quantitative analysis of retardation and distribution of axis orientation is likely to give additional insight on the degree of RPE damage, for example. A high-speed spectral domain PS-OCT system is currently in development.21
REFERENCES
Footnotes
Competing interests: None.
Funding: Austrian Science Fund FWF-Grant P16776-N02.