Article Text

Abstract
Aims: The aim of the study was to evaluate functional and anatomical changes after intravitreal bevacizumab (Avastin®) in eyes with persistent macular oedema secondary to branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).
Methods: Twenty-nine consecutive eyes with macular oedema secondary to BRVO (21 eyes) or CRVO (eight eyes) were included in a prospective clinical trial. Eyes were treated with three initial intravitreal bevacizumab injections of 1 mg at a monthly interval. Retreatment was based on central retinal thickness (CRT) based on optical coherence tomography. If continuous injections were indicated up to month 6, the dose was increased to 2.5 mg.
Results: After 12 months of follow-up, mean visual acuity increased from 50 letters (20/100) at baseline to 66 letters (20/50+1; +16 letters; p<0.001) at month 12 and CRT decreased from 558 μm at baseline to 309 μm at month 12 (−249 μm; p<0.001). Patients received a mean of eight out of 13 possible injections. No drug-related systemic or ocular side effects following intravitreal bevacizumab treatment were observed. Fluorescein angiography revealed no progression of avascular areas.
Conclusions: Intravitreal therapy using bevacizumab appears to be a safe and effective treatment in patients with macular oedema secondary to retinal vein occlusion. However, the main limitations of this treatment modality are its short-term effectiveness and high recurrence rate.
Statistics from Altmetric.com
With a cumulative 10-year incidence of 1.6%, retinal vein occlusion (RVO) is the most common retinal vascular disease after diabetic retinopathy.1 Although the pathogenesis is still not fully understood, several risk factors have been associated with central retinal vein occlusion (CRVO) and branch retinal vein occlusion (BRVO), including age, hypertension, atherosclerotic retinal vessel changes, diabetes, hyperhomocysteinaemia and open-angle glaucoma.1–4 Both CRVO and BRVO seem to have a comparable risk profile, although recent publications hypothesise that the development of CRVO may be multifactorial and not be explicable by a simple thrombus formation alone.5
The most common sequela of RVO is the development of cystoid macular oedema (CMO) with a consecutive deterioration in vision. The major stimulus for the formation of macular oedema and neovascularisation in patients with RVO seems to be hypoxia-induced production of vascular endothelial growth factor (VEGF), an angiogenic factor that promotes angiogenesis and increases permeability.6
The only proven treatment method for eyes with CMO secondary to BRVO is macular grid laser photocoagulation. However, according to the Branch Vein Occlusion Study, only patients with macular oedema associated with BRVO and a visual acuity of 20/40 or less showed a significant visual benefit compared with the untreated control group.7 In patients with macular oedema secondary to CRVO, there was no difference between eyes treated with macular grid laser photocoagulation and observation only.8
Several studies have evaluated the efficacy of intravitreal triamcinolone in the treatment of macular oedema secondary to both BRVO and CRVO, but were only able to show stabilisation or a moderate improvement in visual acuity.9–11 However, the main limitation of intravitreal triamcinolone therapy is the high rate of side effects, such as cataract formation or increased intraocular pressure.
An alternative for patients with macular oedema secondary to RVO is anti-VEGF therapy. Since the first report of the efficacy of intravitreal bevacizumab (a recombinant monoclonal antibody binding to all isoforms of VEGF) in a patient with macular oedema secondary to CRVO in 2005,12 several retrospective case series have shown the benefit of this treatment, with an improvement in visual acuity and a decrease of central retinal thickness (CRT) in patients with macular oedema associated with both BRVO and CRVO.13–15 We have designed a prospective clinical trial to evaluate the effect of intravitreal bevacizumab therapy in patients with macular oedema in retinal vein occlusion (BRVO and CRVO). Consecutive patients with BRVO or CRVO were included and treated based on a standardised protocol over a period of 12 months with monthly follow-up visits. A previous report describes the 6-month results of this trial.16
PATIENTS AND METHODS
In a prospective clinical trial, 29 eyes of 28 patients with macular oedema due to RVO were included. Twenty-one eyes demonstrated BRVO and eight eyes presented with CRVO.
To allow for spontaneous recovery of macular oedema, especially in patients with macular oedema secondary to BRVO, only patients with macular oedema persisting longer than 3 months were included. Patients were required to have a baseline CRT of at least 250 μm and only patients without any neovascularisation were included. Macular grid laser was offered to patients with macular oedema secondary to BRVO with a visual acuity of 20/40 or less, and only patients who refused laser treatment or patients who had undergone laser treatment at least 3 months previously were included into the study.
All eyes underwent a complete ophthalmologic evaluation at baseline, day 1, day 7, month 1 and at monthly intervals during follow-up. Examinations included best corrected visual acuity (BCVA) testing using ETDRS charts at 2 m, slit-lamp and fundus examination including tonometry, standardised optical coherence tomography (OCT) imaging (Stratus, Carl Zeiss Meditec, Dublin, California, USA) and colour fundus photography. Fluorescein angiography was performed at baseline and at 3-month intervals to identify the presence of BRVO/CRVO, active extravasation and the extent of retinal non-perfusion.
All patients received three initial intravitreal Avastin® (bevacizumab) injections at a dose of 1 mg (0.04 ml) at monthly intervals.
After three initial injections, patients were examined monthly and retreated if OCT showed evidence of intraretinal or subretinal fluid. After treatment cessation, retreatment was indicated if recurrent fluid in any retinal compartment was associated with a vision loss of at least five ETDRS letters or if an increase in 1-mm CRT as measured by OCT fast macular mapping was at least 100 μm. If there was no resolution of macular oedema after 6 months of continuous monthly injections, patients received further injections at a higher dose of 2.5 mg (0.1 ml).
All intravitreal injections were performed in the operating room under sterile conditions. Bevacizumab was filled and packed under sterile conditions by the institutional pharmacy using tuberculin syringes containing a total volume of 0.2 ml (5 mg). Bevacizumab was injected intravitreally via the pars plana using a 30 gauge needle.
The t test was used for statistical analysis of changes in visual acuity and CRT. A p value of less than 0.05 was considered to be statistically significant.
RESULTS
Baseline characteristics and follow-up
A total of 29 eyes of 28 consecutive patients (15 women and 13 men) were included in the study. The mean age of the study population was 66 (range 43–81) years. Twenty-one eyes of 20 patients had CMO in association with BRVO, whereas eight patients had CMO secondary to CRVO. During follow-up, five patients were excluded from the study: one patient refused further treatment after three initial injections, one patient died of a salmonella foodborne intoxication after 6 months of follow-up, and three patients were unable to continue the relatively close follow-up visits for practical reasons unrelated to the disease. Baseline mean ETDRS visual acuity was 50 letters (20/100), ranging from three (20/800−2) to 78 letters (20/26−2), and baseline mean 1-mm CRT was 558 (range 353–928) μm, as measured by OCT.
Visual acuity and CRT outcomes
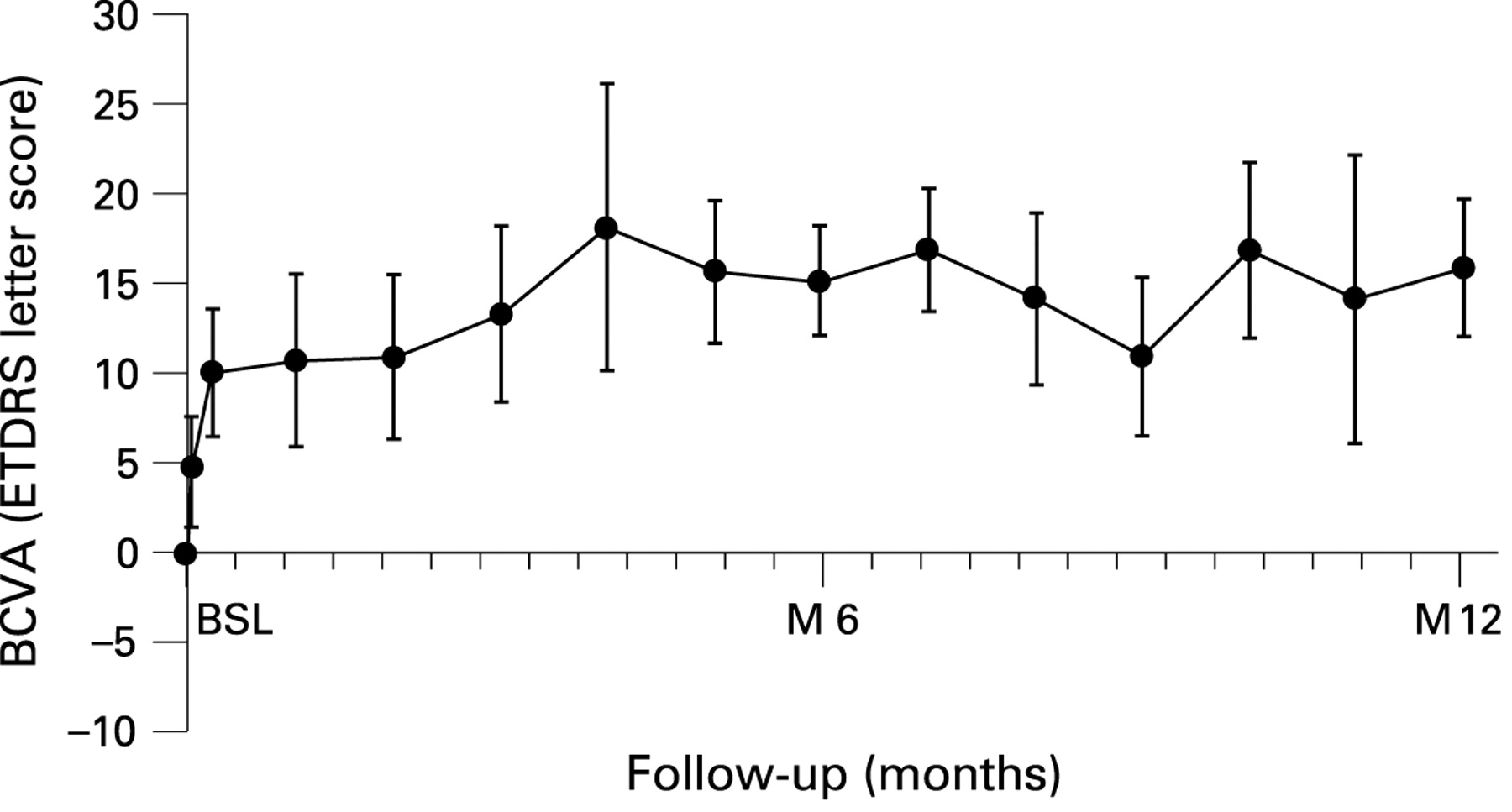
After 6 months of follow-up, mean BCVA had increased significantly to 65 letters (20/50; +15 letters; p<0.001), while mean CRT had decreased to 382 μm (−176 μm; p<0.001).16 Visual acuity decreased and CRT increased slightly but not significantly after 9 months to 61 letters (20/64; +11 letters; p<0.001) and 376 μm (−181 μm; p<0.001). After 1 year of follow-up, mean BCVA had increased to 66 letters (20/50+1; +16 letters; p<0.001) and retinal thickness had decreased to 309 μm (−249 μm; p<0.001). Figures 1 and 2 show mean changes in BCVA and CRT up to month 12. Figures 3 and 4 show examples of eyes with CRVO (fig. 3) and BRVO (fig 4) treated with intravitreal bevacizumab.

Change in best corrected visual acuity (BCVA). Values are means with standard errors. Data from baseline to month 6 have been published by Kriechbaum et al.16 BSL, baseline; M, month.

Mean change in central retinal thickness (CRT). Values are means with standard errors. Data from baseline to month 6 have been published by Kriechbaum et al.16 BSL, baseline; M, month.

A 53-year old patient with cystoid macular oedema secondary to central retinal vein occulusion. The patient received six injections at baseline, month 1, month 2, month 6, month 9 and month 11. CRT, central retinal thickness; Tx, treatments; VA, visual acuity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 66-year old patient with cystoid macular oedema secondary to branch retinal vein occulusion. The patient received four injections at baseline, month 1, month 2 and at month 3. CRT, central retinal thickness; Tx, treatments; VA, visual acuity.
Subgroup analysis
After 12 months of follow-up, mean BCVA in the CRVO group (n = 6) increased by seven letters (+1.5 lines), but the change was not statistically significant (p>0.05). In the BRVO group (n = 18), visual acuity increased from 55 letters (20/80) at baseline to 73 letters (20/32−2) at month 12 (+18 letters; p<0.001). CRT decreased significantly in both groups, by 268 μm (p = 0.007) in the CRVO group and by 241 μm (p<0.001) in the BRVO group after 12 months of follow-up.
Retreatment
Including the visit at month 12, eyes received a mean of eight out of 13 possible injections. Six eyes (20.7%) required continuous treatment up to month 12. Four eyes (13.8%) received only three initial treatments and no further retreatment. There was no difference concerning the retreament rate between the CRVO and the BRVO group and both groups received a mean of eight injections.
Safety
After 12 months of follow-up, no severe ocular (endophthalmitis, retinal detachment, traumatic cataract, uveitis) or systemic (thromboembolic event, systemic hypertension, kidney failure) adverse events were reported. No progression of avascular areas according to fluorescein angiography was observed. No patient developed neovascularisation of the optic disc, of the iris or elsewhere in the retina.
DISCUSSION
Results of this prospective clinical trial at 1 year showed that intravitreal bevacizumab treatment in patients with macular oedema secondary to RVO was associated with a significant improvement in visual acuity (+3.2 lines; p<0.001) and with a marked decrease in retinal thickness (−249 μm; p<0.001). During multiple treatments for as long as 12 months, no severe ocular adverse events, such as endophthalmitis, retinal detachment, traumatic cataract or uveitis, were detected. No patient showed evidence of severe drug-related systemic adverse events such as thromboembolic events, hypertensive crisis or kidney failure. However, one patient died at month 6 of follow-up due to salmonella foodborne intoxication, although this adverse event seems not to be related to intravitreal bevacizumab application. Even if the study was too small to provide solid data on safety, several studies showed comparable results regarding lack of severe adverse events.13–15 17
Consistent with a decrease in CRT as seen by OCT, fluorescein angiography revealed a reduction in the area of leakage. Avascular areas were stable or decreased, but did not progress during bevacizumab treatment.
Although nearly all patients showed an immediate response to intravitreal bevacizumab treatment with a reduction in retinal thickness and an increase in visual acuity as early as 1 day after treatment,16 macular oedema had not resolved completely in 86.2% of all patients after three initial injections. Furthermore, even with an OCT-guided treatment regimen the retreatment rate was high, with a mean of eight out of 13 possible injections over 1 year. In many patients we observed a recurrence of macular oedema after initial improvement and 20.7% of all patients showed no complete resorption of CMO despite continuous treatment up to month 12 and despite an increase of the dose to 2.5 mg bevacizumab. Obviously, primary non-responders do not show an enhanced reaction to more intensive treatment in RVO—a pattern that has already been demonstrated in patients treated with anti-angiogenic therapy of diabetic macular oedema.18 A recent paper suggests a potential rebound phenomenon due to an upregulation of VEGF receptors following intravitreal bevacizumab administration in patients with RVO of chronic nature.19 Recent studies also showed the close correlation between aqueous VEGF levels and the severity of macular oedema in patients with RVO.20 21 Therefore it may be hypothesised that a more prolonged VEGF blockade may be necessary in patients with high and prolonged VEGF levels.
Despite the clear limitation of the study due to the small number of patients in the CRVO group (n = 6), subgroup analysis indicated a better response to bevacizumab treatment in patients with macular oedema secondary to BRVO. Patients with CRVO showed a comparable reduction in CRT, but functional effects were not statistically significant. Therefore, our data do not provide evidence for recommending the use of intravitreal bevacizumab in patients with macular oedema secondary to CRVO.
It has been suggested that anti-VEGF therapy at an early stage of ischaemic CRVO may be more beneficial.22 However, we only included patients with no neovascularisation and a persistent (>3 months) macular oedema to allow for spontaneous improvement and to reduce a potential negative effect of anti-VEGF therapy on early collateral vessel formation.
Even if anti-VEGF treatment is only a symptomatic method for patients with CMO secondary to RVO, it showed promising results after 1 year of follow-up. The main drawback of this new treatment modality seems to be the short durability of the therapeutic effect with the need for frequent retreatments. Large randomised controlled clinical trials should be conducted to compare both entities and to evaluate the long-term efficacy and safety after repeated bevacizumab treatment in patients with CMO secondary to RVO according to their ischaemic status and intraocular VEGF levels.
Acknowledgments
The authors thank M Amschl, C Hirn and G Stock for performing fluorescein angiograms.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: Obtained.
Patient consent: Obtained.
Linked Articles
- At a glance