Article Text

Abstract
Background/aims: To evaluate in vivo three-dimensional (3-D) confocal laser scanning microscopy (CLSM) as a technique for visualising the corneal surface and epithelium.
Methods: Ten human corneas (three from healthy volunteers, three with bullous keratopathy, three from patients following penetrating keratoplasty, and one with corneal erosion) were examined by 3-D CLSM. A novel polymethyl methacrylate (PMMA) contact cap was designed to minimise artefacts due to applanation pressure.
Results: 3-D reconstruction and different visualisation techniques (volume rendering, cross-section, en face view, oblique section and surface reconstruction) were performed to demonstrate alterations to corneal surface and epithelium. Image quality (cell identification, motion blur, absence of compression artefacts, imaging of superficial structures and of subepithelial nerve plexus) was considerably superior to that obtained using a conventional contact cap with a planar surface.
Conclusions: 3-D CLSM permits in vivo visualisation and analysis of the corneal surface and of spatial arrangement at the cellular level in epithelium in normal and pathological corneas. The novel design of the contact cap minimises artefacts due to applanation pressure and improves the image quality of epithelial structures. The method provides a basis for further in vivo studies of alterations to corneal surface structure and its cellular arrangement.
Statistics from Altmetric.com
In recent years, knowledge about the ocular surface has been significantly enriched through the use of confocal microscopy.1–3 In vivo confocal laser scanning microscopy (CLSM) facilitates study of ocular surface structures in healthy subjects and in a range of clinical conditions. Three-dimensional (3-D) analysis of data permits evaluation not only of pathological findings but also of regenerative tissue processes at the cellular level.4 5
In principle, non-contact confocal microscopy can be used to examine corneal and conjunctival structures. An objective with a long focal length makes it possible to image the iris and lens surface.6 The main disadvantage of the non-contact method is the difficulty in obtaining precise data about fine tissue structures (eg, detailed information about the subepithelial nerve plexus or the layered structure of corneal epithelium). Contact confocal microscopy offers the advantages of superior image quality and precise pachymetry. After local anaesthesia, the examination is performed through a gel medium using a Z-ring contact element (ConfoScan 4, Nidek, Tokyo) or a polymethyl methacrylate (PMMA) contact cap (Rostock Cornea Module (RCM) in combination with a Heidelberg Retina Tomograph II (HRT II), Heidelberg Engineering, Heidelberg, Germany). The main disadvantages associated with contact investigation are applanation artefacts (eg, tissue folds, compression of the epithelium as well as of the cornea as a whole, and possible mechanical surface distortions).
In order to overcome these applanation artefacts we have designed a novel contact cap for use with the RCM-HRT II device. This innovative design minimises applanation pressure on the area investigated, thus reducing artefacts potentially interfering with the confocal images and improve the capability of correctly imaging of the most superficial cell layer. The aim of the present article is to demonstrate the potential of in vivo 3-D CLSM for ocular surface characterisation using an improved contact element..
MATERIALS AND METHODS
Device description
In vivo confocal microscopy was performed using an RCM-HRT II equipped with a water contact objective (Zeiss, Jena, Germany; 63×/0.95 W, 670 nm, ∞/0).6 The distance between the corneal surface and objective is kept stable using a single-use contact element (TomoCap, Heidelberg Engineering, Germany) with a planar surface and a refractive index of 1.49. We used a carbomer gel (Vidisic, Bausch & Lomb/Dr Mann Pharma, Berlin, Germany; n = 1.35) as a coupling medium.
The ability of a microscope to resolve fine specimen detail at a fixed object distance depends on the relationship between image resolution, angular aperture and the refractive index of the medium. The numerical aperture (NA) can be calculated from the equation NA = nsin α (where n is the refractive index of the contact medium, and angle α = half the angle of aperture). Accordingly, the limiting factor is the refractive index of the contact medium. Insertion of the PMMA contact element, which is coupled to the objective using a liquid immersion medium, produces an immersion sandwich structure in front of the cornea. The laser beam passes from the objective lens through the contact medium (n = 1.35) into the PMMA plate with a higher refractive index (n1 = 1.49) and then into the cornea with a lower refractive index (n2 = 1.44). According to the Snellius law, the focus is shifted towards the contact plate due to refraction, resulting in increased numerical aperture and resolution.6
To prevent applanation artefacts, the standard PMMA cap design was modified by fixing an additional 200 μm thick PMMA plate with a central hole (diameter 2000 μm) to the contact surface of the original TomoCap (fig 1A,B). Although compression of the surrounding corneal surface could not be completely eliminated, the cap construction enables confocal microscopy to be performed in contact mode with the tissue surface but without direct applanation pressure on the scanned area. It further avoids superimposition of interfaces (superficial cell layer and contact plate), resulting in a significant improvement in image quality.

Polymethyl methacrylate (PMMA) cap design and image quality. (A) Schematic drawing (not to scale) of the objective with a mounted PMMA cap, coupling medium and cornea. Inset top right: photograph of the modified cap design with a central hole in an attached PMMA plate. (B) Axial resolution (measured as half maximum of the through-focus response) was 7.6 μm with the conventional PMMA cap and 7.9 μm with the modified design. (C) Corneal epithelium in a healthy volunteer imaged with a conventional cap: upper wing cells with a very few washed-out superficial cells are visualised. Proper visualisation of the most superficial cells is altered by the direct contact of this cell layer with the PMMA cap. (A) Same cornea imaged with a modified cap: complete structure of superficial cells was recognisable. The bar represents 50 μm. RCM, Rostock Cornea Module.
In vivo confocal microscopy
Ten human corneas (three from healthy volunteers, age 19–32 years, one female and two males; three with bullous keratopathy, age 64–72 years, two females and one male; three following penetrating keratoplasty, age 67–78 years, two females and one male; and one with corneal erosion, age 30 years, male) were investigated. The study was performed once approval had been obtained from the Ethics Committee of the Medical Faculty, University of Rostock. The study was explained in detail to the patients, and informed verbal consent was given before any investigative procedures were conducted.
After topical application of anaesthetic (Proparakain-POS, Ursapharm, Saarbrücken, Germany), a drop of Vidisic was instilled into the inferior conjunctival fornix to serve as a coupling medium. Patients fixated on a bright object with their contralateral eye to stabilise their gaze. Image acquisition was performed in z-scan mode (manual sequence mode: 30 frames/s; total number of images: 100; automatic volume mode: 30 images) to a maximum depth of 60 μm. The acquisition time for the image stack was 1.2 s. A slit-lamp investigation was performed after confocal microscopy in order to verify the integrity of the cornea.
3-D reconstruction of the confocal images
Each 2-D image (400×400 μm, 384×384 pixels, 8 bit) represents an en face optical section of the cornea. 3-D reconstruction was performed on the basis of a minimum of 30 images using the AMIRA 3.1 software package (TGS Inc, San Diego). Before 3-D reconstruction, the image stacks were aligned using a semiautomatic least-square algorithm based on grey values. Different visualisation techniques (volume rendering, cross-section, en face view, oblique section as well as surface reconstruction) were applied to the scanned volume (400×400×40 μm) in each investigated case. With the acquisition parameters defined above, the voxel size was 1.04×1.04×0.95 μm. The total time required for the procedure ranged from 10 to 30 min, depending on operator skill and image quality.
RESULTS
Axial resolution in confocal microscopy can be measured by moving a surface through the focal plane and plotting the returning integrated signal. To replicate this, we moved the focal plane through a fixed surface (glass plate) and presented the results as full-width at half maximum of the through-focus response (fig 1B). These data show the axial resolution of the RCM-HRT II to be 7.6 μm with the original cap and 7.9 μm with the redesigned contact element.
The new contact cap design enables the corneal surface to be studied without direct contact pressure on the scanned area, thus minimising artefacts due to corneal compression. The most superficial cell layer from the same cornea was imaged with a conventional cap design (fig 1C) and with the novel PMMA cap design (fig 1D).
In volume scan mode, the existing set-up allows up to 40 frames to be obtained with a step progression of about 2 μm. The healthy cornea is presented in figs 2, 3. All histological structures of the corneal epithelium are shown: superficial, intermediate and basal cells as well as the subepithelial nerve plexus and Bowman membrane. With the aid of 3-D reconstruction, it is possible to perform in vivo volume rendering (fig 2A), cross-sectional (fig 2B) and en face views (fig 2C), oblique cuts of the rendered stack (fig 2D) as well as surface reconstruction (fig 3).

Representative images of a 3-D reconstruction of the cornea. (A) Volume rendering: 3-D stack of images (two series of 100 2-D en face images, distance between two adjacent images 2.5 μm, frame rate 30 frames/s, mechanical z-scan, sequence mode). (B) Cross-section through previous image: all histological structures of the cornea are present. (C) En face view of rendered volume at the user-defined depth; the quality of the single confocal image is not disturbed. (D) Oblique section through epithelium and anterior stroma: the angle of the section can be changed in order to see structures located at a greater or lesser depth (automatic z-scan, volume mode).

In vivo 3-D reconstruction of the ocular surface in healthy human volunteers. (A, B) In vivo confocal images of the superficial cells of corneal epithelium, depth 1 μm (A), and of superficial and upper wing cells, depth 5 μm (B). (C) 3-D reconstruction of the superficial cell surface: the roughness of the ocular surface derived from intrinsic irregularities of the surface epithelial plane. The bar represents 50 μm.
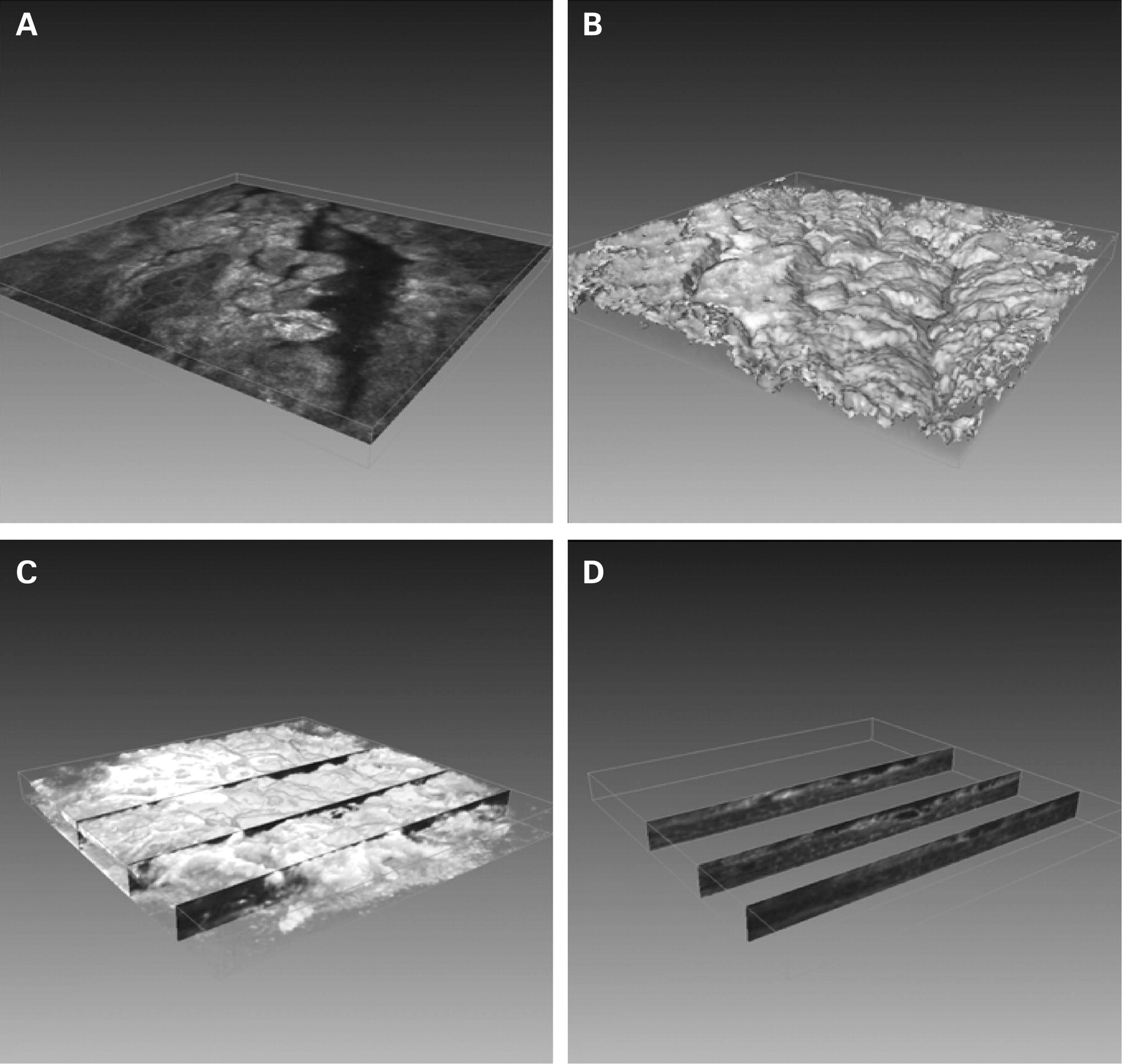
In the case of bullous keratopathy, all layers of the epithelium are oedematous, and the cellular epithelial defect is visible as far as the level of the basal cells and Bowman’s membrane (figs 4A–C). Cross-sections (fig 4D) show the depth of the epithelial changes, permitting user-defined oblique sections and analysis of each area of tissue. Reconstruction of the corneal surface reveals the defect zone and enables results to be compared at the microscopic level (fig 4B).

In vivo 3-D reconstruction of ocular surface in bullous keratopathy (A–D). (A) In vivo confocal images of superficial and wing and basal cells: oedema of all three layers of epithelium, and a cellular epithelial defect is visualised as far as the level of the Bowman membrane. (B–D) In vivo 3-D reconstruction: (B) irregularity of ocular surface with deep defect; (C) user-defined cross-sections through bullous cornea; (D) isolated sections: each cross-section contains the whole stack of epithelial images reflecting the clinical situation.
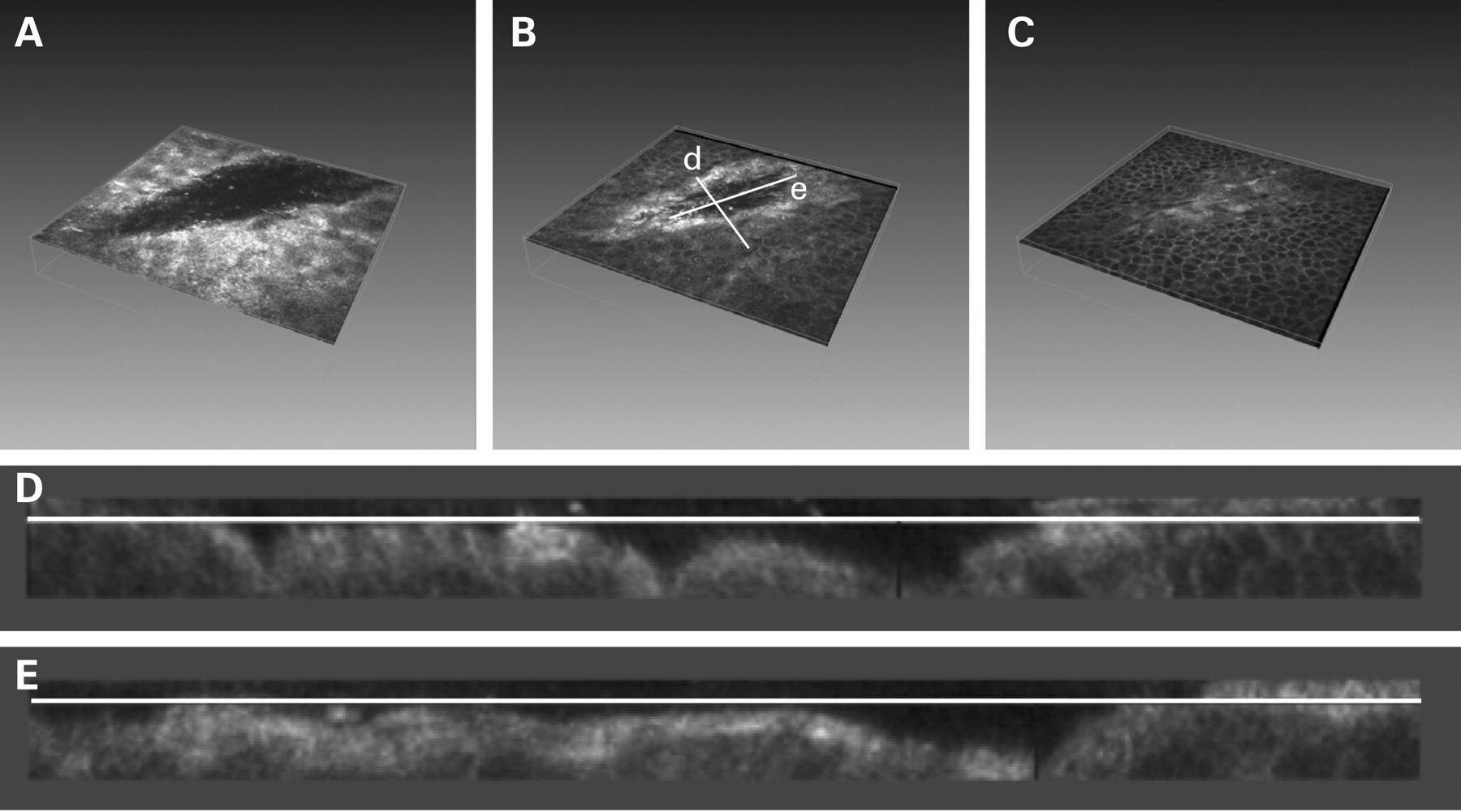
In addition to their qualitative presentation, defects can also be measured quantitatively. Figure 5 illustrates the reconstruction of a corneal erosion as far as the level of the basal cells. The geometry of the defect is presented (fig 5B,D,E) with its longitudinal and transverse measurements, thus providing complete information on 3-D coordinates.

In vivo 3-D reconstruction of ocular surface in corneal erosion (A–C). In vivo confocal images of corneal erosion at the level of the superficial (A), upper (B) and lower wing cells (C): transverse and longitudinal axes (corresponding to D and E) are shown. (D, E) Reconstructed images of the transverse (D) and longitudinal (E) axes of the corneal erosion.
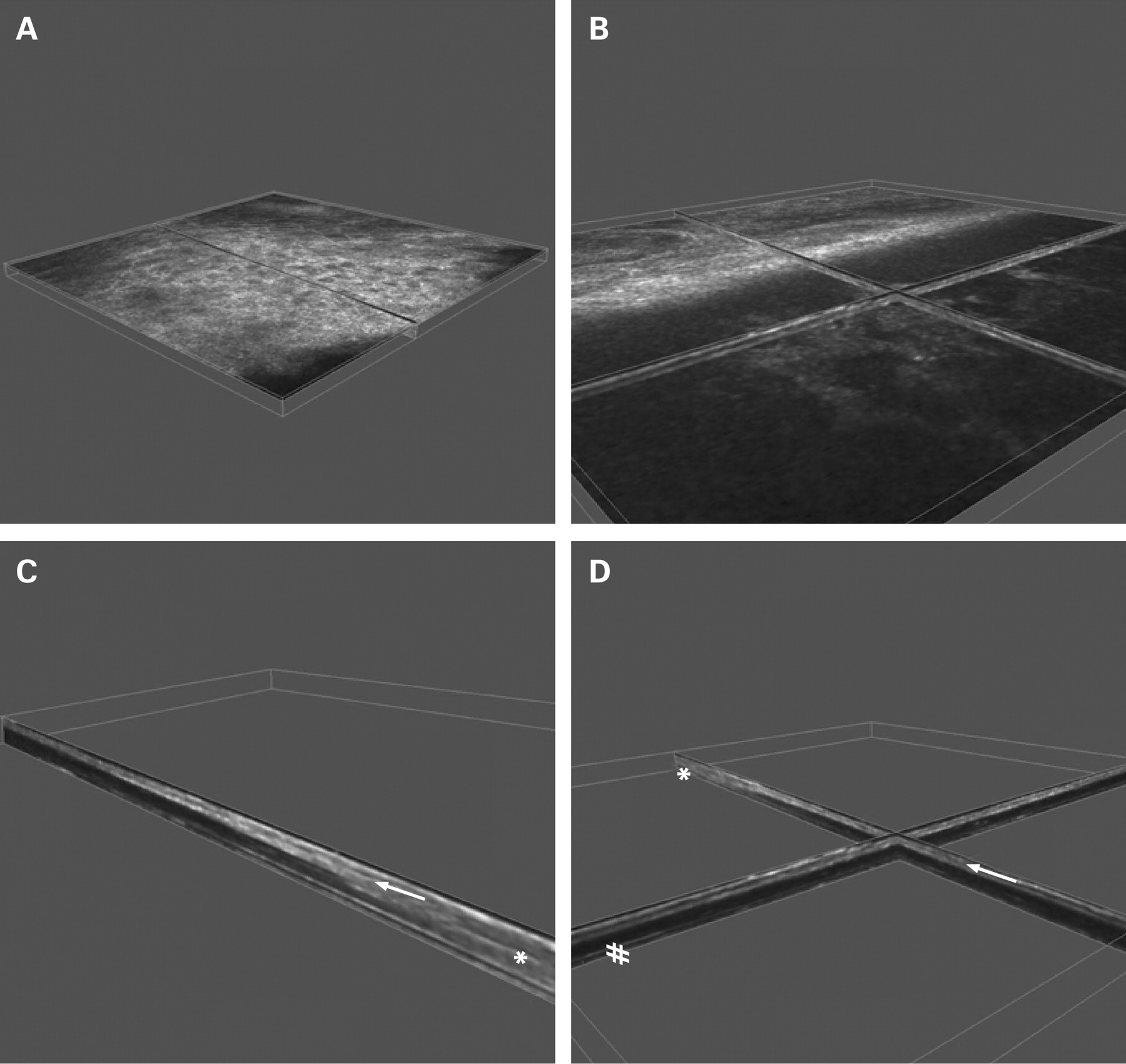
Confocal microscopy also enables structures with opacities to be visualised. Figure 6 shows the situation after penetrating keratoplasty, with the donor–recipient crossover zone clearly visible. Even in cases of epithelial opacity, information can be gained about the stroma (oedema, thickness of epithelium and stroma, scarring, opacities, etc). Figure 6C,D shows the hyper-reflective epithelium as well as the hyporeflective stroma without signs of graft rejection (oedema, inflammatory cell infiltration, etc).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In vivo 3-D reconstruction of ocular surface after penetrating keratoplasty at the donor–recipient crossover zone. (A, B) In vivo confocal images: (A) complete graft epithelialisation—superficial cells (imaged) and the epithelium as a whole are hyper-reflective; (B) crossover zone with hyporeflective stroma of graft at a depth of 80 μm. (C, D) In vivo 3-D reconstruction: cross-sections through crossover zone and graft: opaque recipient cornea (*), clear graft (#) with complete epithelialisation (arrow).
DISCUSSION
The aim of the present article is to demonstrate the potential of in vivo 3-D CLSM for ocular surface characterisation with the aid of commercially available software. Modern software packages enable images to be edited, with excellent quality as standard. With the modern devices in current use, the main problem of contact confocal microscopy investigations is compression of the superficial cell layers with attendant loss of quality.5 7 8 Conversely, non-contact confocal microscopy is associated with increased corneal movement due to the patient’s breathing or pulse; this makes exact pachymetry as well as imaging of fine, miniscule structures virtually impossible.
The RCM-HRT II with its axial resolution of 7–8 μm is a reliable confocal laser scanning microscope for in vivo investigation and 3-D reconstruction of the ocular surface. Compared with the axial resolution of other microscopes (tandem scanning confocal microscope (TSCM): 9 μm;7 ConfoScan: 29 μm9), the RCM offers an excellent opportunity to render the ocular surface in authentic 3-D proportions.2 5
Recent studies of corneal image quality comparing white light scanning slit and laser scanning systems3 10 have shown that the laser system is more efficient for imaging epithelial structures and the subepithelial nerve plexus (SEP) but is less satisfactory in terms of the number of compression artefacts. Improved cell recognition in the superficial layer structures and absence of mechanical artefacts (folds) are the conspicuous advantages offered by CLSM with a modified PMMA cap.
Differentiation of fine structures in the cornea requires the smallest possible distance between images in the z-axis, in conjunction with high axial and lateral resolution. Recently published papers on the subject of 3-D reconstruction have described studies with TSCM as well as CLSM. In 2000, Li et al presented an on-line 3-D imaging system developed in-house and based on TSCM.7 The software allowed acquisition of 2-D images (30 frames/s) that were processed into real-time 3-D images with a 2.12 μm interval between adjacent images in the z-axis. Axial resolution of 9 μm as well as contact investigations through gel as a coupling medium were insufficient for epithelial structure analysis and especially for ocular surface reconstruction due to increased motion blur. The proposed data-averaging approach did not completely compensate for data loss. Some years later, the Rostock group6 11 suggested processing RCM data with external software. The features of the RCM-HRT II enabled the subepithelial nerve plexus as well the whole cornea to be reconstructed. Taking advantage of the high resolution offered by CLSM and the homogenous illumination of the image, Patel and McGhee produced a reconstruction map of the subepithelial plexus in the normal human cornea and in keratoconus.12 13 The novel PMMA cap design minimises artefacts (false folds of Bowman and Descemet membrane layer as well as stromal striae) and permits quality in vivo CLSM.
The RCM-HRT II software enables 2-D image stacks to be acquired in volume scan mode (frame rate up to 30 frames/s) with simultaneous control of image sequence quality. Nevertheless, some 50% of all data are not suitable for further reconstruction due to motion artefacts. Another disadvantage of this technique is the depth of the image stack (max. 60 μm). This is sufficient for epithelial reconstruction as well for 3-D visualisation of the subepithelial plexus but not for reconstruction of the whole cornea. Alternatively, the mechanical z-scan6 can also be used for the 3-D reconstruction of the complete cornea with an increased z-axis interval and consequent image misalignment (fig 2). All these problems illustrate the difficulties inherent in the on-line conversion of high-resolution images and point to the need for well-established image-processing software.
As intimated above, one of the solutions proposed to compensate for motion blur of the image is to average the data.7 In our system, used in contact mode with the new PMMA contact cap, we are able to visualise single layers of superficial cells at different depths without/with minimal artefacts, allowing structural reconstruction without loss of resolution.
This modification would be of particular interest in ocular surface studies, for example in dry eye and in research into the effects of preservatives, or in wound-healing mechanisms and defect geometry in dynamic refractive surgery, keratoplasty, amniotic membrane grafting and corneal cross-linking. Moreover, the potential for studying the whole epithelium enables corneal thickness to be analysed without possible compression effects. Complete elimination of the surrounding corneal surface compression is not possible, even with the modified cap. Nevertheless, the applanation artefacts could be minimised: according to our unpublished data, mechanical compression of the epithelium accounts for about 10% of epithelial thickness with traditional techniques, and this fact should be taken into account in the research setting.
In summary, the proposed novel design of the contact cap yields significantly improved confocal image quality and allows 3-D reconstruction of the corneal surface and epithelium once the user-friendly external software has been mastered. Our technique permits reconstruction of the corneal surface in vivo in contact mode while avoiding commonly encountered compression artefacts. The processing of 2-D into 3-D data provides a basis for further in vivo studies of alterations to corneal surface structure and its cellular arrangement.
Acknowledgments
The authors are grateful to C Feinbaum, for his helpful comments and critical review of the manuscript, and to D Beattie for editorial support.
REFERENCES
Footnotes
Competing interests: AZ, JS and RFG are consultants to Heidelberg Engineering, Heidelberg, Germany.
Funding: The study was supported in part by the DFG (Transregio 37, Micro- und Nanosystems in Medicine—Reconstruction of Biological Functions) and by an internal grant from the University of Rostock (FORUN N 889009). The PMMA caps were manufactured in collaboration with Acri.Tec AG (Berlin, Germany).
Ethics approval: Ethics approval was provided by the Ethics Committee of the Medical Faculty, University of Rostock.
Patient consent: Obtained.