Article Text

Abstract
Background/Aims To develop and assess a zonal classification of the retina to facilitate description of the location of retinal haemorrhages in children.
Methods A novel zonal classification of the retina was devised based on the anatomical landmarks of the optic disc and vascular arcades, by reviewing a large number of wide field digital retinal images drawn from our database of children with accidental and non-accidental head injury and other encepthalopathies. Four expert examiners then independently ‘located’ 142 retinal haemorrhages by zone, from 31 high quality photographs.
Results Cohen's unweighted κ scores for all possible pairs of the four raters (ie, six pairs) ranged from 0.86 to 0.92, that is ‘almost perfect’ agreement. Fleiss' κ for agreement between multiple raters (four) and for multiple categories (three) was 0.8841, that is ‘almost perfect’ agreement. Cohen's unweighted κ statistic for intrarater reliability gave an overall concordance that ranged from ‘substantial’ to ‘perfect’ agreement.
Conclusion This new retinal zone classification and the use of photographs and templates is a very reliable tool for reporting the location of retinal haemorrhages from multiple aetiologies in children, and may be useful for research and medico-legal reports.
- accidental traumatic brain injury
- child health (paediatrics)
- imaging
- medico-legal reports
- non-accidental (inflicted) traumatic brain injury
- retinal haemorrhages
- retinal zones
- trauma
Statistics from Altmetric.com
- accidental traumatic brain injury
- child health (paediatrics)
- imaging
- medico-legal reports
- non-accidental (inflicted) traumatic brain injury
- retinal haemorrhages
- retinal zones
- trauma
Precise description of the number, location and morphology of retinal haemorrhages in children with suspected non-accidental head injury is of great importance for diagnostic, legal and research purposes.1 As part of a prospective, longitudinal study of retinal haemorrhages caused by accidental and non-accidental head injury and other encepthalopathies in children, we have developed a zonal classification of the retina to facilitate description of the location of retinal haemorrhages in these cases.
Existing zone classifications have been used by a number of authors in research publications investigating the location and demography of retinal lesions such as retinopathy of prematurity,2 cytomegalovirus choroiditis,3 retinal haemorrhages in the newborn4–12 and shaken baby syndrome.13–15 These classifications have variously been used to describe the retinal location, retinal layer involved and extent (size and number) of lesions, and are summarised in table 1.
Literature reports of retinal haemorrhage classification systems utilised for individual studies, based on combinations of extent (size and number) of retinal haemorrhages, retinal layer involved and location (distribution)
Some of the reported classifications lack precise definition, some are too cumbersome for routine use and few have been validated with replication studies. A number commonly rely on ‘size’ in relation to optic disc diameter and generally refer to retinal locations such as macula, peripapillary and peripheral area. The wide variety of these suggest that none have found universal acceptability and we have thought to combine the ‘best’ features of those described by Wilkinson et al14 into an adapted description of retinal zones. From our experience with a large database of cases of traumatic and non-traumatic encephalopathies we have found that the only landmarks that could be consistently identified were the optic disc and the arcades of the temporal vessels. In many eyes the position of the fovea could not be reliably determined, because of the presence of haemorrhages or traumatic retinoschisis. Similarly, the position of the vortex veins ampullae could not be identified in many eyes because of the presence of haemorrhages and insufficient quality of peripheral imaging.
Our aim was therefore first to devise a classification that would precisely and comprehensively describe the entire retina, but also prioritise the key locations of interest in the differential diagnosis of suspected non-accidental head injury cases—the peripapillary area, the macula and the retinal periphery, and second to test the inter and intrarater reliability of this new zonal classification with RetCam images that could be of value for clinicians, researchers and in medico-legal reporting.
Materials and methods
Our classification was devised by reviewing a large number of wide field digital retinal images obtained using a ‘RetCam’ (Clarity Medical Systems, Irvine, California, USA) camera with a 120 degree lens. The images were drawn from our database of children with accidental head injury, suspected non-accidental head injury and other encepthalopathies. The Lothian Regional Ethics Committee approved the use of anonymised images for these studies.
The following zone classification was therefore devised.
Definitions (see figure 1A)
Zone D—the peripapillary circle
We use a circle (zone D), which has a diameter of three times that of the optic disc and is centred on the centre of the optic disc: that is zone D covers the optic disc and one disc diameter all around the disc. This gives us a view that includes the nasal side of the optic disc.
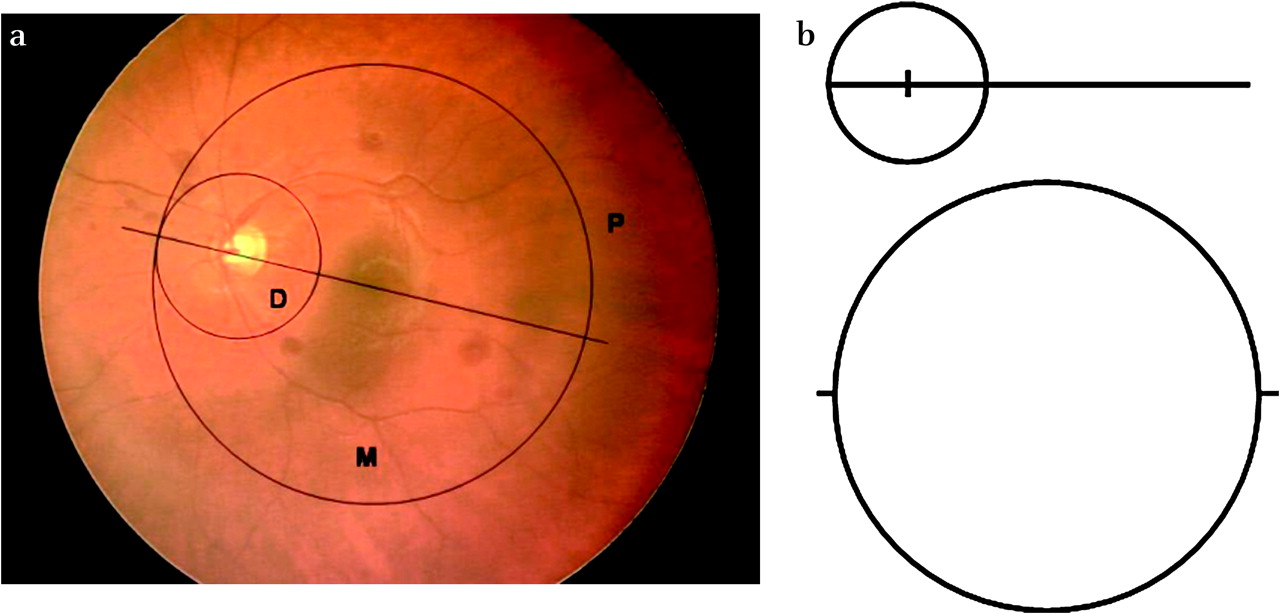
{kind=link}
(A) Fundal image with the retinal zones superimposed. Zone D: Circle with diameter of three times optic disc diameter, centred on the centre of the optic disc. Zone M: Circle with a radius of four times diameter of optic disc (ie, diameter of 8× optic disc width). Centre of zone M circle is on a line bisecting the retinal arcade and optic disc and joining the tangential point of contact between zone D and zone M. Zone P is the peripheral area, outside zone M. (B) Scaled transparent acetate templates to overlay on fundal image, with marks at centre of small circle and at diameter of large circle, for ease of alignment.
Zone M—the posterior pole
This is an area contained within a circle with a radius of four times the optic disc diameter (ie, zone M diameter is eight times that of the optic disc). The centre of this circle is on a line bisecting the retinal arcades and the optic disc, and at a point on this line, so that the nasal edge of the zone M circle is tangential to circle D, (ie, circle centred approximately on the fovea).
Zone P—periphery
The remainder of the image is considered to be zone P (ie, the peripheral zone), which is outwith zone M.
Preparation of digital retinal image for zoning
Counting and locating the haemorrhages was done using high quality hard copy photographs. For each retina studied, we choose the photograph ‘most centred’ in the picture so as to have the maximum view of all three zones as defined above.
The zones, and therefore circle diameters, were based on the actual horizontal width measurement of the optic disc (either measured and ‘zoned’ by electronic measurement on screen, or on the printed photograph). This eliminated error due to anatomical variation in the true optic disc diameter, as well as minor disparity in image magnification due to variation in ocular optics and imaging artefact, or inter-computer differences.
Two clear transparent (acetate) templates were used to analyse each image, as seen in figure 1B. In practice, sets of templates were prepared to cover the range of optic disc diameters encountered. First the template was positioned over the image, with the small circle centred over the optic disc so that the line bisected the vascular arcade, and second the large circle was aligned with its axis in line with the bisecting line and positioned to contact the most nasal point of the small circle. Positioning of the templates on the photograph took only a few seconds to align accurately.
Ascribing a zone to each haemorrhage
Haemorrhages were counted and the number per zone was recorded. When a haemorrhage was found to overlap more than one zone, it was counted only once, and designated to be in the innermost zone. For example, a haemorrhage lying partly in zone D and partly in zone M is counted as a zone D haemorrhage; if in zones P and M, it is counted for zone M; and if it overlaps all three zones, then it is counted as zone D.
Interrater study
The examiners consisted of two experienced paediatric ophthalmologists (raters 1 and 3), a paediatric ophthalmology fellow (rater 4) and a paediatric neurologist with experience in non-accidental head injury (rater 2).
The four examiners were independently shown 142 nominated haemorrhages on 31 high quality RetCam photographs. The images included: right and left eyes, images of the same eyes on different days after admission (day 1 equals day of admission); images from children with different retinal haemorrhage aetiologies (accidental traumatic head injury, non-accidental (inflicted) traumatic brain injury and other encephalopathies); retinal haemorrhages in different retinal layers and appearance; and from all regions of the retina. The examiners were masked to patient details including the likely aetiologies, but each image was identified by right or left eye. The order of presentation of images was a random sequence, but the same order was used for each rater. Specified nominated haemorrhages from each image (generally five per fundal image) were ascribed a zone by each rater. Six retinal images were re-presented within the random presentation sequence, to test intraobserver consistency.
Statistics
Interrater agreement was measured for all pair combinations of raters (Cohen's unweighted κ) as well as for multiple raters (Fleiss' unweighted κ).
Intrarater agreement was also measured using Cohen's unweighted κ.
These measures calculate the degree of agreement in classification over that which would be expected by chance, and are scored as a number between 0 and 1, and the generally accepted guidelines are that zero represents no agreement, 0.0–0.2 slight agreement, 0.21–0.4 fair agreement, 0.41–0.6 moderate agreement, 0.61–0.8 substantial agreement and 0.81–1.0 almost perfect agreement, respectively.16
Results
Cohen's unweighted κ scores for all possible pairs of the four raters (ie, six pairs) ranged from 0.86 to 0.92, that is ‘almost perfect’ agreement (table 2), and the percentage disagreement on location, of all 142 haemorrhages, between the rater pairs varied from 5.63% to 8.45%. Fleiss' κ for agreement between multiple raters (4) and for multiple categories (3) was 0.8841, that is ‘almost perfect’ agreement.
Interrater κ scores for pairs of raters
Cohen's unweighted κ statistic for intrarater reliability is shown in table 3 in which the overall concordance ranged from ‘substantial’ agreement to ‘perfect’ agreement. It can be seen that although raters 1 and 2 had similar agreements (24/26) on the repeat test, the different unweighted κ values reflect a different distribution of two of the haemorrhage locations between these raters. The differences occurred when haemorrhages just overlapped one of the zone circles. There was a different zonal allocation for two retinal haemorrhages by these raters, although intrarater consistency was maintained.
Intrarater unweighted κ scores for the four raters
Discussion
We have proposed a simple schema for reporting of the location of retinal haemorrhages, using fundal photographs, and employing a graticule that describes circles and areas based on measurements relative to the diameter of the optic disc and a line bifurcating the temporal retinal arcade. Although we used a ‘RetCam’ photographic system with a 120 degree lens, the system could be used with any photographic system as the measurements used are relative to the optic disc diameter and are not absolute. Images taken with RetCam narrow field, high magnification lenses could also be analysed in this way. Zone D corresponds to the peripapillary area (disc), zone M to the posterior pole (including macula) and zone P to the peripheral retina, including the ora serrata.
Interrater agreement shows the ‘almost perfect’ agreement between different raters from different clinical specialties (interrater agreement 0.86–0.92 for pairs and 0.8841 for multiple interraters Fleiss' κ). Intrarater agreement for consistency in zone allocation by each rater was similarly ranged from ‘substantial’ to ‘perfect’. Near-perfect results are uncommon for agreement on clinical signs between clinicians.17 The high κ values obtained with our zones on retinal photographs from RetCam imaging may be higher than those that would be obtained by simply describing a zone after using direct or indirect ophthalmoscopy alone.
We have experienced few limitations using this new graticule system. One reason for slight disagreement on zone allocation was that occasionally haemorrhages with particularly blurred or diffuse edges closely approximated the boundary of a zone. Although there was almost perfect agreement in zone allocation by the raters, when differences did occur it was always because of a haemorrhage just overlapping one of the zone circles, and this was the reason for the different κ values in table 2 between rater 1 and rater 2.
A potential limitation is the determination of the centre of the optic disc and the ‘arcade bisecting line’, for subsequent positioning of the zone circles. Centering the optic disc is based on the rater's impression and is not an absolute measurement, but given the relatively small area of the optic disc with respect to the fundus, this is unlikely to contribute to any appreciable lack of agreement. Placement of the ‘arcade bisecting line’, however, is more subjective (angles are not measured and the arcade vessels are not precisely symmetrical) and the slope of the line subsequently determines the position of zone M outer limit and hence zone P. Such minor irregularities may also have contributed to not obtaining perfect κ agreement.
There are a number of advantages that have become evident when using our graticule and zone definitions: (1) The system is simple, and repeatable, and equally reliable and usable by personnel other than consultant ophthalmologists. (2) This schema is suitable for locating retinal haemorrhages from all causes in children (accidental and non-accidental traumatic brain injury and other non-traumatic encephalopathies). (3) Repeated examinations allow researchers to identify the same haemorrhage on successive occasions and possibly to their resolution. (4) Landmarks for the zones are obvious, that is optic disc and temporal retinal arcade (even when there are multiple haemorrhages, retinoschisis, dark pigmented fundi, etc). (5) Although designed essentially as a research tool, our zonal grid, because of the circle areas D, M and P (which identify peripapillary, posterior pole and importantly in inflicted traumatic brain injury, the periphery/ora serrata), makes it particularly suitable for enumerating and locating retinal haemorrhages for medico-legal purposes. (6) Cases of non-accidental head injury often have retinal haemorrhages ‘too numerous to count’ and although counting will not be easier, approximate numbers can be reported as ‘frequent’ in all these retinal zones.
Descriptions of retinal haemorrhages in suspected child abuse cases that are made using an ophthalmoscope will inevitably be qualitative, unless the number of haemorrhages present is very small and their locations are in relatively easily defined parts of the retina. We believe that any meaningful descriptive system is dependent on photographs. Our approach can be used for any photography system, as all measurements are made relative to the dimensions of anatomical features and are not absolute.
This new retinal zonal classification and the use of the templates is a very reliable tool for reporting the location of retinal haemorrhages from multiple aetiologies in children, including accidental and non-accidental trauma. The statistical agreement between raters indicates a level of accuracy and robustness suitable for research purposes and medico-legal reporting for courts.
Acknowledgments
The authors are grateful for the fruitful discussions they had with Dr Alex Levin (Philadelphia), and to Ms Catriona Graham, lead statistician, Wellcome Trust, Clinical Research Facility, Western General Hospital Edinburgh.
References
Footnotes
Funding This study was supported by the RS MacDonald Charitable Trust and the Royal College of Surgeons Edinburgh (Ophthalmology Grant-Royal Blind).
Competing interests None.
Ethics approval This study was conducted with the approval of the Lothian Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.