Article Text

Abstract
Aim To assess specific clinical criteria in patients with uveitis that are related to signs of sarcoidosis on high-resolution computed tomography (HRCT) of the chest.
Methods Retrospective study of 50 consecutive patients with uveitis who were referred for chest HRCT because of suspicion of sarcoidosis. Clinical characteristics, laboratory findings, chest radiographs and chest HRCT scans were retrieved. HRCT scans were reassessed for signs of sarcoidosis. Mann–Whitney and Fisher exact test were used for data analysis.
Results Ten of 50 (20%) uveitis patients referred for HRCT demonstrated signs of sarcoidosis on HRCT. The median age of these patients was significantly higher than those patients with a negative HRCT (71.1 vs 44.7 years, p=0.002). The presence of peripheral chorioretinal punched out lesions and posterior synechiae were significantly related to an abnormal HRCT scan.
Conclusion Increasing age, presence of peripheral multifocal chorioretinitis and posterior synechiae were associated with an abnormal HRCT scan.
- Uveitis
- sarcoidosis
- CT
- multifocal chorioretinitis
- posterior chamber
- inflammation
- imaging
- diagnostic tests/investigation
Statistics from Altmetric.com
- Uveitis
- sarcoidosis
- CT
- multifocal chorioretinitis
- posterior chamber
- inflammation
- imaging
- diagnostic tests/investigation
Introduction
Sarcoidosis is a relatively common systemic disease with a life-time risk of 0.85% for Caucasians and 2.4% for black individuals in USA.1 The cause of sarcoidosis is unknown, and a histological proof is required for the definitive diagnosis. The most commonly affected organs are mediastinal and hilar lymph nodes (50–80%) and the lungs (20–50%). Respiratory tract involvement occurs in nearly all sarcoidosis patients.1 2 Skin and eyes are also frequently involved.3 Uveitis is present in approximately 25% of sarcoidosis patients depending on the population studied.4–6
The correct and timely diagnosis of sarcoidosis in uveitis patients is important, since it determines the treatment strategy in this often chronic and potentially blinding ocular disorder. Suspicion of ocular sarcoidosis in patients with uveitis is usually based on clinical findings and is further supported by laboratory (serum angiotensin-converting enzyme (ACE)) and radiological tests (chest x-ray (CXR), high-resolution computed tomography (HRCT)); if possible, a biopsy is taken from affected tissues. The superiority of HRCT over CXR for detecting signs of sarcoidosis is well established, but HRCT comes with the disadvantages of a higher radiation dose and higher costs.7–10 The value of HRCT of the chest in the diagnostic workup of ocular sarcoidosis is not yet known, and it remains uncertain which patients to refer for HRCT evaluation.
In the present study, we assessed which clinical and laboratory characteristics in patients with uveitis are related to signs of sarcoidosis on HRCT of the chest.
Methods
In the present study, we included all 50 chest HRCT scans of patients with uveitis and a suspicion of sarcoidosis performed between August 2006 and September 2008. The ethical review board of the University Medical Center Utrecht approved the study; informed consent was not required.
Medical data of these 50 patients were retrospectively reviewed. We registered age, gender, comorbidity, current treatments, duration of uveitis and various clinical characteristics including location of the uveitis, presence of posterior synechiae, vitritis, papillitis, vasculitis, cystoid macular oedema, peripheral multifocal chorioretinitis and intraocular pressure. Anatomical location was classified according to the Standardisation of Uveitis Nomenclature (SUN) criteria.11 Intraocular pressure above 22 was considered elevated. All patients had been suspected for the diagnosis of sarcoidosis on the basis of their ocular manifestations. Due to the retrospective character of this study, next to the clinical suspicion of sarcoidosis, no systematic clinical criteria for performing the chest HRCT scans were employed. We also collected chest radiographs obtained within 3 months before the chest HRCT, results of bronchoalveolar lavage (BAL), biopsies and laboratory data (ACE; ESR; c-reactive protein, CRP; leucocyte count). These specific tests were not available for all patients.
All patients underwent chest HRCT scanning following a routine protocol on a 16-detector-row CT scanner (MX8000 IDT or Brilliance-16, Philips, Cleveland, Ohio) or a 64-detector-row CT scanner (Brilliance-64, Philips, Cleveland, Ohio). Inspiratory scans were acquired in a caudocranial direction using 130 mAs and 120 kVp with a slice thickness of 1 mm (16-detector-row scanners) or 0.9 mm (64-detector-row scanner) and an increment of 0.7 mm. Intravenous contrast (90 ml injected at 3 ml/s, followed by a flush of 25 ml normal saline at 3 ml/s), was given in all patients to optimise visualisation of lymph nodes.
The scans were re-evaluated by one observer who did not know the patients' signs and symptoms other than the presence of uveitis. The original HRCT report and other test results were not available to the observer. In case of a different opinion from the original report, a specialised chest radiologist was consulted. Criteria that defined HRCT as positive for sarcoidosis were: lymph nodes at left and right hilum and mediastinum with a short-axis diameter greater than 1 cm, perilymphatic pulmonary nodules and other parenchymal lung abnormalities characteristic of sarcoidosis.7 12–16
Data were analysed using SPSS 12.0 (SPSS, Chicago). Characteristics of patients with a positive HRCT were compared with characteristics of patients with a negative HRCT. The Mann–Whitney U test was used for continuous variables and the Fisher exact test for categorical variables. Data are given as mean±SD unless indicated otherwise. A p value of <0.05 was considered significant.
Results
General characteristics of the included patients are illustrated in tables 1, 2. Posterior and panuveitis was present in 43 of the 50 patients. In patients with positive HRCT, all 10 had posterior and panuveitis.
Characteristics of patients with a positive versus a negative (HRCT) scan
Ophthalmological findings in patients with a positive versus a negative high-resolution computed tomography (HRCT) scan
The HRCT scans demonstrated signs of sarcoidosis in 10 patients (20%); nine showed only lymphadenopathy (stage I), and one showed lymphadenopathy and lung nodules (stage II). None of these patients had pulmonary complaints. There were no discrepancies between the HRCT reassessment and the original HRCT report, demonstrating that signs of sarcoidosis were relatively easy to assess with our HRCT protocol. Four of the patients with an abnormal HRCT had a chest radiograph within the 3 months before the HRCT. Only one of these chest radiographs (25%) was initially reported as being suspicious for sarcoidosis. Among the 40 patients with a normal HRCT, 10 received a chest radiograph, two of which were initially reported as showing possible hilar enlargement in one and possible hilar enlargement and interstitial lung disease in the other. In both patients, the subsequently ordered HRCT to confirm or exclude the possible CXR findings ruled in both patients the presence of hilar lympheadenopathy and pulmonary disease out.
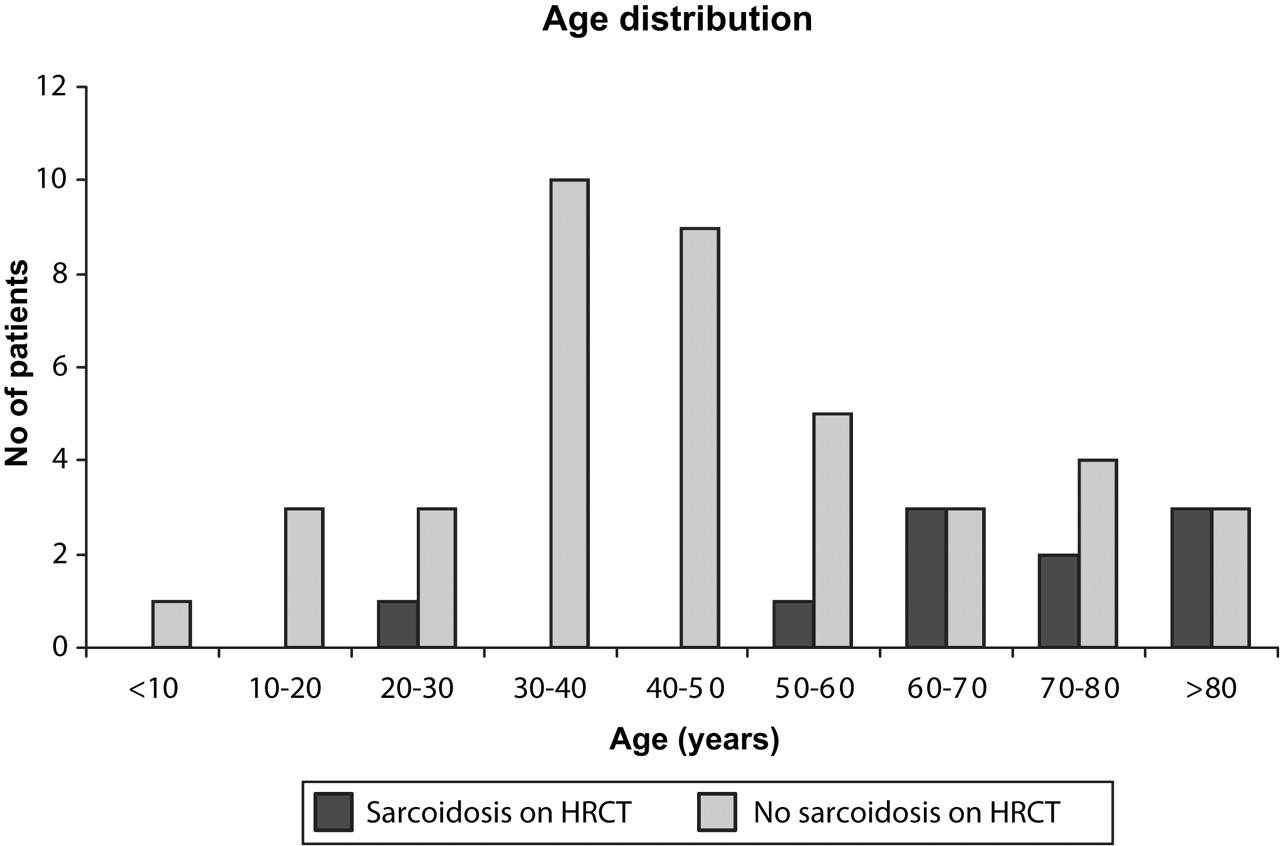
The characteristics of patients with normal and abnormal HRCT scans are presented in table 1. The age of the patients with an abnormal HRCT was 69±17 (median 71.1) years and with a normal HRCT 47±19 (median 44) years (p=0.002). Of the 13 female uveitis patients older than 50 years, six (46%) had an abnormal HRCT scan. The age distribution of patients with positive and negative scan outcomes is presented in figure 1. Gender was not significantly associated with an abnormal HRCT. None of the recorded laboratory data were related to an abnormal HRCT. Serum ACE (normal range 7–20 U/l) was within the normal range in 80% of the patients with an abnormal HRCT and in 90% of patients with a normal HRCT.

{kind=link}
Age distribution for patients with a positive and a negative high-resolution computed tomography (HRCT) scan. Age distribution differed significantly between the groups, Mann–Whitney U test p=0.002.
Ophthalmological signs for patients are presented in table 2. The presence of peripheral multifocal chorioretinitis (p=0.01) and posterior synechiae (p=0.05) was significantly associated with an abnormal HRCT. Duration of symptoms or other specific ophthalmological features were not associated with an abnormal HRCT. There were no differences in comorbidity between the HRCT positive (40% had one or more comorbidity) and negative groups (42% had one or more comorbidity). Seven patients with a positive HRCT were referred to a pulmonologist. In five, the diagnosis of sarcoidosis was confirmed by biopsy, in one patient the BAL was suggestive of sarcoidosis, and in one patient no further confirmation was attempted. Of the 10 patients with an abnormal HRCT, two patients received systemic treatment with corticosteroids (oral/systemic) and methotrexate (due to severe ocular involvement), while the others were treated locally and/or by periocular steroid injections.
The final diagnosis of 40 patients with a normal HRCT scan included infectious disease (n=5), Harada disease (n=2) and neuromyelitis optica (n=1); in the remainder, the cause was not established (n=32).
Discussion
In our series, elderly age, presence of peripheral multifocal chorioretinitis and posterior synechiae were significantly associated with HRCT findings suggestive of sarcoidosis.
In most studies on ocular sarcoidosis, two age peaks were noted: first between 20 and 30 years (mostly acute form) and around 60 years (chronic form). The affected patients were predominantly females.6 17 18 We found that HRCT scans were predominantly positive in elderly patients. Kaiser et al8 also noted that 62% of 52 consecutive uveitis patients referred for HRCT were older than 60 years. It may be possible that young patients with ocular sarcoidosis are diagnosed by different means and without the use of HRCT (different clinical presentation, positive CXR and/or tissue biopsy). This hypothesis is in accordance with the more frequent prevalence of Löfgren syndrome at young age and its frequent association with various systemic symptoms, pulmonary involvement and concurrent anterior uveitis.19 In contrast, sarcoidosis at an elderly age was more frequently associated with posterior uveitis and might be accompanied by a less frequent pulmonary involvement.20
Peripheral punched out lesions in the retina are characteristic lesions of peripheral multifocal chorioretinitis, an ocular disorder already previously linked to sarcoidosis in older female patients.21 22 In the present series, the positive HRCT findings were frequently noted in patients with this typical clinical disorder.
Posterior synechiae are typical for chronic anterior uveitis and were frequently found in chronic types of sarcoidosis.23–25 Several laboratory tests were reported to be typical for sarcoidosis, including serum ACE and calcium levels.25–27 In our series, however, none of the evaluated tests was found to be associated with an abnormal HRCT, which might be due to a limited systemic activity of the disease in patients and/or related to the limited number of patients included.
The value of CXR and HRCT in patients with uveitis has been debated,8–10 18 and the higher accuracy of HRCT is generally accepted. Kaiser et al8 examined 30 elderly women with chronic iritis, vitritis or choroiditis of unknown cause using HRCT in all and CXR in a subset of 25 patients. Eight of 25 (32%) had an abnormal CXR, while HRCT was abnormal in 17 of 30 (57%) patients. Chung et al18 studied 60 uveitis patients with biopsy-proven sarcoidosis, of which 44 underwent chest HRCT and CXR. CXR was abnormal in 22 (50%) and HRCT in 42 (95%). Of the 60 patients, 68% first presented at the ophthalmology clinic, and the others had extraocular presenting symptoms. The age peak was in the sixth decade; no gender differences were noted. Our manuscript adds to the paper by Chung et al,18 since we selected patients suspected of sarcoidosis, while Chung et al18 studied proven sarcoidosis cases, and in addition differences between European and Chinese populations might exist. As an extension to the work by Chung et al,18 we studied laboratory tests and specific ophthalmological signs. Most of our patients did not undergo CXR within 3 months before or after the HRCT, and so we cannot compare the value of CXR with that of HRCT. The reason for the low number of CXR in our patients is unknown, but some patients might have had a radiograph in another hospital before the referral to our ophthalmology department or had a CXR more than 3 months before the HRCT. In addition, some ophthalmologists might prefer HRCT in some patients with a high likelihood of having sarcoidosis.
Despite the higher accuracy, HRCT is not advocated as a primary screening test, because of higher costs and higher radiation exposure.8–10 18 However, so far, a systematic study comparing the diagnostic value of CXR and HRCT in a large group of patients with uveitis is not available, and specific recommendations on the role of HRCT cannot be made. For clinical purposes and for a systematic study, it would be valuable to recognise specific clinical criteria associated with a high chance of positive HRCT findings. Our study suggests that the presence of peripheral multifocal chorioretinitis and posterior synechiae in an elderly patient are associated with positive HRCT scan findings.
Our study is limited by the fact that we had no systematic criteria to perform the HRCT scan in patients with uveitis. There might have been patients with uveitis that presented to an ophthalmologist in whom other tests (eg, positive chest radiograph) led to the diagnosis of sarcoidosis without the use of HRCT and others in whom the diagnosis of sarcoidosis might have been missed. A second drawback is the limited number of abnormal HRCT scans, which increases the likelihood of type II errors (ie, not finding any significant differences between HRCT-positive and HRCT-negative groups), while in a larger study the differences might have been significant. Therefore, caution is needed with the conclusion that specific tests, for example ACE, are not useful in uveitis patients.
We have shown that elderly patients with uveitis (especially with peripheral multifocal chorioretinitis and posterior synechiae) and without pulmonary symptoms can be diagnosed as having sarcoidosis. From the pulmonologist's point of view, there was no indication to treat patients with systemic medications. In our opinion, it is important to make the correct diagnosis of sarcoidosis even in patients with mild pulmonary involvement. The potential benefit for the patients includes the empirical knowledge of best treatment regimens, more information on possible future development of the disease, complications and visual prognosis. In addition, it might prevent unnecessary diagnostic procedures in case of development of systemic manifestations. The costs of the examinations need to be compared with the potential benefit for the patients, and only a future study, which would systematically compare the outcome of CXRs and CT, might determine the correct diagnostic strategy and the exact role of the CT in diagnosing the patients with uveitis.
In conclusion, our study shows that in patients with uveitis, an older age, presence of peripheral multifocal chorioretinitis and posterior synechiae increase the probability of HRCT findings suggestive for sarcoidosis.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the ethical review board of the University Medical Center Utrecht approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance