Article Text

Abstract
Aim To assess the efficacy and safety of ranibizumab in the treatment of choroidal neovascularisation (CNV) caused by pathologic myopia (PM).
Design Prospective, multicentre, interventional case series.
Methods 40 eyes of 39 consecutive patients with PM and CNV were treated with ‘on demand’ intravitreal injection of ranibizumab 0.5 mg. Final best corrected visual acuity (BCVA) and its change from baseline were the main outcome measures. Changes in optical coherence tomography (OCT) central retinal thickness (CRT) were a secondary outcome.
Results Mean age was 53±13 years and mean refractive error –13.5±6.5 D. Median follow-up was 13.3±2 (range 12–18) months. Fifteen eyes (37.5%) had previously been treated with photodynamic therapy (PDT). The mean baseline logarithm of the minimum angle of resolution (logMAR) BCVA (Early Treatment Diabetic Retinopathy Study (ETDRS) vision chart) was 0.68±0.34 (Snellen equivalent 20/131) and 21±16 letters. The final mean logMAR BCVA was 0.27±0.2 (p = 0.008) (20/42) and 40.5±14 letters (p = 0.01). Mean final VA improved in 82.5% of patients, in 60% by 3 or more lines (median number of lines gained 2.9). Even six out of seven cases of low vision (≤1.1 logMAR) at the final examination has improved vision. Mean OCT CRT reduced from 218±70 to 175±46 μm (p 0.02). Age and previous PDT did not influence the results (p>0.05). The mean number of injection was 2.8±1.2 (range 1–6). No ocular or systemic side effects were observed.
Conclusion Ranibizumab was an effective treatment for stabilising and improving vision with a low number of injections in 92.5% of patients with myopic CNV in a long-term follow-up.
- Pathological myopia
- choroidal neovascularisation
- ranibizumab
- intraocular injection
- anti-VEGF drug
- drugs
Statistics from Altmetric.com
Introduction
Choroidal neovascularisation (CNV) is the main cause of acute vision loss in pathologic myopia (PM).1 2 The natural course of the disease accounts for low visual acuity (VA) (20/200) in 44–60% of the patients after 24 months. Laser photocoagulation is no longer used in juxtafoveal CNV because of large retinal scars increasing over time.3 Photodynamic therapy (PDT) with verteporfin may stabilise VA and significantly reduce visual loss in eyes with subfoveal and juxtafoveal CNV PM.4–6 Nevertheless the results show a decrease of VA in up to one-third of the eyes with subfoveal CNV and only 6% of the eyes gain more than three lines in juxtafoveal form.6 Meanwhile, the widespread use of anti-VEGF drugs in the treatment of CNV due to age-related macular degeneration (AMD) has enabled the development of new therapeutic strategies.
The use of off-label bevacizumab in CNV related to PM has been evaluated in a few clinical non-randomised clinical trials with a maximum follow-up period of 12 months.7 8 Few reports about ranibizumab show short-term efficacy in maintaining vision.9–12
We report the results of a 12-month prospective study in patients with PM who were treated with intravitreally administered ranibizumab 0.5 mg for CNV.
Materials and methods
Forty eyes of 39 patients with CNV related to PM were consecutively enrolled in this open-label, multicentre, non-randomised, prospective case series. They were treated with an off-label intravitreal administration of ranibizumab 0.5 mg, regardless of lesion location.
Inclusion criteria were: (1) highly myopic eyes, spherical equivalent greater than –6 D; (2) posterior pole myopic retinal changes (lacquer cracks, chorioretinal atrophy, papillary crescent, posterior staphyloma); (3) fluorescein angiography (FA) detection of the subfoveal or juxtafoveal CNV; (4) best corrected VA (BCVA) >20/400 at baseline; (5) duration of symptoms no longer than 4 weeks before enrolment; (6) minimum follow-up of 12 months; (7) clear ocular media.
Exclusion criteria included: (1) post inflammatory macular changes; (2) extrafoveal CNV; (3) age-related macular alterations; (4) refractive media opacities; (5) presence of other maculopathies as diabetic retinopathy or retinal vascular occlusion; (6) history of recent myocardial infarction or other thromboembolic events; (7) other previous intravitreal drugs injections; (8) ocular hypertension or glaucoma.
Previous PDT was not considered as an exclusion criterion if administered more than 3 months before enrolling. However, no additional PDT session was performed during the follow-up and treatment options included either ‘on demand’ ranibizumab intravitreal injections or observation.
BCVA was recorded using the Early Treatment Diabetic Retinopathy Study (ETDRS) chart at 4 m distance using a logarithm of the minimum angle of resolution (logMAR) scale: results were recorded as logMAR values and the number of letters read. At the baseline and at every examination, all patients underwent the standard ocular examination with ETDRS VA evaluation, biomicroscopy, tonometry and optical coherence tomography (OCT) evaluation (Stratus OCT 4.01; Carl Zeiss Meditec, Inc., Dublin, California, USA). Retinal fluorescein angiography (TRC-50/IMAGEnet H 1024 system; TOPCON, Tokyo, Japan, and/or Heidelberg Retina Angiograph 2, Heidelberg Engineering, Heidelberg, Germany) was performed at baseline within the 15 days prior to the initial visit, and subsequently according to the judgement of the ophthalmologist during the follow-up period.
The retinal thickness map analysis program was applied with the extrapolation of data from six diagonal 6 mm radial line scans. The scans were reviewed and manually calliper-assisted measurements were used in case of delineation errors. An SD greater than 10% of the macular thickness was considered out of range and scans were repeated or rejected. A decrease of 10% thickness in comparison with the baseline was considered as a reduction, while an increase of 10% as an amount.
The off-label use of the drug and its potential risks and benefits were discussed extensively with all the patients.
Patients received an initial dose of 0.5 mg (0.05 ml) of ranibizumab using the standard injection procedure in a surgical room.13 Patients were re-examined the day after treatment. All patients were given detailed instructions and asked to call promptly if any significant changes in vision occurred. The patients were examined on a monthly basis, after the injection for the first 3 months, and monthly or quarterly thereafter, according to the judgement of the specialist.
Re-treatment was performed if any of the following conditions occurred: decrease in BCVA and/or increase of metamorphopsia; new retinal haemorrhage; increase of retinal/subretinal fluid or retinal thickness on OCT; CNV leakage on FA images.
The primary outcome was considered to be the improvement of VA with a minimum of 5 letters (one ETDRS line) or the stabilisation of VA. Secondary outcome was the changes in OCT CRT. Alpha level (p) was fixed at 0.05, as a probability of 95%. Statistical analysis was performed by means of a non-parametric Wilcoxon signed-ranks test and two-tailed t test, provided by SAS (Statistical Analysis Software) for Windows 8.0 (Microsoft Corp., Redmond, Washington, USA), in order to evaluate BCVA and OCT CRT changes. The influence of age, previous PDT and lesion size on VA change were analysed by means of multivariate linear regression.
VA changes from baseline were defined as improved if an increase of 1 ETDRS line or 5 letters was registered, or worsened if there was a decrease of 1 line; otherwise VA was considered unchanged.
Data are presented as mean, SD, median, and percentage (%).
Results
Thirty-nine patients were enrolled in this study and forty eyes were treated. Twelve patients were men and 27 were women; the mean age at the initial examination was 53 (SD 13, range 32–80) years. Mean refractive error was –13.5 (SD 6.5, range – 6 to – 28) D. In 29 eyes the CNV was subfoveal (72.5%) and in 11 eyes it was juxtafoveal (27.5%). Fifteen eyes (37.5%) were previously treated with PDT and 23 (57.5%) were not. The mean ETDRS BCVA at baseline was 0.67 logMAR (SD 0.34, range 1.1–0.1, Snellen equivalent 20/131) and 21 (SD 16, range 0–50) letters The mean follow-up was 13.3 (SD 2, range 12–18) months. All the patients completed a 12-month follow-up, nine of them being followed-up for 18 months. Clinical data at baseline are reported in table 1.
Baseline characteristics of patients at the study entry
Post-treatment visual outcomes are displayed in table 2. The mean BCVA was stable or improved during post-treatment follow-up with a mean final VA of 0.27 logMAR (SD 0.2, range 1.1–0.0, Snellen equivalent 20/41) and 40.5 letters (SD 14, range 0–55) at 12 months after enrolling (p=0.008 for logMAR, 0.01 for letters) (figure 1).
Outcomes at the end of the follow-up
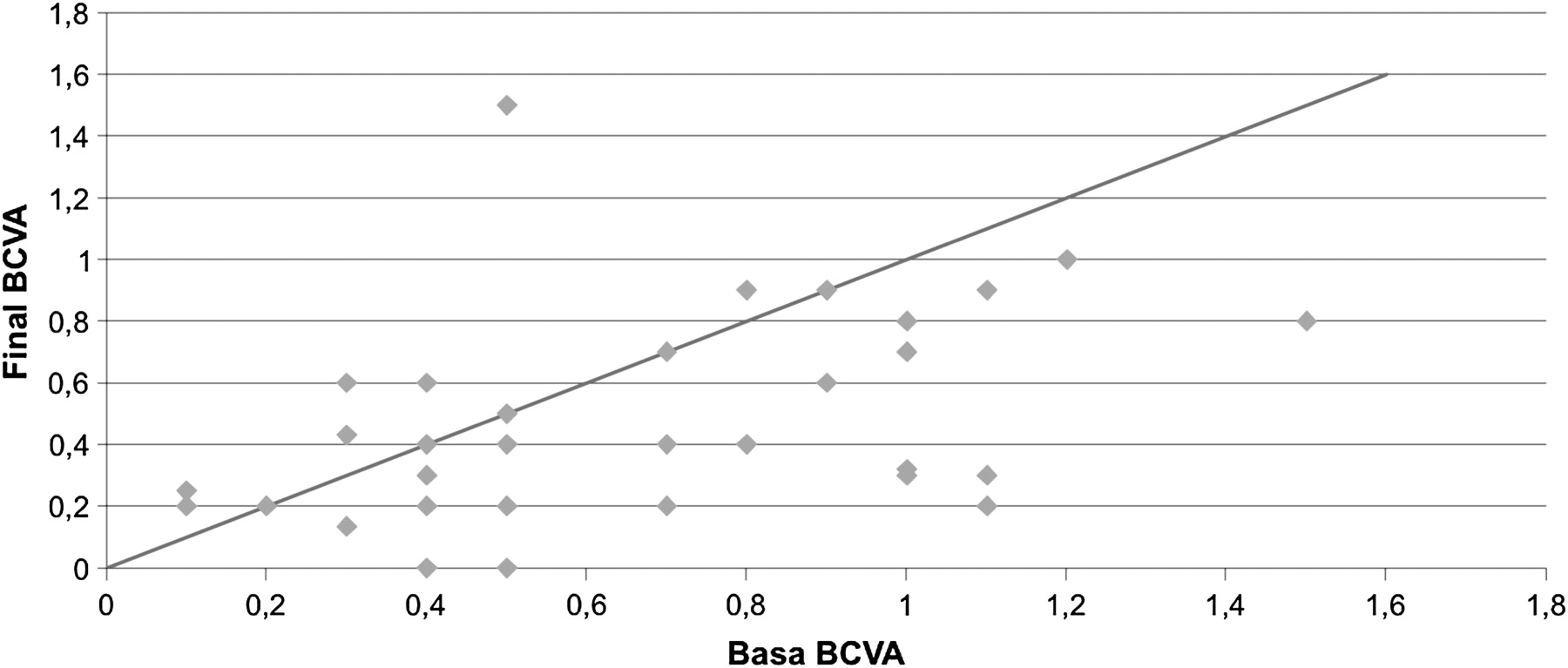
Results are presented as a scatterplot of basal and final best corrected visual acuity (BCVA). The scatterplot presents the distribution of BCVA in logarithm of the minimum angle of resolution (logMAR) units before intravitreal injection and the final BCVA at the end of the follow-up. The values below the red line show the eyes with a visual improvement; in addition, most of the remaining patients, even if not improving, show fairly stable visual acuity after the treatment (dots close to the diagonal line).
The final BCVA, compared with baseline, improved in 32 out of 40 eyes (80%), decreased in three eyes (7.5%) and remained stable in five eyes (12.5%). In the eyes showing improvement, the median number of lines gained from baseline was 2.9 (range 1–8), and 19 out of the 32 (59.4%) patients improved by 3 or more lines: nine eyes (28%) improved by 1 line, four eyes (12.5%) by 2 lines. Three eyes worsened in VA despite therapy: one eye lost 1 ETDRS line, one eye 2 lines and the third case lost 3 lines. However, they maintained BCVA between 0.2 and 0.6 logMAR. Seven eyes had BCVA lower than 1 logMAR (range 1.1–1.5) at the time of enrolment, but at the end of the follow-up period only one eye was lower (1.5 logMAR): that was its exact BCVA at baseline, so it was considered as stabilised.
Mean central macular thickness analysed by OCT showed a reduction in all cases, from 218.9 (SD 70) to 175 (SD 46) μm (p=0.02) (figure 2).

{kind=link}
{kind=link}
Demonstrative fluorescein angiography (FA) and optical coherence tomography (OCT) of three patients (indicated as 1, 2, 3). A1–3, middle/late phase FA before treatment, showing leakage from subfoveal neovascularisation. B1–3, 12–14 months after treatment, showing resolution of leakage and peripheral annular window effect and central staining. C1–3, OCT scan before treatment showing intraretinal hyper-reflective lesion, in case 2 and 3 associated with neurosensory detachment and/or intraretinal fluid. D1–3, OCT scan 12-15 months after beginning of treatment showing hyper-reflective waveform changes of retinal pigment epithelium band associated with complete resolution of both the neurosensory detachment and intraretinal fluid. Arrow on images (A) indicates the OCT B-scan orientation min, minutes.
When analysing VA results in relation to refractive errors, age and lesion size, no statistical accordance was found. Eyes with an initially poor VA (lower than 1.1 logMAR) did not differ statistically in visual improvement from those with initially good VA.
Considering the entire group, the mean number of injections was 2.8 (SD 1.2); the number of treatments varied from one to a maximum of six.
The eyes previously treated with PDT were compared with the naive ones. No statistical accordance was found (p>0.05) regarding age, refractive errors, lesion size, BCVA, central macular thickness and the response to a ranibizumab injection. In addition the mean number of injections (2.56 vs 2.6) was similar. The mean number of letters gained was 31 vs 34 (p = 0.2).
No ocular or systemic side effects were observed; in particular, neither retinal tears nor detachment occurred during the observation.
Figure 2 shows FA and OCT changes from basal observation to the last examination.
Discussion
Treatment of CNV in PM is still open to debate and should be further defined. Currently laser photocoagulation is the standard treatment for extrafoveal CNV,14 while PDT is the only approved therapy for subfoveal lesions showing significant visual and anatomic benefits.4–6 However, 2–3 year observational reports2 15 fail to demonstrate the effectiveness of PDT in stabilising vision or reducing severe loss of vision versus a placebo. Moreover, in juxtafoveal form, about 25% of eyes had experience of a decrease in vision and only 6% of the eyes gained 3 or more lines.6
Vascular endothelial growth factor A (VEGF-A) has been implicated as a major mediator responsible for subretinal neovascularisation in several ocular diseases and it is now the main target for therapy in exudative AMD. Ranibizumab and bevacizumab are the most diffused anti-VEGF drugs for AMD complicated by CNV, giving a pan-vascular endothelial growth factor blocking.16–18 The effect of anti-VEGF drugs on aqueous VEGF and PEDF19 and such therapy is now having wide clinical support.20 Previous studies on bevacizumab in myopic CNV have shown very promising results.7 8
Ikuno et al,7 in a retrospective analysis, enrolled 63 myopic eyes and treated them ‘on demand’, disregarding the CNV clinical form, VA or timing of symptoms at enrolment. The mean number of injections was 2.4±1.4: 40% of patients had improved vision (27% from 3 to 6 lines, 13% to 6 or more lines), while 56% remained stable, with a gain or loss of less than three lines. Three patients (5%) lost more than 3 lines in 12 months because of enlargement of macular atrophy.
Gharbiya et al,8 in a 1-year follow-up prospective study on 20 eyes, demonstrated that 1.25 mg intravitreal bevacizumab can improve vision significantly and reduce macular thickness at the OCT and angiographic leakage in 95% of cases. In 90% of subjects vision improved by 10 or more letters and in 70% by 15 or more letters. None of the patients experienced a worsening of VA with respect to the baseline condition. The mean number of injections was four, ranging from three to seven, starting with a loading dose.
Very few papers report clinical experience with ranibizumab.9–12Explanations could be that PDT has been stated as on-label treatment and the different costs between anti-VEGF drugs.
Silva et al9 retrospectively evaluated the efficacy of ranibizumab in myopic CNV in 26 eyes followed up for 3–6 months, while Kostantidinis et al 10 prospectively enrolled 14 eyes and followed them for up to an average of 8 (range 3–16) months. They showed a positive trend in vision recovery, stable vision after the third month, and a lower reduction in OCT macular thickness.
Monés et al11 prospectively enrolled 23 patients with CNV related to PM, treated ‘on demand’. Almost 70% of patients gained at least 1 line of visual acuity in a 1-year follow-up, with a mean number of injections of 1.5. Intravitreal ranibizumab has also been suggested as first line treatment in 16 patients by Lai et al,12 who chose the use of a loading dose in their protocol: they observed a gain in vision in 75% of patients and only one patient needed retreatment during the follow-up of 12 months.
In our paper we confirm the efficacy of intravitreal injection in myopic CNV. The final mean VA improved in 32 out of the 40 eyes considered and was stable in five (92.5%). The median number of lines gained was 2.9 from the baseline. About 60% of all patients improved by 3 or more lines. Ranibizumab stabilised BCVA to the range of legal blindness in one eye only, while it allowed six eyes to recover to mild low vision level (range 1–0.5 logMAR). Even in those cases where BCVA worsened, it stabilised between 0.6 and 0.2 logMAR.
We did not notice any difference in visual outcome between eyes previously treated with PDT and naive eyes. The mechanisms of action of PDT and ranibizumab are different, and therefore where PDT is unsuccessful, anti-VEGF blocking is always a treatment opportunity. The role of PDT in promoting fibrosis should, however, be considered21 in evaluating visual prognosis.
Which is the most effective regimen to adopt in non-AMD CNV still remains uncertain.
Clinically myopic CNV differs from AMD-CNV, the former being slower in natural evolution with a variable visual outcome.2 The role of pigment epithelium and the release of different VEGF-related factors are probably the key to the differences.22 Patients are often young and therapies can be more effective because of the healthy retinal pigment epithelium (RPE) that is able to react adequately, creating a barrier to the development of CNV. The same results were observed after PDT treatments in the past.5 6 23
For these reasons we think that, in myopic CNV, the ‘on demand’ regimen may be preferable with respect to the loading phase; this would lead to a lower number of injections, lower risks and less expense. At present, there has not been a controlled trial assessing the best modality of treatment in myopic CNV; however, among the papers published, some indicate very good results with the on demand regimen, the final mean number of injection being very low. In our paper we observed a mean number of injections of 2.8 in the first year, indicating a better prognosis in myopic CNV than in AMD (5.6 reported in the Prospective OCT Study With Lucentis for Neovascular AMD (PrONTO) study).24
In our series, the number of treatments was not related to poorer final VA, in contrast with other reports about bevacizumab.8
Even though, in our series, OCT central foveal thickness showed statistically significant reduction after treatment (p = 0.02), the role of OCT needs to be clarified.
In myopic patients OCT may be considered useful to better define the diagnosis of CNV, excluding the presence of vitreoschisis with foveal alterations, tractions and small macular holes. However, since PM-CNV can often have minimal leakage and choroid is usually very thin, OCT macular thickness can be irrelevant and the presence of fluid very scarce (see figure 2, case 1). Furthermore, the Stratus OCT can give a large number of artefacts and therefore needs a very skilled examiner.
New spectral domain OCTs will give us more and better clinical information, but at the present, considering also that the Stratus OCT is the gold standard in current scientific reports, in our opinion we should be very careful in carrying out a treatment or a retreatment of patients on the basis of OCT only. In our experience metamorphopsia is the leading symptom and should be highly considered in reaching a decision.
Several reports underline that refractive error, lesion dimension and age can influence treatment response, both for PDT and for anti-VEGF drugs.5 8 23 However, in our cohort of patients, statistical analysis did not show any correlation with age, refractive error or previous PDT. This issue surely deserves more investigation.
The safety of the drug was confirmed by our report. None of the patients developed any ocular or systemic side effects associated with intravitreal ranibizumab.
The efficacy and safety of a new drug should be tested on a large population as was done in AMD trials; this has seldom been done for myopic population. When evaluating literature about myopic CNV and anti-VEGF drugs, our series is large and can be accepted as representative of this population. We hope that a larger multicentre trial will offer stronger support to clinical practice. A further limitation of our paper is follow-up extension: we agree that clinical trial or observational studies should have at least 12 months of follow-up or 24–36 months in order to really compare results with natural history. The study lacks a control group: however, we consider it to be ethically unacceptable to perform a comparison with randomised untreated patients, since therapies have greatly improved the prognosis of the disease.
Conclusion
International trials with ranibizumab negated any subgrouping of CNV and therefore treatment with anti-VEGF drugs is equally suggested for any form or localisation of CNV in AMD. Anti-VEGF drugs give a high chance of stabilising and improving vision that has otherwise deteriorated because of CNV. These drugs are therefore currently used in any form of CNV, and also in off-label settings.20
In our experience, intravitreal injection of ranibizumab appears to be very effective in the treatment of myopic CNV, with a high proportion of patients reporting an improvement in vision and a mean of three injections in the first year. Treatment is also able to avoid legal blindness. The correct regimen of treatment, as well as retinal and choroidal changes with time, still need to be defined.
Acknowledgments
We thank Giuseppe Bianco for his help in managing surgical times.
References
Footnotes
Competing interests None to declare.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.