Article Text

Abstract
Background/aims The aim of this study was to evaluate the long-term corneal toxicity of topical chemotherapy with 1% 5-fluorouracil (5-FU) as a sole or adjuvant treatment of ocular surface squamous neoplasia (OSSN).
Methods Forty-one consecutive cases of OSSN were included in this prospective study. Patients underwent topical chemotherapy with 1% 5-FU four times/day for 4 weeks (one course). Adjunctive courses were repeated until clinical and cytological tumour regression. Clinical confocal microscopy was used to check for 5-FU long-term corneal toxicity.
Results Mean follow-up was 89.7±14.4 months (range 63–122 months). Twenty-two patients (53.7%) underwent topical 5-FU as a sole treatment, and 19 patients (46.3%) as adjuvant and/or debulking therapy. The mean number of 5-FU cycles was 1.9 (range 1–5 cycles). Three tumours (7.3%) treated with 5-FU alone recurred during follow-up. Recurrences were successfully treated with additional 5-FU courses. Clinical confocal microscopy showed no long-term difference between the treated eye and fellow (control) eye in: endothelial cells count, pleomorphism and polymegatism, anterior stromal keratocyte density, sub-basal nerve plexus fibre number, density, and beadings and central cornea epithelium thickness (p=NS).
Conclusion Topical 5-FU, as a sole or combined therapy, must be considered a long-term safe and effective treatment for patients affected by OSSN.
- Ocular surface
- neoplasia
- drugs
- cornea
- conjunctiva
Statistics from Altmetric.com
Introduction
Ocular surface squamous neoplasia (OSSN) is a spectrum of diseases with the potential of visual loss and local morbidity.1 OSSN are traditionally seen in Caucasian older males or in lighter-skinned populations in tropical countries.1 2 Risk factors for this disease include: ultraviolet light exposure, petroleum products, cigarette smoking, human papillomavirus and human immunodeficiency virus infection.3 The term OSSN encompasses corneo-conjunctival intraepithelial neoplasia (CIN) and invasive squamous cell carcinoma (SCC).4 These lesions are commonly seen in the exposed corneo-conjunctival areas and described as being slightly elevated, variably shaped, relatively sharply demarcated from the surrounding normal tissues, accompanied by feeding blood vessels and having a pearly grey to reddish grey appearance.1 Surgical excision with adjunctive cryotherapy was formerly considered the treatment of choice.5 However, recurrence rates after surgery are significant, even when free surgical margins were achieved.5
Topical chemotherapy has become a valuable therapeutic option for the treatment of ocular surface tumours in the last decade. 5-Fluorouracil (5-FU), mitomicyn C (MMC) and interferon α2b (INFα) have been introduced, and are currently widely used, as both adjuvant therapy (to prevent tumour recurrence) and primary treatment of OSSN.6–8 Although many reports suggest a short-term safety of topical chemotherapy with 1% 5-FU, only few data were reported on a long-term basis.6 9 10 Moreover, morphological and morphometric analysis of corneal layers was never performed in vivo, at microscopic level, after topical chemotherapy. The aim of this study was to evaluate long-term corneal toxicity of topical chemotherapy with 1% 5-FU, as a sole or adjuvant treatment of OSSN, using clinical confocal microscopy (CCM).
Material and methods
This study complied with the tenets of the Declaration of Helsinki and was approved by the IRB of our Institution. Each patient was recruited from those referred to the Ophthalmic Oncology Unit of our departments and underwent a baseline full ophthalmological examination. Clinical and demographic characteristics were collected, including: age, gender, tumour location (cornea, conjunctiva, corneo-conjunctival) and tumour largest basal diameter. Adjunctive tumour clinical features such as nodularity, mutifocality, prominent vascularisation (presence of macroscopically evident tumour vessels or conjunctival feeder vessels) and fornix involvement were also reported.2 The tumour clinical aspect was documented by anterior segment photography. Cytological analysis (scraping technique) was obtained from all patients and reported as low-grade dysplasia (cells with enlarged nuclei, hyperchromasia and irregular contour of the nuclear membrane with increased nuclear/cytopasmic ratio) or high-grade dysplasia (pleomorphism of the nucleus with dyskeratotic cells.1 The presence of syncytial sheath, nucleoli and infiltration of inflammatory cells was reported as invasive SCC.1 Each patient was treated with 1% 5-FU as a sole or in a surgical combined approach. Our standard protocol consists of topical instillation of 1% 5-FU prepared in aqueous solution and administered four times a day during the course of 4 weeks (one course).6 9 Patients were instructed about possible 5-FU local side effects. After instillation of the eye-drops, the inferior lacrimal punctum was briefly occluded, and an eye ointment was applied on the inferior eyelid skin to minimise skin contact with the drug. A new medication bottle was used for one entire course and then returned to the pharmacy. Adjunctive courses were administered after 3 months of free interval and repeated until clinical and cytological tumour regression. Patients treated with topical chemotherapy as a combined treatment underwent wide surgical excision followed by cryotherapy to the cut edges of the conjunctiva. Alcohol epitheliectomy was performed for corneal involvement. Large tissue defects were managed by amniotic membrane reconstruction of the ocular surface. Topical chemotherapy was administered at least 3 weeks after surgery, following our standard protocol.6 9 Follow-up was performed monthly until clinical resolution, after 1, 3 and 6 months and every 6 months thereafter. Follow-up included full ophthalmological examination, slit-lamp biomicroscopy and anterior segment photography. Scraping cytology was also performed after 1 and 6 months of complete clinical tumour regression. Follow-up was longer than 5 years.
Corneal confocal microscopy
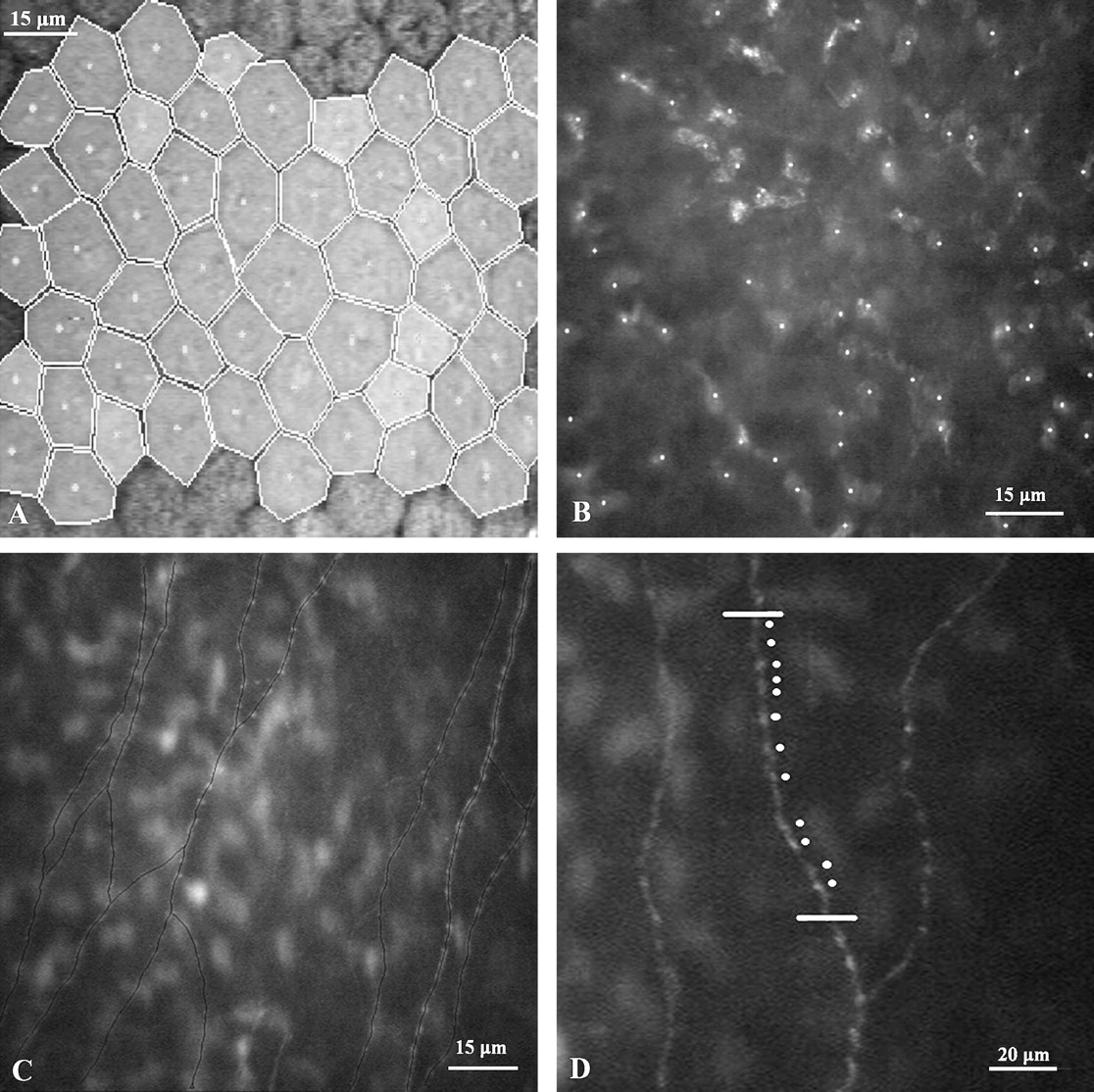
In vivo corneal multilayer analysis was performed using clinical confocal microscope Confoscan 4.0 (Nidek Co Ltd, Gamagori, Japan) equipped with a 40× immersion objective lens (Zeiss, Oberkochen, Germany) and the Z-ring adaptor system designed for full thickness examination of the cornea. Inclusion criteria were: patients affected by OSSN, treated with 1% 5-FU (as a sole or combined therapy), with follow-up longer than 5 years. Exclusion criteria were: any coexisting chronic cornea-conjunctival disease, unilateral cataract surgery, other mono- or bilateral intraocular surgery or refractive surgery, unilateral chronic use of preserved eye-drops, glaucoma therapy or other topical therapy. Confocal microscopy examination was performed according to a standard procedure.11–13 Endothelial cell density (number of cells/mm2), pleomorphism (percentage of hexagonal cells) and polymegatism (percentage of oversized cells) were automatically calculated selecting the best-focused image (figure 1A). Anterior stromal keratocyte density (cells/mm2) was manually calculated, selecting the first focused image of corneal stroma (figure 1B).11–13 Epithelium thickness was defined as the distance between the last focused image of the subbasal nerve plexus and the last focused image of the corneal epithelium, as described by Li et al.14 Subbasal nerve plexus was evaluated, choosing the best focused image of this structure.13 Nerve fibre density (μm/mm2), number of fibres (fibres/field) and number of beadings (beadings/100 μm) were quantified. Nerve fibres were traced using the Neuron J program, an image-processing computer tool, to outline nerve fibres from each corneal sub-basal nerve plexus frame (figure 1C).13 15 Nerve-fibre density was calculated for each image as the total length of the nerves (in micrometres) divided by the area of the image (0.132 mm2) and expressed as micrometres per square millimetre (μm/mm2).13 The number of nerve fibres was calculated as the total number of principal nerve trunks seen in the selected (best focused) image.13 The number of beadings was manually calculated as the number of well-defined hyper-reflective points per unit of length (100 μm) in a single nerve fibre, randomly selected from the best-focused fibres (figure 1D).13 The fellow eye was also evaluated and considered as a control.
{kind=link}
Corneal confocal microscopy analysis (using ConfoScan 4.0) in a patient treated with 1% 5-fluorouracil. Endothelial cells were automatically selected, marked and analysed by the software (A). Anterior stromal keratocyte density was manually calculated by the operator marking each on-focus keratocyte (B). Nerve fibres were analysed using the Neuron J program (C). The number of nerve beadings was manually calculated as the number of well-defined hyper-reflective points per unit of length (100 μm) in a single nerve fibre (D).
Statistical analysis
Data on corneal endothelium density, pleomorphism and polymegatism, keratocyte density, number and density of nerve fibres, beadings and epithelial thickness in treated eyes were compared with the data obtained in fellow eyes using the Student paired t test.
Results
Forty-one consecutive patients with a mean age at treatment of 65.5±10.2 years (range 44–88) were included. Tumour characteristics and cytological results are reported in table 1.
Demographic data, tumour characteristics and cytological results
Twenty-six patients were male (63.4%), and 15 were female (34.5%). The right eye was affected in 19 patients (58.6%) and the left eye in 22 (36.6%). Twenty-nine tumours (70.7%) were corneo-conjunctival in location, one (2.4%) was corneal, and 11 (26.8%) were conjunctival. The mean tumour largest basal diameter was 8.9±5.0 mm (range 3–25 mm). Baseline scraping cytology results were: low-grade dysplasia in seven cases (17.1%), high-grade dysplasia in 14 cases (34.1%) and squamous cell carcinoma in 20 cases (48.8%). Twenty-two patients (53.7%) underwent 5-FU as a sole treatment, whereas 19 patients (46.3%) underwent 5-FU as a surgical-combined approach. Of these, topical chemotherapy was used as a debulking treatment in one case (2.1%), as adjuvant therapy in 15 cases (36.6%) or as a double treatment (debulking+adjuvant) in seven cases (17.1%). Histological examination of all excised lesions confirmed baseline cytological diagnosis. Complete regression was achieved in all treated patients. Three patients (7.3%), treated with 5-FU as a sole therapy, developed early recurrences during follow-up. These patients were successfully re-treated with additional courses of chemotherapy. The mean number of 1% 5-FU courses before definitive regression was 1.9 (range 1–5). The mean follow-up was 89.7±14.4 months (range 63–122). The mean age of disease onset, mean chemotherapy courses, mean follow-up and rate of recurrences related to baseline cytology are reported in table 2.
Clinical and demographic characteristics related to baseline cytology
Confocal microscopy analysis of both eyes was successfully conducted in all patients. No significant differences were observed between treated eye and fellow/control eye in: endothelial cell density, endothelial pleomorphism and polymegatism, mean keratocyte density, mean corneal nerve density, mean sub-basal nerve fibres number/fields, mean nerve beadings number and mean epithelial thickness. Confocal microscopy analysis results are reported in table 3.
Confocal microscopy analysis
Discussion
The main treatment modality for OSSN remains wide surgical excision with cryotherapy (with accurate histological assessment of surgical margins) and amniotic membrane reconstruction for large tissue defects.7–10 However, the long-term local recurrence rate remains high, ranging from 15% to 52%, even when surgical margins of primary excision are free from malignant cells.1 The recurrence rate associated with surgery is probably due to the difficulty in establishing clinically tumour-free margins.7 Unless an intraoperative frozen-section technique is used, residual tumour cells may remain.5 16 Moreover, epithelial tumours of the conjunctiva can be multifocal or diffuse, rendering focal treatments less effective in eradicating these lesions.1 17 These data prompted us to introduce topical chemotherapy, as a sole or combined treatment, in a routine clinical setting.6 9
5-FU is a cell-cycle-specific pyrimidine analogue with cytotoxic properties due to its effect on both DNA and RNA.18 It was first synthesised in 1957 by Dushinski et al and was found to have significant activity against tumours of the gastrointestinal tract, head, neck and breast.18 19 This drug was originally known for its widespread use as an anticancer agent, but its ability to reduce fibroblastic proliferation and subsequent scarring has made it an important adjunct in ocular and periorbital surgery.18 5-FU acts on rapidly proliferating epithelial cells and was therefore used as a topical treatment for preinvasive OSSN as early as 1986.20 Many reports confirm the efficacy of topical chemotherapy with 5-FU as a sole or combined treatment of OSSN.3 6 9 17 21 Moreover, only transient, low to mild and self-limited side effects were reported.6 9–19 Poothullil et al, reviewing the use of topical medical therapies for ocular surface tumours, reported punctuate keratitis and hyperaemia as the only side effects of topical 5-FU. Other side effects included small epithelial defects, their accompanying discomfort and erythema of the eyelid skin.10 Topical corticosteroids were usually applied to improve tolerance during the treatment, and rarely (never in our experience) patients discontinued therapy because of 5-FU side effects.6 9 10 Although many reports suggest a short-term safety of topical chemotherapy with 5-FU, there are no data on a long-term basis.6 9 10
In vivo evaluation of the ocular structures at high magnification (to distinguish microscopic cell details) has always been a challenge for ophthalmic clinicians and researchers, but microscopic studies have, until recently, been limited to ex vivo investigation. Confocal microscopy was introduced in the clinical practice as a non-invasive tool to observe at high magnification the structure of human cornea and conjunctiva in vivo.11–13 CCM analysis extends, in vivo, the principles of biomicroscopy to the microscopic range, scanning tissue layer by layer, by changing the plane of focus of the detector source.11–13 Confocal microscopy was previously used to analyse in detail corneal pathological changes secondary to ocular surface disease,22 refractive surgery,23 chronic use of topical therapy,24 systemic disease12 and systemic pharmacological therapy25 with promising results.
Panda et al have recently analysed the effect of topical MMC on corneal endothelium in 25 patients affected by OSSN using endothelial specular microscopy. They reported that topical 0.04% MMC eye-drops do not significantly affect corneal endothelium but suggested that long-term data are mandatory.26 Moreover, this study has analysed only endothelium and not the other corneal layers. To the best of our knowledge, the present study is the first to focus on long-term safety of topical chemotherapy using full-thickness clinical confocal microscopy. These data, obtained in vivo in a fully non-invasive way, show no long-term corneal toxicity in eyes treated with topical chemotherapy with 1% 5-FU. Using clinical confocal microscopy, we have confirmed that 5-FU is selective for neoplastic cells, demonstrating no long-term pathological change in corneal endothelium, epithelium, stroma and sub-basal nerve plexus structures. These data, paired to clinical outcome of patients, suggest that topical chemotherapy with 1% 5-FU should be considered a long-term safe and effective method as a sole or combined treatment of selected OSSN.
References
Footnotes
This paper was partially presented at the International Congress of Ocular Oncology, 8–12 September 2009, Cambridge, UK.
Competing interests None.
Ethics approval Ethics approval was provided by the University of Padova, Padova, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.