Article Text

Abstract
Purpose To describe a new technique for transillumination photography of uveal melanoma and other intraocular tumours based on a simple modification of a standard digital slit lamp camera system.
Methods Transillumination imaging was performed with a digital slit lamp camera (Photo-Slit Lamp BX 900; Haag-Streit, Koeniz, Switzerland) modified by releasing the distal end of the background illumination fibre cable from its holder. The patient's eye was held open, and the head was positioned on the head and chin rest of the slit lamp. Transillumination was achieved by gently pressing the tip of the light fibre cable against the globe. The camera was then fired and the flash delivered through the cable while synchronising with the camera shutter.
Results This technique was applied in five patients with ciliary body or anterior choroidal tumours. Photographs were of good diagnostic quality, making it possible to outline the tumour borders and evaluate any ciliary body involvement. No patient experienced discomfort or negative side effects.
Conclusions We recommend this technique in all cases where transillumination and photographic documentation of intraocular tumours are considered important.
- Uveal melanoma
- transocular
- transpupillary
- transillumination
- photography
- imaging
- neoplasia
- pathology
- retina
- vitreous
Statistics from Altmetric.com
- Uveal melanoma
- transocular
- transpupillary
- transillumination
- photography
- imaging
- neoplasia
- pathology
- retina
- vitreous
Introduction
Transillumination is a simple and commonly used technique for the diagnosis and localisation of intraocular tumours.1 Cystic or atrophic lesions may transilluminate, while pigmented tumours such as uveal melanomas usually block the light. Transillumination is particularly useful in identifying the margins of a ciliary body or anterior choroidal melanoma, thereby facilitating the correct positioning of radioactive plaques in episcleral brachyterapy. Different methods and light sources have been used for preoperative as well as perioperative transillumination.2–5 Transillumination is usually performed using a fibre optic light source, and photographic documentation typically utilises an external camera with a macro lens. The limited light intensity requires a relatively long exposure time, and involuntary movements of the patient or the examiner make exact photographic documentation of the scleral tumour shadow difficult. The transillumination images tend to be both dark and blurred, making them unsuitable for the evaluation of tumour growth and preoperative planning of plaque placement in relation to episcleral landmarks. This report describes a new technique for transillumination photography of uveal melanoma and other intraocular tumours based on a simple modification of a standard digital slit lamp camera system.
Materials and methods
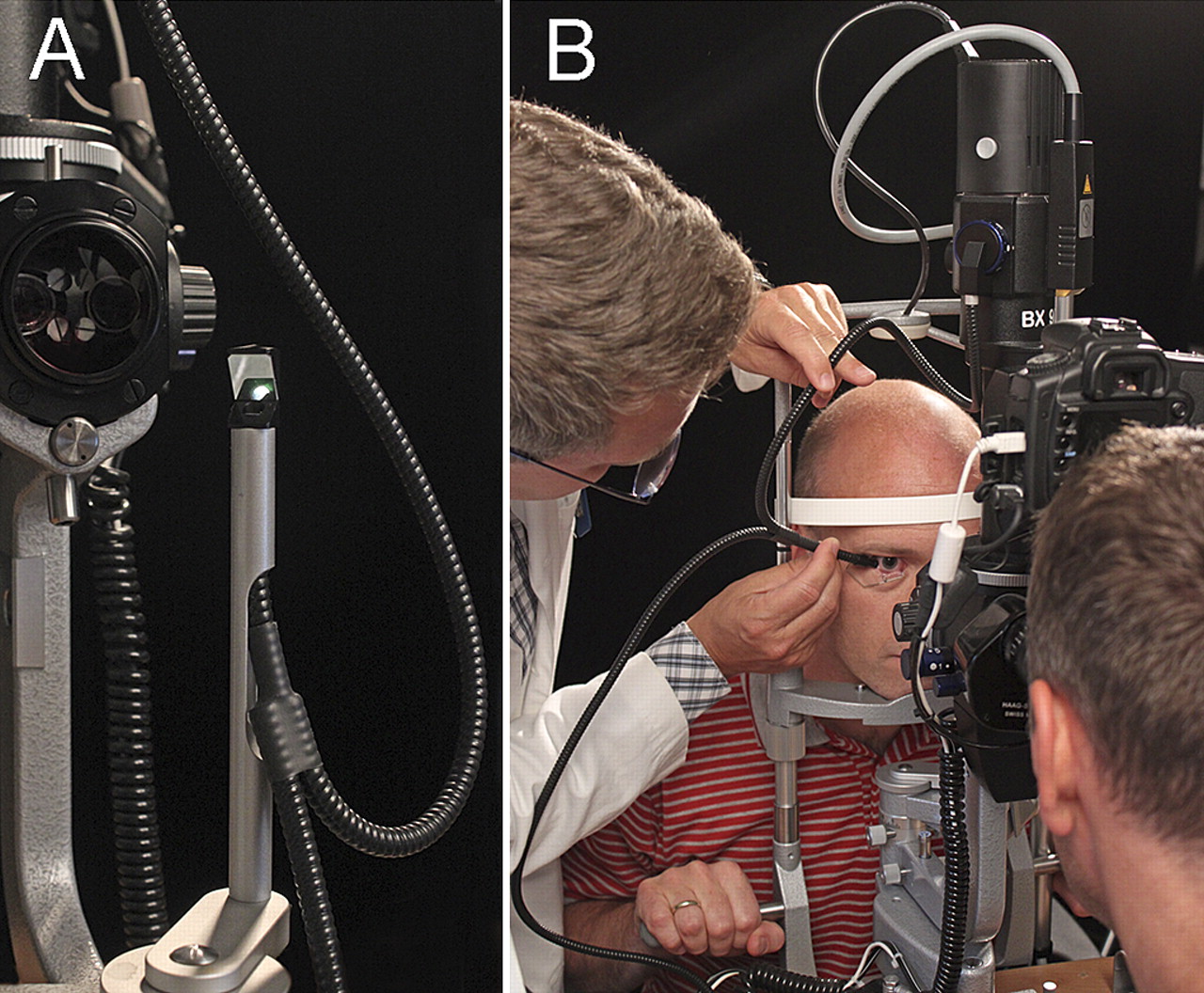
The transillumination imaging was performed with a digital slit lamp camera system, a Haag-Streit Photo-Slit Lamp BX 900 (Haag-Streit, Koeniz, Switzerland), which is a combination of a conventional slit lamp biomicroscope, an illumination system and a photo attachment. The illumination system consists of an electronic flash unit and a separate light source for the modelling light. The continuous modelling light is used to show where the light from the flash will fall. The background illumination is provided via a fibre optic cable, which contains two optical fibre bundles, one for the flash illumination and one for the modelling light (figure 1A). The camera used in this study was a Canon EOS 20D (Canon, Tokyo, Japan).

(A) Front view of the slit lamp showing the background illumination cable connected to its holder. (B) The modified digital slit lamp camera system in use during transillumination photography.
The slit lamp camera system was modified by simply loosening the locking screw which secures the distal end of the background illumination cable to its swivel holder in front of the slit lamp (figure 1A), allowing the long, free end of the flexible fibre optic cable to be released and freely moved by the examiner. The flat, smooth tip of the cable was covered with a small piece of sterile, adhesive and transparent polyethylene drape (Steri-Drape, 3M Health Care, St. Paul, Minnesota, USA) in order to protect the fibre optics and maintain sterile conditions during the procedure. Topical anaesthetic (proxymetacaine 0.5%) was then instilled in the patient's eye, the lids were kept open by a Barraquer wire speculum, and the head was positioned on the head and chin rest of the slit lamp. The patient was asked to move the eye in the desired direction, and light was delivered by gently pressing the light fibre tip, which is about 5 mm in diameter, against the surface of the sclera or the cornea for transocular or transpupillary transillumination, respectively (figure 1B). For photographic documentation, the camera was set to 800 ISO, and the background illumination was maximised. The examination room was darkened, and the slit light beam from the slit lamp was turned off. Despite the dim working conditions, the modelling light was sufficient for precise placement of the light fibre tip against the patient's eye and for accurate focusing of the camera. The slit lamp camera was then fired, delivering the flash through the background illumination fibre cable synchronised with the camera shutter. Due to the digital processing, immediate observation and judgement of the captured images were possible.
We have applied this technique to a consecutive series of five patients aged between 43 and 73 years. One patient had a ciliary body melanoma, two had an anterior choroidal melanoma with ciliary body involvement, one had a ciliary body naevus, and one had atrophy of the ciliary body and choroid after episcleral brachytherapy. The study was registered and approved by the Regional Committee for Medical and Health Research Ethics, Western Norway, and followed the official ethics regulations for clinical research.
Results
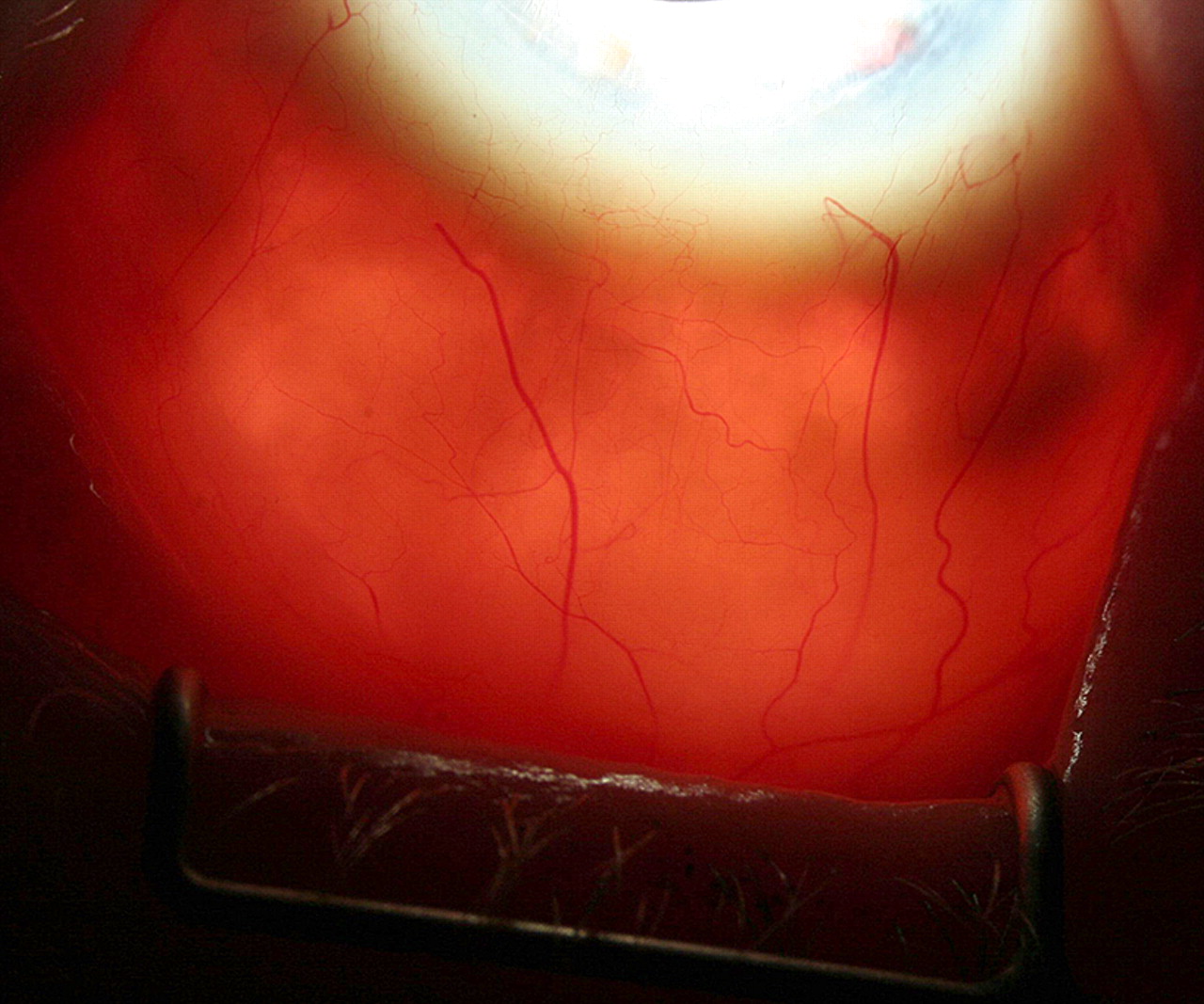
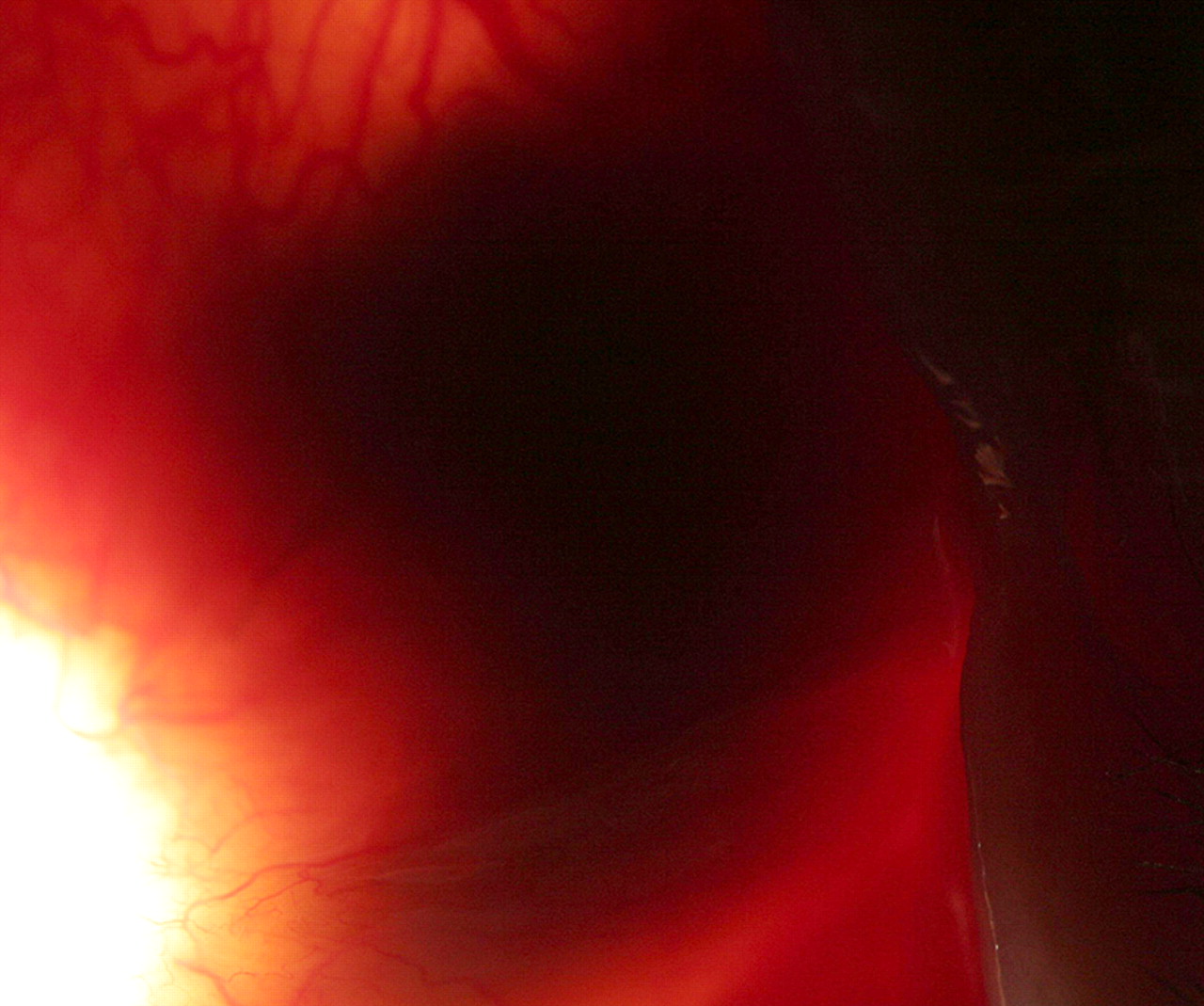
The transillumination photographs were of good diagnostic quality, making it possible to outline the tumour borders and evaluate any ciliary body involvement. Examples of the images are shown in figures 2–5 and demonstrate that they are relatively sharp, revealing the limbus, the ciliary sulcus and the pars plicata of the ciliary body. Most importantly, the high resolution and magnification made it possible to determine the exact location and extent of the tumours in relation to fine landmarks such as conjunctival and episcleral vessels. In one patient, the transillumination photograph was taken 15 years after iodine-125 episcleral brachytherapy for a large ciliary body melanoma, demonstrating complete tumour regression and radiation-induced atrophy of the uveal tissue in the plaque treated area (figure 5). The procedure was easy to carry out in daily clinical practice, and none of the patients experienced discomfort or negative side effects during or after the examination.

Transillumination photograph of a ciliary body melanoma located in the temporal segment of the left eye of a 58-year-old woman. Note the pars plicata of the ciliary body in the upper part of the picture and the fine conjunctival and episcleral vessels between the limbus and the tumour shadow.

Transillumination photograph of an anterior choroidal melanoma with ciliary body involvement in the upper temporal quadrant of the left eye of a 73-year-old woman. Note the episcleral vasculature in the upper part of the picture.

Transillumination photograph of a clinically diagnosed ciliary body naevus located in the temporal segment of the right eye of a 67-year-old woman. The lesion has remained stable in size for many years.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transillumination photograph of the left eye of a 53-year-old woman 15 years after episcleral brachytherapy for a large ciliary body melanoma. The iodine-125 plaque had been positioned between the 5 and 8 o'clock meridians. Note the complete regression of the tumour and the increased transillumination in the plaque-treated area due to radiation-induced uveal atrophy.
Discussion
We have described the modification and use of a conventional digital slit lamp camera system for transillumination photography of intraocular tumours. Our technique offers increased illumination and image resolution by utilising the electronic flash unit and the advanced imaging technology of the system. As this keeps exposure time to a minimum, minor ocular movements do not preclude sharp and accurate images. The procedure is convenient for the patient, easy to repeat and does not require additional equipment. The technique can also be adapted to other slit lamps with a design similar to that of the Haag-Streit type. Furthermore, it has potential for improvements, for instance by attaching a custom made transparent cap to the light fibre tip for better light penetration and focusing abilities.
High quality transillumination images are essential not only for the differential diagnosis of uveal melanoma, but also for the documentation of tumour growth, preoperative planning in episcleral brachytherapy, and follow-up after treatment. We recommend the use of this technique in all cases where transillumination and photographic documentation of intraocular tumours are considered important.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Regional Committee for Medical and Health Research Ethics, Western Norway.
Provenance and peer review Not commissioned; externally peer reviewed.