Article Text

Abstract
Aim To report on the cerebrospinal fluid (CSF) exchange between the intracranial spaces (ie, basal cisterns) and the subarachnoid space (SAS) of the optic nerve (ON) in subjects with normal-tension glaucoma (NTG) compared with control subjects without NTG or other forms of glaucoma.
Methods CT cisternography of the brain and orbits was performed in 18 patients with NTG (7 women, 11 men; mean age 64.9±8.9 years) and in four patients without glaucoma or intracranial disease (4 women; mean age 62.8±18.4 years). The density of contrast-loaded cerebrospinal fluid (CLCSF) in the intracranial spaces and in the SAS surrounding the ONs was measured in Hounsfield units.
Study design Unmasked, prospective series. Statistical analysis was performed using an independent two-tailed t test and the non-parametric Spearman correlation test.
Results The density of CLCSF in the SAS surrounding the ONs in the NTG group was significantly reduced compared with its density in the intracranial CSF spaces and in the SAS of ONs measured in the control group (p=0.006). There were no significant differences between men and women within the NTG group (p>0.35).
Conclusions The finding of a difference in the concentration gradients between the CLCSF within the intracranial spaces and the SAS of the ONs in this group of NTG patients compared with control subjects supports the hypothesis of a disturbed CSF exchange between the CSF in the intracranial spaces and the CSF in the SAS surrounding the ONs. The disturbance of CSF dynamics in this specific CSF pathway can be explained by ON compartmentation. The clinical importance of this finding warrants further investigation.
- Cerebrospinal fluid
- computed cisternography
- normal-tension glaucoma
- subarachnoid space
- translaminar pressure
- anatomy
- physiology
- optic nerve
- pathology
- visual pathway
- diagnostic tests/investigation
- glaucoma
- muscles
Statistics from Altmetric.com
- Cerebrospinal fluid
- computed cisternography
- normal-tension glaucoma
- subarachnoid space
- translaminar pressure
- anatomy
- physiology
- optic nerve
- pathology
- visual pathway
- diagnostic tests/investigation
- glaucoma
- muscles
Introduction
The pathophysiology of normal-tension glaucoma (NTG), a condition characterised by visual field loss and optic disc excavation identical to primary open-angle glaucoma (POAG) despite apparently normal intraocular pressure (IOP), remains poorly understood. Impaired blood flow to the optic nerve (ON) head and vascular dysregulation are thought to be two of the predisposing factors.1 2 Furthermore, there is some evidence that NTG patients have a variety of serological vascular-related abnormalities such as elevated levels of endothelin, a potent vasoconstrictor.1 3 In addition to vascular risk factors, it has been suggested that cerebrospinal fluid (CSF) pressure is a contributing factor to the development of NTG. For example, two recent studies reported lower intracranial pressure (ICP) in NTG patients than in POAG patients.4 5 This finding raised the possibility that axon death in patients with NTG could be due, at least in part, to an imbalance of translaminar pressure, that is, the difference between IOP and pressure in the subarachnoid space (SAS) of the ON. Ren et al reported that the translaminar pressure gradient was significantly higher in both POAG and NTG patients compared with controls.5 In addition, Watanabe et al showed a correlation between ICP and increased ON sheath diameter.6 Using CT scanning, we have found that patients with NTG have increased ON sheath diameters similar to those of patients with increased ICP.7 In the present study, we performed CT cisternography measurements of the contrast density in the SAS of the ONs and compared them with the contrast density of CSF in the basal cisterns of patients with NTG and in subjects without any ON or intracranial disease. Cisternography is a neuroradiological technique used to detect CSF leaks after suspected disruption of the dura mater and can be used to demonstrate CSF flow.8
Patients and methods
The study group consisted of 18 patients (mean age 64.9±8.9 years)—seven women (62.4±8.2 years) and 11 men (66.5±9.4 years)—who were referred by ophthalmologists with the diagnosis of advanced NTG, characterised by progressive visual field loss and an optic disc appearance consistent with POAG but with IOP always <21 mm Hg by Goldmann applanation tonometry. All patients had at least six IOP measurements at different times of the day (between 08:00 and 20:00) in a seated position as well as at night (between 21:00 and 06:00) in a recumbent and supine position using a Perkins hand-held tonometer (Haag-Streit International, Berne, Switzerland). All patients were subjects in another clinical study (‘Normal Tension and Chronic Open Angle Glaucoma and Cerebrospinal Fluid Composition’; NIH clinical trial identifier: NCT00306657) who underwent CT of the brain and orbits combined with cisternography. At the beginning of cisternography, a lumbar puncture was performed that included measurement of ICP with the subject in the lateral decubitus position to confirm CSF pressure ≤20 cm H2O. At the time of lumbar puncture, 10 ml of CSF was obtained for chemical analysis, following which 10 ml of the contrast agent iopamidol (molecular weight 778 D, Iopamiro 300, Bracco, Milano, Italy) was injected intrathecally. The patient was then turned to the prone position. None of the patients were on medication that would influence production or resorption of CSF. A 64-detector scanner (Aquillion 64, Toshiba, Tokyo, Japan) providing 0.5 mm×32 section collimation was used. Scanning parameters were a 25 cm field of view with a 512×512 matrix, and soft tissue and bone reconstruction algorithms were employed. The field of view included the foramen magnum and the nose. Multiplanar reconstruction images were obtained in the axial, coronal and sagittal planes with a 1 mm slice thickness. CT images were analysed on a workstation using the AW (Advantage Workstation) 4.1 software (General Electric, Milwaukee, Wisconsin, USA). Contrast density was measured in Hounsfield units (HU). Measurements were performed intracranially in the basal cisterns (ie, suprasellar and prepontine cisterns) as well as in the SAS surrounding the orbital portion of the ON (figures 1 and 2). To find the site with the highest contrast density, the cursor was moved over the area of interest until the highest HU number was determined. In all patients, the highest measurement in HU from the same location was used to standardise the procedure.
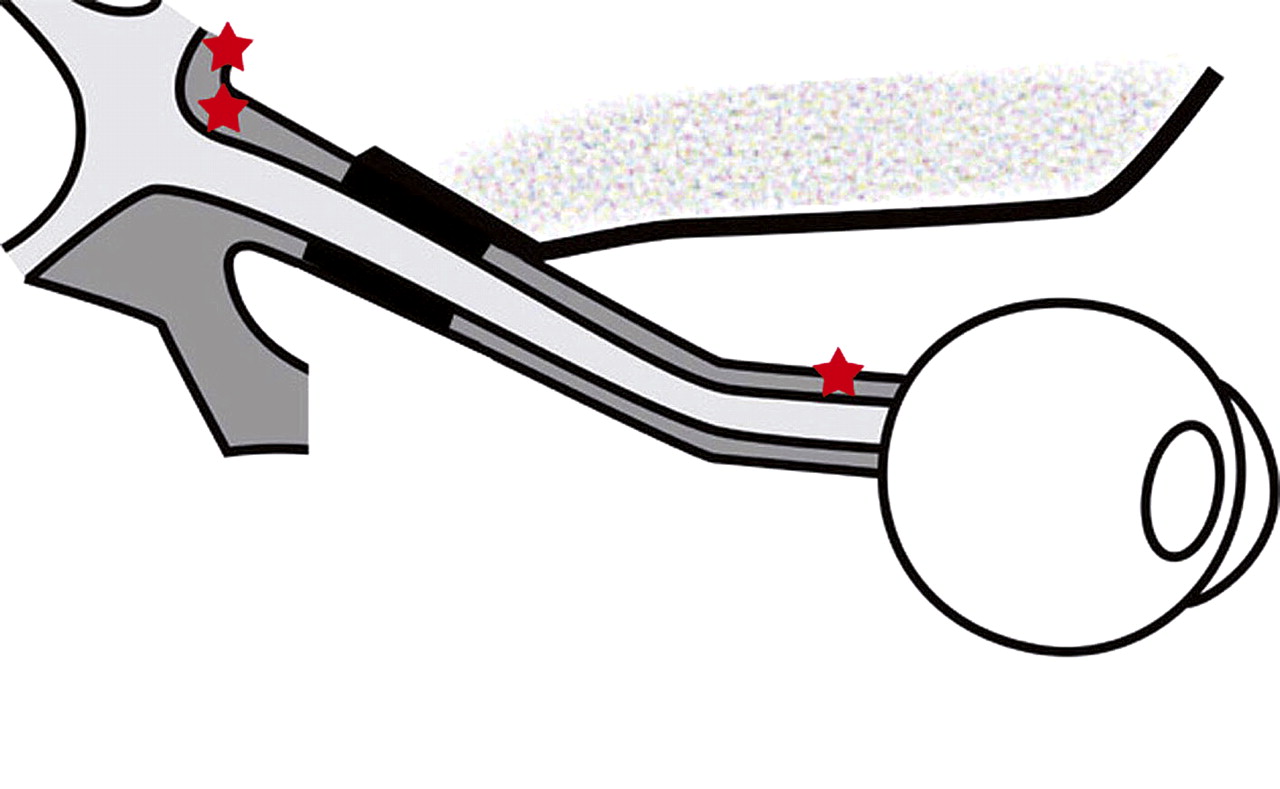
Measurement points for density of contrast-loaded cerebrospinal fluid. Two stars, intracranial (pituitary cistern); one star, bulbar region of the subarachnoid space of the optic nerve.
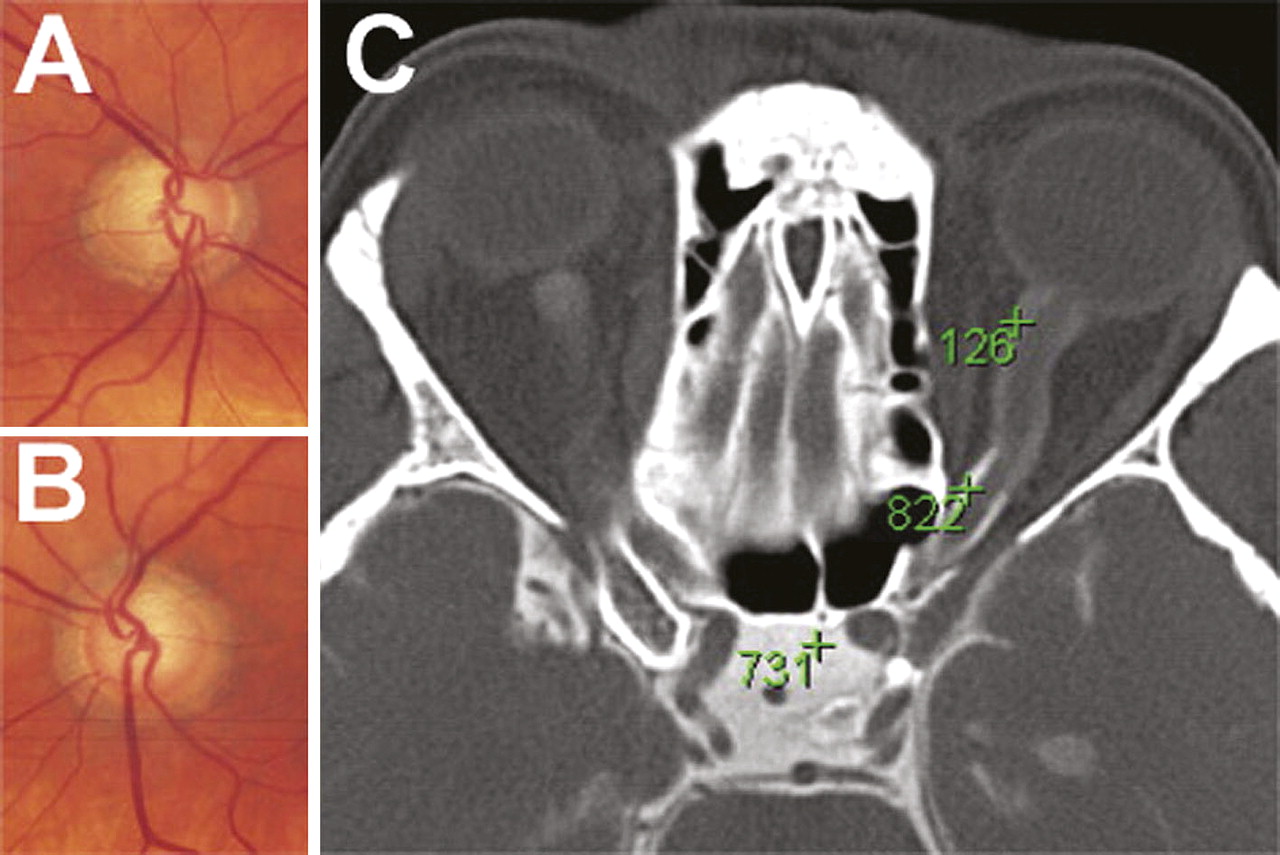
Optic discs of the right (A) and the left (B) optic nerve (ON) of one of the normal-tension glaucoma patients in this study and corresponding cisternography (C). Note the distension of the bulbar region in both ON and the lack of contrast-loaded cerebrospinal fluid (CLCSF) in the distended subarachnoid space. The gradient of CLCSF from the pituitary cistern to the bulbar region of the ON is evident. The numbers represent CLCSF density measurements in Hounsfield units.
Four subjects (mean age 62.8±18.4 years; all women) without known intracranial disease or any form of glaucoma including NTG who also underwent CT cisternography as part of another study served as controls. Measurements of contrast-loaded cerebrospinal fluid (CLCSF) density intracranially and in the SAS surrounding the ONs were obtained in these subjects as described above.
The independent two-tailed t test and the non-parametric Spearman rank order correlation coefficient (SPSS 14.0; SPSS Inc) were used for statistical analysis. This study was designed and performed according to the tenets of the Declaration of Helsinki and was approved by the local ethics committee.
Results
The subjects in the NTG group did not differ significantly in age compared with the four female control subjects with respect to either women (p=0.98) or men (p=0.38). In addition, there was no significant difference in age between women and men with NTG (p=0.35). There was no significant difference in ICP between subjects in the NTG group (mean 13.3±3.5 cm H2O) and the control subjects (mean 13.0±5.7 cm H2O) (p=0.96) or between women and men with NTG (p=0.43) (table 1).
Cerebrospinal fluid dynamics in normal-tension glaucoma patients and controls
CT cisternography
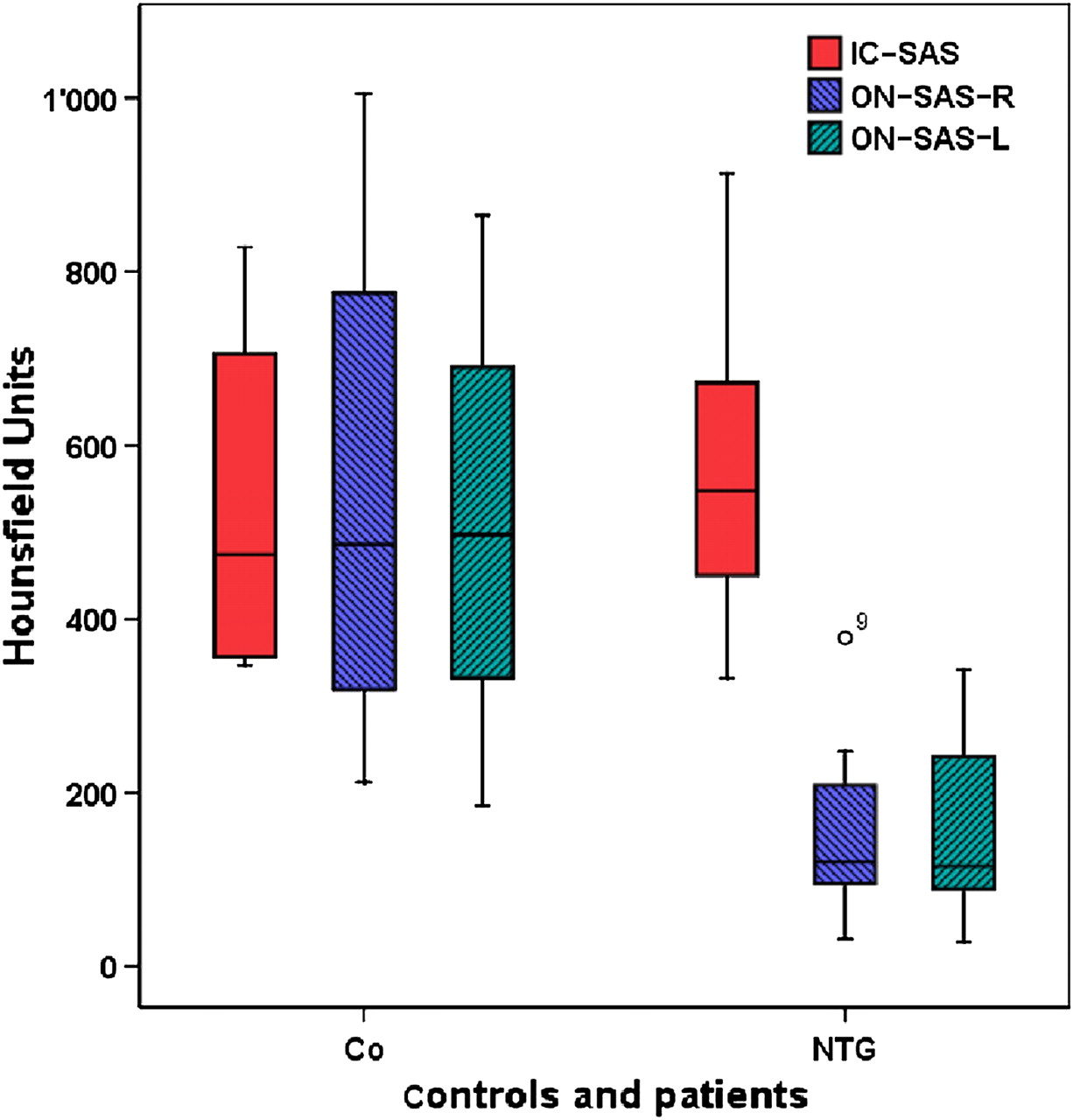
In the eight eyes from the four control subjects, the densities of contrast medium by CT cisternography in the SAS surrounding the ON ranged from 185 to 1005 HU (mean density 529±285.8 HU) and the densities in the basal cisterns ranged from 347 to 828 HU (mean density 531±208.3 HU) (table 1). In the 36 eyes with NTG, densities of contrast medium in the SAS of the ONs ranged from 28 to 378 HU (mean density 144±88.4 HU) and differed significantly from the densities in the control eyes (p=0.006), whereas contrast densities in the basal cisterns of the NTG patients ranged from 332 to 913 HU (mean density 566±166.5 HU) and did not differ significantly from the controls (p=0.67) (table 1, figure 3).

Box-plot of contrast density measurements in Hounsfield units in the basal cistern (IC-SAS) as well as in the subarachnoid space (SAS) of the right (ON-SAS-R) and the left (ON-SAS-L) optic nerve (ON) in four controls (Co), all of whom were women, and 18 normal-tension glaucoma (NTG) patients, showing median and quartiles as well as standard deviation and outlier case (corresponding to case numbers in table 1).
The difference between the measured contrast density in the SAS surrounding the ON (ON-SAS) and the intracranial SAS (IC-SAS) in the basal cisterns was calculated for each case separately. The results revealed a large and highly significant (p<0.0001) difference between the NTG patients (mean difference (ON-SAS–IC-SAS) = −422±192.8 HU) and the control subjects (mean difference = −1.75±146.8 HU (calculated ONSAS – ICSAS in each case for the right ON-SAS and the left ON-SAS separately); median −15).
Discussion
This study of 18 patients with bilateral NTG demonstrates a significantly higher intracranial density of CLCSF in the intracranial spaces (basal cisterns) compared with the density of CLCSF in the SAS surrounding the ON (figure 3). This difference was not present in the small control group without NTG. This finding can be explained by a reduced CSF exchange between the basal cisterns and the SAS surrounding the ON, leading to reduced CSF turnover in the SAS of the ON.
The velocity of CSF flow depends largely on the CSF pressure difference that follows changes of CSF volume due to newly produced CSF. A lower CSF pressure difference will therefore result in a lower CSF velocity (ie, slower propulsion). Several studies in glaucoma patients report a lower lumbar pressure in patients with NTG than in patients with POAG,4 5 whereas a recent study reported a higher lumbar pressure in 17 patients with ocular hypertension compared with control subjects.9
Lower ICP indeed could explain the reduced density of the CLCSF in the SAS of the ONs as demonstrated with cisternography; however, this explanation is inconsistent with our previous finding of increased ON sheath diameters measured in patients with NTG that demonstrate similar diameters as seen in patients with papilloedema.7 10 Based on a concept of continuous CSF pressure and velocity, these findings seem contradictory, as distension of the ON sheath is a typical feature of elevated ICP, not lower ICP.11 This apparent inconsistency can, however, be explained if the concept of continuous CSF flow and pressure is incorrect.12–14
CSF flow is directed from the intracranial spaces (ventricles, basal cisterns) through the optic canals to the SAS of the ONs. Unlike the intracranial CSF spaces, which are basically open spaces, the SAS surrounding the ON contains numerous trabeculae and septae that reduce both CSF volume and CSF flow. In addition, the SAS of the ON (including the trabeculae and septae) is lined with meningothelial cells (MECs).15 These cells, which have a major role in the metabolic status of the CSF are more abundant in patients with POAG than in normal subjects.16 In addition, an in vitro study from our laboratory demonstrated MEC proliferation of up to 20% when MECs were submitted to extrinsic increased pressure.17 Furthermore, in a sheep model, these cells were noted to enlarge when flow through the SAS of the ON was restricted with gentle ligation of the ON.18 It thus may be postulated that an increase in both the number and volume of MECs results in narrowing of the SAS surrounding the ONs thus increasing the resistance to the flow of CSF from the basal cisterns.
A recent study of 10 patients with normal-pressure hydrocephalus described a close relationship between the lumbar pressure and the intraparenchymal pressure of the brain19; however, the findings were not compared with those from a group of age- and gender-matched normal subjects. In addition, the parenchymal pressure rather than the ventricular pressure was measured, and because of the different compliances of the brain parenchyma and the ventricular wall, a linear relationship may not be present. Indeed, the authors themselves noted that their assumption that lumbar pressure equals ICP is only correct if the CSF flow throughout these regions is continuous—an assumption for which there are no data.19 In fact, a recent study on patients with papilloedema would seem to contradict this assumption.10
Even if lumbar pressure were to equal ventricular pressure, the question still remains whether or not this relationship can be extrapolated to the SAS surrounding the ON. There are several sound reasons to doubt such a relationship. First, the volumes of the ventricles and the SAS surrounding the ON are very different. Second, the anatomy within the SAS surrounding the ON is sufficiently different from the anatomy within the ventricles to allow a simple extrapolation of pressure from one region to the other. The fact that CLCSF density in the SAS surrounding the ON is reduced in our patients with NTG together with the dilation of the retrobulbar portion of the ON as we have reported previously,7 suggests that this region can develop into a compartment with a different CSF composition, different CSF dynamics and probably a different pressure in patients with NTG compared with otherwise normal individuals, much as is the case in patients with papilloedema.10
Finally, patients with papilloedema demonstrate an increased concentration of lipocalin-like prostaglandin D synthase (L-PGDS) in the SAS surrounding the ON compared with its concentration in the spinal CSF.10 20 L-PGDS plays a significant role in the metabolism and health of the central nervous system. Indeed, elevated concentrations of L-PGDS demonstrate damage to astrocytes as well as diminished ATP production in an in vitro model.21 Given the large molecular weight of this protein (26 kD), it is feasible that the presence of such a large molecule in such a small perioptic space prevents the influx of smaller molecules, such as iopamidol (778 D). The presence of a large and potentially harmful molecule as L-PGDS could at least partly explain the absence of CLCSF in the perioptic space in our patients (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Possible distribution of iopamidol (778 D; large dots) and β-trace protein (lipocalin-like prostaglandin D synthase) (26 kD) in the subarachnoid space of the optic nerve. β-trace protein (large dots) blocking the influx of contrast-loaded cerebrospinal fluid (CLCSF) due to its large molecular size.
We acknowledge that the results of this study do not explain the entire complex pathophysiology of NTG, but none of the present hypotheses on the pathophysiology of NTG does so. In fact, it may very well be that NTG is not a separate entity from open-angle glaucoma at all.22 Nevertheless, based on the present study, which demonstrates impaired circulation of CSF in a probably compartmented SAS of the ON in patients with NTG, we believe it important to consider the possibility of a detrimental effect of CSF stasis on axons and glial cells of the ON similar to that which may occur in patients with normal-pressure hydrocephalus.23 The high recycle rate as well as the impressive proteome of CSF indicates its importance for the biochemical milieu of neurons, glial cells and axons as well as its role as a transport system for clearing the CSF of toxic metabolites and other substances that may damage the various components of the ON (eg, stasis of CSF is thought to be associated with dementia).24 An obvious weakness of this study is the paucity of normal controls. Because cisternography is an invasive procedure and because its use for experimental purposes in control subjects is extremely limited for safety reasons, it is difficult to recruit normal subjects. In addition, as the control subjects had an unexplained ON disease that probably might be explained on the basis of a vascular aetiology, it is conceivable that the results are not truly those of normal individuals. In contrast to our small control group the NTG patients represent a population with ‘chronic and progressive’ ON disease and the change in CSF exchange might therefore reflect the impact of chronicity. Although we do not have the proper controls (normal subjects), we have the laws of physics, such as the second low of thermodynamics. And these laws tell us that the CLCSF should distribute homogeneously in an open system. Further studies should be performed to confirm or exclude the role of CSF composition and flow in the ONs of patients with NTG.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the ethical committee of the hospital and the local government—Kantonales Ethikkommittee Aargau.
Provenance and peer review Not commissioned; externally peer reviewed.