Article Text

Abstract
Aims To determine the prevalence of glaucoma within the indigenous Australian population living in central Australia.
Methods 1884 individuals aged ≥20 years, living in one of 30 remote communities within the statistical local area of ‘Central Australia,’ were recruited for this study. This equated to 36% of those aged ≥20 years and 67% of those aged ≥40 years within this district. Slit-lamp examination of the anterior segment and intraocular pressure measurement, followed by stereoscopic slit-lamp funduscopy of the optic nerve, was performed. Selected patients underwent automated visual-field testing. The diagnosis of glaucoma was based on pre-existing definitions. Glaucoma prevalence data are presented.
Results Seventeen individuals had glaucoma (0.90%). Causes of secondary glaucoma were found in four with neovascular glaucoma, two with uveitic glaucoma and four who had developed glaucoma subsequent to trauma or surgery. The remaining seven had no identifiable cause for their glaucoma and were thus classified as open-angle glaucoma equating to a prevalence of 0.52% (95% CI 0.14% to 0.90%) for those aged ≥40 years. Of these, four had an intraocular pressure ≤21 mm Hg, and three had an intraocular pressure >21 mm Hg.
Conclusion The prevalence of open-angle glaucoma among indigenous Australians within central Australia was 0.52% for those aged ≥40 years. After adjustment for the age distribution of our sample, this is one-third the prevalence seen among the non-indigenous Australian population and is despite a higher prevalence of ocular parameters considered to be associated with glaucoma.
- Indigenous Australians
- remote Australia
- glaucoma
- prevalence, epidemiology
Statistics from Altmetric.com
Glaucoma is a major cause of blindness worldwide.1 In Australia, glaucoma is the second most common cause of blindness after age-related macular degeneration.2 It increases in prevalence with age3–5 and shows a strong association with a known family history of glaucoma5–7 and the presence of ocular conditions such as pseudoexfoliation syndrome (XFS)8 or pigment dispersion syndrome.9 The prevalence of open-angle glaucoma (OAG) varies considerably among different racial groups, occurring in 2.1% of white populations, 1.4% of Asian populations and 4.2% of black populations for those aged 40 years and older.10
Within the non-indigenous Australian population, the prevalence of OAG been estimated at 1.7% of those aged 40 years3 or older and 3.0% of those aged 49 years or older.4 However, indigenous Australians have been felt to have a much lower prevalence,11 with previous work performed by the National Trachoma and Eye Health Project in the 1970s finding a rate of only 0.4% among those aged 40 years or older.12 This is despite other studies finding a high frequency of XFS,12 13 thinner central corneal thickness (CCT)14 15 and larger optic discs and cup/disc ratios16 17 among indigenous Australians.
During the Central Australian Ocular Health Study, we aimed to perform a comprehensive enumeration of the current ocular morbidity among indigenous Australians living within central Australia. This paper was designed to determine the prevalence and subtypes of glaucoma within this population.
Methods
The Central Australian Ocular Health Study took place in 30 remote communities within the statistical local area of ‘central Australia,’ excluding those living in and around the city of Alice Springs (figure 1). Clinics were held at each of these communities a total of once or twice per year, depending on the population of the community. Given the length of time between each of these clinics, the health workers in the communities would actively encourage every resident to attend the clinics regardless of their symptoms.

Schematic map of the central Australian statistical local area. ▲, communities visited during the study.
Patients were recruited from those who identified themselves as indigenous Australians, presenting to the remote clinics at each of these communities during the 36-month period between July 2005 and June 2008. Ethical approval from the Central Australian Human Research Ethics Committee was obtained and conformed to the tenets of the Declaration of Helsinki. The aims of the study were explained, with an interpreter whenever necessary, and written informed consent was obtained. Data were entered on a standardised form which had been constructed prior to the commencement of the study. All data collection was performed under the supervision of one of two experienced consultant ophthalmologists.
Following visual acuity testing using a tumbling E acuity chart at 3 m in a well-lit room, intraocular pressure was performed using either a Perkins tonometer (Haag-Streit, Koeniz, Switzerland) or an ICare tonometer (Tiolat Oy, Helsinki, Finland) depending on the availability of equipment. A slit-lamp examination of the anterior segment was performed, followed by a pupil examination performed with a hand torch. An assessment of the anterior chamber depth was then made using the ‘oblique flashlight test’18; however, a gonioscopy was not performed. The pupils were dilated with tropicamide 1.0% and phenylephrine 2.5%, unless the anterior chamber was found to be shallow, in which case only tropicamide 1.0% was used. The anterior surface of the lens capsule was examined for the presence of XFS, followed by an examination of the lens with grading using the modified Lens Opacities Classification System III.19 Finally, stereoscopic slit-lamp funduscopy of the optic nerve, the posterior pole and the peripheral retina was performed using a 90 D funduscopy lens. If indicated based on clinical suspicion of glaucoma, visual-field testing was performed using either a screening C20-1 algorithm on a Frequency Doubling Perimeter (FDP) (Carl Zeiss, Dublin, California), or an SITA-fast algorithm (Swedish Interactive Thresholding Algorithm) on a Humphrey Field Analyzer II (HFA) (Carl Zeiss, Dublin, California). A field was considered unreliable if false-positive errors, false-negative errors or fixation losses were greater than 33%.20 An abnormal field using FDP was one in which there were two or more adjacent non-central abnormal zones of p<1% or worse, with at least two zones of p<1% or worse, or one zone of p<0.5% or worse touching the horizontal nasal meridian.21 22 Visual-field loss was considered significant on the HFA if it had a pattern typical of glaucoma and occurred in a field with five or more non-rim points of p<5%, with a cluster in a nasal quadrant of at least three abnormal points of p<5%, or at least two points of p<1%.3
The presence of glaucoma was defined under the guidelines according to Foster et al.23 Owing to the logistics of ocular healthcare delivery to this remote area, a visual-field perimeter was not available on a number of occasions. Therefore, case identification was undertaken in the following way (figure 2). Participants were examined for the presence the neuroretinal rim width reduced to <0.1 Cup/Disc Ratio (CDR) (between 11 and 1 o'clock or between 5 and 7 o'clock) or the presence of a CDR ≥97.5th percentile.23 This equated to ≥0.7 owing to the large vertical disc size and consequently large CDR possessed by indigenous Australians.16 When present, the participant was considered for a visual-field test. When this was possible, the participant was then assessed under category 1 criteria (disc criteria as above and a definite visual-field defect consistent with glaucoma). When perimetry was not possible, glaucoma was considered to be present if category 2 criteria were fulfilled (CDR ≥99.5th percentile (ie, ≥0.8)16 in the absence of any other explanation) or if category 3 criteria were fulfilled when disc assessment was not possible (visual acuity <3/60 and IOP >99.5th percentile (24 mm Hg),24 or visual acuity <3/60 and the eye shows evidence of glaucoma filtering surgery, or medical records confirm glaucoma).

Diagnostic algorithm used to define glaucoma. CDR, Cup/Disc Ratio; IOP, intraocular pressure; VA, visual acuity.
Finally, we presented data regarding those who were considered to be glaucoma suspects,23 which were defined as: those with a CDR ≥0.7 but <0.8 who either had no visual-field loss or did not undergo visual-field testing, those with optic disc margin haemorrhages in the presence of a normal optic disc and normal IOP, those with an IOP >97.5th percentile (21 mm Hg),24 those with XFS and those with a positive oblique flashlight test but normal optic disc, visual field and IOP.
Based on previous work,14 16 25 which established the likely demographics of patients presenting to the remote clinics and the likely prevalence of ocular disorders,12 our aim was to enrol at least 1850 patients aged 20 years or older into the study, in order to ensure that at least 1200 patients aged 40 years or older were enrolled. This would allow the detection of the least prevalent major ocular disorder (glaucoma) at an expected prevalence of 0.4%.12
Statistical Analysis System 9.1 was used for statistical analysis including descriptive statistics, Student t test and logistic regression. Age was considered as a continuous variable. The presence of a positive oblique flashlight test, sex, diabetes and hypertension were considered as categorical variables. Test statistics, 95% CIs and p values are presented. CIs for prevalence estimates were derived using a normal approximation interval of a binomial distribution. A p value of <0.05 was considered statistically significant.
Results
From the 5173 persons who were in the target population, we recruited 1884 during the 36-month period of the study. This included 689 (36.6%) males and 1195 (63.4%) females, whose average ages were 49 years (SD 14 years) for males and 48 years (SD 15 years) for females (t=1.58; p=0.11). This represented 36% (1884/5173) of the total and 67% (1347/2014) of those aged 40 years and older.
One thousand three hundred and ninety-four patients underwent optic disc assessment and were assessed under category 1 and 2 criteria, and 490 patients could not undergo optic disc assessment owing to media opacity and therefore were assessed under category 3 criteria (figure 2). Twenty-four of these could not have their anterior chambers assessed due to enucleation, phthisis or severe corneal scarring.
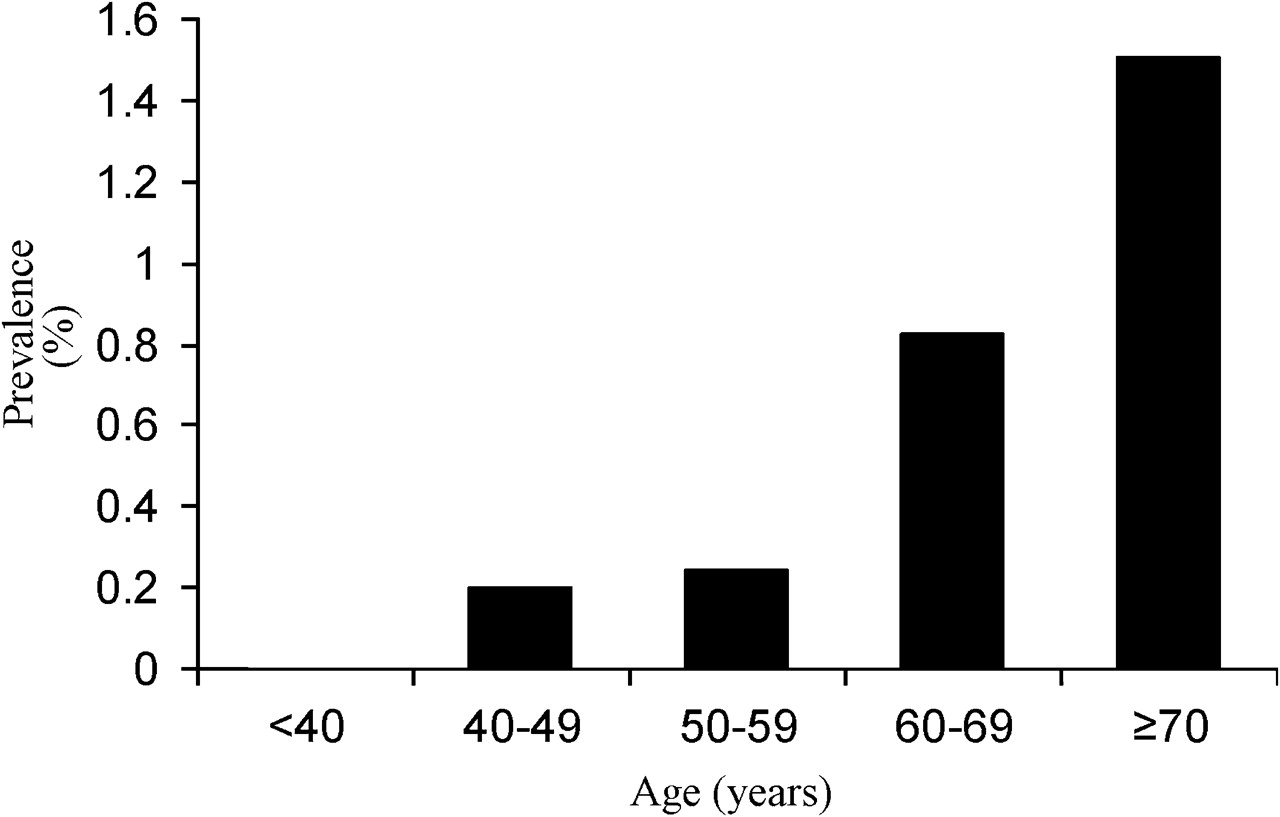
From the total, there were 17 patients (0.90%, 95% CI 0.40 to 1.20) who had glaucoma, and 15 of those were aged 40 years or older (1.11%, 95% CI 0.55 to 1.67). The 17 patients included four with neovascular glaucoma, two with uveitic glaucoma and four who had developed glaucoma subsequent to trauma or surgery. The remaining seven from the original sample of 1884 (0.37%) had no identifiable cause for their glaucoma including a negative oblique flashlight test, equating to a prevalence of OAG of 0.52% (95% CI 0.14% to 0.90%)(7/1347) for those aged 40 years or older (figure 3). After adjusting for the age distribution of our sample, the prevalence of OAG varied from 0.57% (95% CI 0.17% to 0.97%)3 to 1.01% (95% CI 0.36% to 1.66%)4 depending on the non-indigenous Australian population used in the comparison. Of those who had OAG, four had an IOP ≤21 mm Hg, and three had an IOP >21 mm Hg. Four were female, and three were male. There was an increase in prevalence of OAG with increasing age (figure 4).
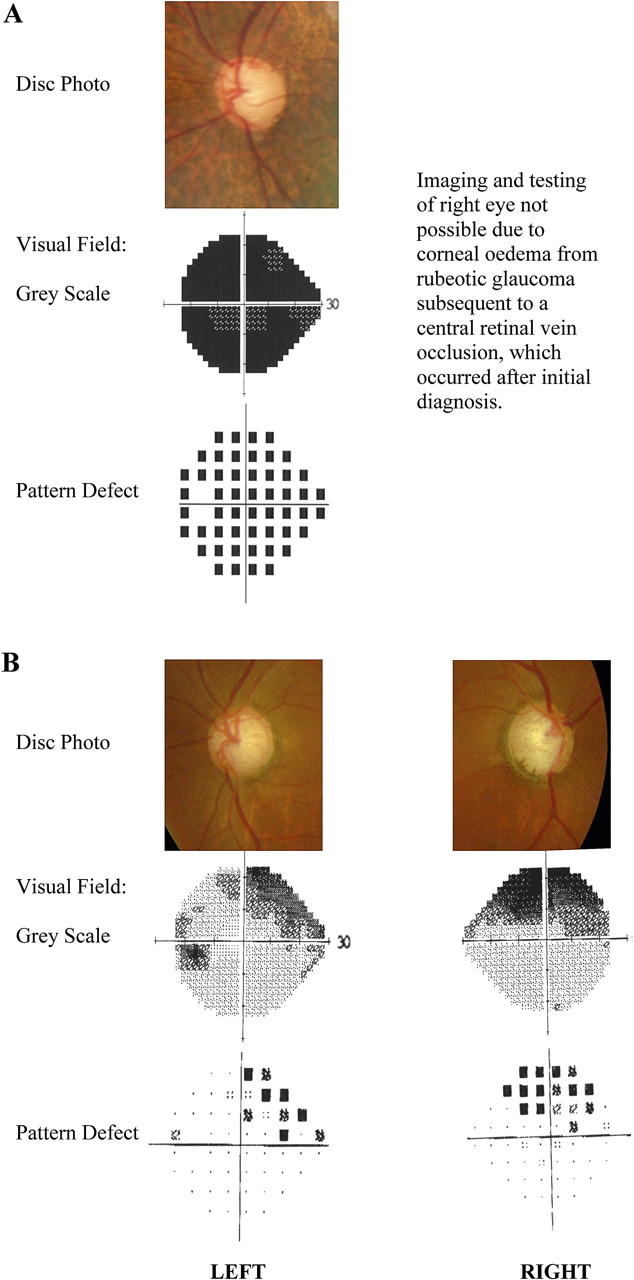
Sample patients A and B who were found to have open-angle glaucoma.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of open-angle glaucoma by age.
There were 137 patients who were considered glaucoma suspects. These included 28 with CDR ≥0.7 but <0.8 with no definite signs of glaucoma and an IOP <21 mm Hg, 71 with XFS but with an IOP <21mm Hg and a normal optic nerve, 14 with an IOP >24 mm Hg but no glaucomatous optic neuropathy, one patient with a disc margin haemorrhage but an IOP of 13 mm Hg and a CDR of 0.4 and one patient with XFS and a CDR of 0.7 without focal changes consistent with glaucoma and an IOP of 12 mm Hg. Furthermore, we found 22 (1.3%) patients with a positive oblique flash-light test in one or both eyes (1.7% of those aged 40 years or older), but without any evidence of raised IOP or glaucomatous optic neuropathy. The prevalence of a positive oblique flashlight test increased with advancing age, although this did not reach statistical significance (t=1.68; p=0.09). Furthermore, the presence of a positive oblique flashlight test was not associated with sex, diabetes or hypertension.
Discussion
Glaucoma is a condition which is seen to affect all populations around the world. However, its prevalence can vary widely between racial groups. Among non-indigenous Australians, the prevalence of OAG has been estimated at between 1.7%3 and 3.0%.4 We found a prevalence of glaucoma among indigenous Australians of 0.52%. After adjustment for the age distribution of our sample, this increased marginally to 0.57% (for those ≥40 years old) when the Vision Impairment Study3 was used in the comparison and 1.01% (for those ≥49 years old) when the Blue Mountains Eye Study4 was used. This equates to one-third of the prevalence found among non-indigenous Australians and is similar in magnitude to the rates of 0.4% for indigenous Australians and 1.5% for non-indigenous Australians found by the National Trachoma and Eye Health Project.12
These findings are significant for a number of reasons. The variation in prevalence of glaucoma between different races has been hypothesised to be caused by risk factors associated with glaucoma, such as CCT,26 optic disc size or CDR27 28 and XFS.8 However, given that indigenous Australians' CCT is significantly thinner than other racial groups,16 17 their optic disc size is significantly larger than that of other racial groups,14 15 and XFS is significantly more prevalent than other racial groups,12 13 these factors would predict a significantly greater prevalence of glaucoma. However, if we were to assume that these risk factors did not contribute to the variation in OAG prevalence between races, then it may be that other genetic or possibly environmental factors have exerted a protective effect on indigenous Australians. This may be demonstrated by a direct comparison of genetic profiles between groups of indigenous Australians, Caucasians and black Africans.
Our study is limited by the method through which the sample was recruited. As patients need to voluntarily present to an eye clinic, there is the potential that the prevalence of ocular disorders within this sample may be over-represented. However, visits to these remote communities occurred only once or twice per year; therefore the health workers in the communities would actively encourage every resident to attend the clinics regardless of their symptoms. The majority presented for a ‘check-up’ and not due to symptoms; therefore the data collected should reflect the current prevalence of glaucoma within this indigenous population. As males are less likely to present to a health professional,29 almost twice as many females as males were recruited. This phenomenon has been observed in previous work involving non-indigenous populations,30 and there is evidence that it may translate to the indigenous Australian population.31 32 However, glaucoma was not associated with sex, so this gender imbalance that decreased in older age groups should not have affected our results. We collected data on 36% of the population within the central Australian statistical subdivision who were aged 20 years or older, and this recruitment increased with age, such that 67% of those aged 40 years or older were included. Although glaucoma was associated with advancing age, we feel that estimates of visual impairment among those aged 40 years or older should reflect the true prevalence of visual impairment within this age group. Our work was based on the findings from two different tonometers (an ICare tonometer and a Perkins tonometer), which may have affected the results. The selection of a tonometer was based on the availability of the equipment in the remote locations and was not dependent on any aspect of the patient. ICare rebound tonometry has been validated as a good and reliable alternative to applanation tonometry; however, it has been reported in some studies to measure a higher IOP reading, with the average overestimation being up to 2.0 mm Hg (SD 3.0).33–39 Despite this, we found no statistically significant difference between the readings from the group measured with Perkins tonometry compared with those from the group measured with ICare tonometry.24 Ideally, all patients should have had perimetry. Those who underwent visual-field testing were assessed under category 1 criteria, among which 20% (3/17) were found to have glaucoma (figure 2). However, there was a group for whom perimetry was not possible, and these patients were assessed under category 2 criteria. Among this second group, 27% (10/37) were found to have glaucoma (figure 2), although given the results from those assessed under category 1 criteria, we might have expected only 20% of the second group (7/37) to have been diagnosed as having glaucoma, had they also undergone visual-field testing. Therefore, had perimetry been possible for all patients, the prevalence estimate of glaucoma might have been less. It is possible that those assessed under category 3 criteria had only ocular hypertension and not glaucoma, thereby resulting in a total prevalence for glaucoma of only 0.69% (95% CI 0.32% to 1.06%), although we feel this was unlikely given that these patients had either rubeosis or penetrating trauma with an IOP ranging from 31 to 47 mm Hg. A gonioscopy was not performed, but we used the oblique flashlight test to exclude those with occludable anterior chamber angles.18 Although we found a positive flashlight test in 1.7% of individuals, none of these had any form of glaucoma. This test has been reported to have a negative predictive value of between 94% and 98% for the detection of occludable angles (at least three quadrants where the posterior trabecular meshwork is obscured),40 41 and thus those found to have a negative flashlight test would have been unlikely to have had angle closure. Lastly, the estimation of CDR was determined clinically. We had performed a pilot study prior to this survey in order to determine the likely range of CDR and inform the clinicians about the expected appearance of optic discs among this population.16 Furthermore, all data collection was performed under the supervision of one of two experienced consultant ophthalmologists, which would have minimised interobserver error.
We have found that the prevalence of OAG for indigenous Australians was between one-third and one-quarter the prevalence of that found within the non-indigenous Australian population. This was despite the sample having ocular parameters which are considered to be associated with a higher risk of glaucoma (ie, XFS, thinner CCT and larger optic disc size and CDR). Other as-yet unidentified genetic or environmental factors may be protective for the development of glaucoma among indigenous Australians.
Acknowledgments
We would like to thank R Raju, S Wearne, K Billing, T Gray, I Patel, JJ Khong, J Chang, S Durkin and D Parker, without whom this project would not be possible. We would also like to thank V Davies and S Ford, for their support.
References
Footnotes
Funding Partial equipment grants for the study were received from the Ophthalmic Research Institute of Australia: B & L Lowe Grant and NH&MRC: Centre for Clinical Research Excellence.
Competing interests None.
Ethics approval Ethics approval was provided by the Ethical approval from the Central Australian Human Research Ethics Committee was obtained and conformed to the tenets of the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.